

Abstract
AIM: To explore the dynamic changes in the pressure of the lateral ventricle during acute brainstem hemorrhage and the changes of neural discharge of vagus nerve under the load of intracranial hypertension, so as to analyze their effects on the congestive degree of intestinal mucous membrane and the morphologic changes of intestinal mucous membrane.
METHODS: An operation was made to open the skull to obtain an acute brainstem hemorrhage animal model. Microcirculatory microscope photography device and video recording system were used to determine the changes continuously in the caliber of jejunal mesenteric artery during brainstem hemorrhage and the changes with time in the congestion of jejunal mucosal villi. We used HE stain morphology to analyze the changes of duodenal mucosal villi. A recording electrode was used to calculate and measure the electric discharge activities of cervical vagus nerve.
RESULTS: (1) We observed that the pressure of lateral cerebral ventricle increased transiently during acute brainstem hemorrhage; (2) The caliber of the jejunal mesenteric artery increased during brainstem hemorrhage. Analysis of red color coordinate values indicated transient increase in the congestion of jejunal mucous membrane during acute brainstem hemorrhage; (3) Through the analysis of the pathologic slice, we found enlarged blood vessels, stagnant blood, and transudatory red blood cells in the duodenal submucous layer; (4) Electric discharge of vagus nerve increased and sporadic hemorrhage spots occurred in duodenal mucous and submucous layer, when the lateral ventricle was under pressure.
CONCLUSION: Brainstem hemorrhage could cause intracranial hypertension, which would increase the neural discharge of vagus nerve and cause the transient congestion of jejunal mucous membrane. It could cause hyperemia and diffused hemorrhage in the duodenal submucous layer 48 h after brainstem hemorrhage.
Keywords: Brainstem hemorrhage, Irritable changes, Alvine mucous membrane
INTRODUCTION
The normal function of gastric juice is to digest food, but it can cause ulcer through digesting the gastric and duodenal mucosa. Gastric juice contains hydrochloric acid, which is a strong acid with pH1.0. Hydrochloric acid can prevent bacteria from breeding in stomach. The gastric mucosa is covered with the mucus of gastric juice, which can prevent the gastric mucosa from being digested. If the gastric mucosa was directly digested by gastric juice, the mucosa can be injured. Under stress, the discharge of sympathetic nerve and parasympathetic nerve will change, which will cause changes in gastrointestinal motility, the secretion of gastric juice, the mucosa blood stream, all of which are reasons that cause the stress ulcer[1,2]. Usually, the meaning of stress is emotional, such as agitation, anger, etc., under the irritable environmental conditions breakthrough. They evoke the changes of the neural discharge of autonomic nerve[3]. The stress conditions in our experiment is brainstem hemorrhage[4-6].The recovery of brainstem hemorrhage in different part and extent has significant variation, which is determined by the complex anatomic structure of brainstem[2,7-10]. The reticular formations of brainstem have many neurons, which are related to visceral activities. It was reported recently that the injury of the brainstem could cause a high incidence rate of stomach mucosa hemorrhage[11,12]. Some literatures also reported that the proportion of midbrain hemorrhage in brainstem hemorrhage was 28%, which is higher than 10 years ago[13]. The recovery of brainstem hemorrhage is related not only with the hematoma, but also with the body conditions and complications of the patient[14]. Fatality rate is high in a man who has the complications of stress digestive tract ulcer with hemorrhages. The pathogenesis of digestive tract stress ulcer bleeding, induced by brainstem hemorrhage, was thought as the nerve and body fluid factors acting on the gastric mucosa[4]. The changes of vagus nerve discharge during acute brainstem hemorrhage are not clear. The aim of this research was to probe into the influence of brainstem hemorrhage on the intestinal mucous, the microcirculation of the mesentery, the regularity of the electric discharge of vagus nerve with the changes of intracranial pressure under brainstem hemorrhage at midbrain level, in order to guide the early diagnosis and treatment of brainstem hemorrhage complicated with digestive tract stress ulcer bleeding[12,15-19].
MATERIALS AND METHODS
Fifty male Japanese white rabbits with long ears (weighing 1.5-1.8 kg) were employed. Thirty rabbits of one group were used to observe the changes in the pressure of lateral cerebral ventricle and the blood stream of the duodenal mucosa and the jejunal mucosa, under the acute brainstem hemorrhage. The other 20 rabbits were used to analyze the changes of neural discharge of vagus nerves under the intracranial hypertension (36 mmHg, 1 min). Urethane 25% was used for intravenous anesthesia[20]. An operation was made to open the skull at interparietal bone and 0.1 mL blood of itself was injected into its brainstem to make the acute brainstem hemorrhage animal model at the level of inferior colliculus[21]. The hematoma was confirmed to compress the aqueduct of midbrain through the general dissection. Right lateral cerebral ventricle intubation was employed to calculate and measure the dynamic pressure, before and after the load of acute brainstem hemorrhage. We used the recording electrode to calculate and measure the changes of neural discharge of cervical vagus nerve under the intracranial hypertension (36 mmHg, 1 min). We used the software of the device, manufactured in Chengdu device factory, RM6204B organism signal acquisition processing system to measure the absolute value of an area of the nerve discharge activities wave[22]. Through the absolute value of an area of the wave, we could analyze the intensity of the nerve electric activities. By setting a single liminal value line to analyze the frequency of wave in each time segment, we could analyze the electric activities’ intensity indirectly. Microcirculatory microscope photography device and video recording system were used to determine the changes continuously in the caliber of jejunal mesenteric mini-artery and the changes with time in the congestion of jejunal mucosal and duodenal mucosa during brainstem hemorrhage[11] (microcirculatory image process system, made in Optic Instrument General Factory of Xuzhou). The duodenal biopsies of normal and 12, 24, 48, 72 h after brainstem hemorrhage were taken, and fixed with 20% formalin, HE stained. We observed the morphologic changes of mucous layer and submucous layer under light microscope and oil immersion objective (magnification ×1500).
We used paired t-test for statistical method-dependent samples. P<0.05 was considered significant.
RESULTS
(1) We observed a stationary baseline wave (about 9 mmHg) through lateral ventricle intubation, and intracranial pressure increased rapidly after acute brainstem hemorrhage animal model was made, which recovered subsequently, but the pressure level was still higher than it was loaded before (Figure 1); (2) The caliber of jejunal mesenteric artery increased after the load of brainstem hemorrhage. Statistical analysis showed a significant difference between pre-loaded and loaded brainstem hemorrhage (Figure 2); we also observed that the occurrence time sequence of mesenteric artery caliber dilation had individual difference. We analyzed the congestion of jejunal mucosa in acute brainstem hemorrhage by red color coordinate values, then we observed that the congestion increased transiently during 30 s after the load of hemorrhage (Figures 3A-D). The analysis of paired t-test for dependent samples showed that the increasing tendency was significant (Figure 4), and the time sequence of the phenomenon above had the individual difference; (3) We analyzed the intensity of the nerve electric activities through the absolute value of an area of the wave. We also analyzed the discharge activities’ intensity indirectly by setting a single liminal value line to calculate the frequency of dischargeable wave in each time segment (Figures 5A-C). We observed that the neural discharge of vagus nerve increased after intracranial hypertension; (4) Comparing the pathologic slice of duodenal mucous membrane between normal and 48 h after brainstem hemorrhage, we observed that the duodenal submucous layer in normal rabbits did not have dilated minute blood vessel and red blood cells leaked out from capillary lumens to tissue space basically (Figure 6A, B). Analyzing rabbit’s duodenum pathological slices that are 48 h after brainstem hemorrhage, we found that capillaries dilated in duodenal villi and duodenal glands, red blood cells increased in lumens and leaked out from capillary lumens to tissue space in local submucous layer (Figures 6C, D).
Figure 1.
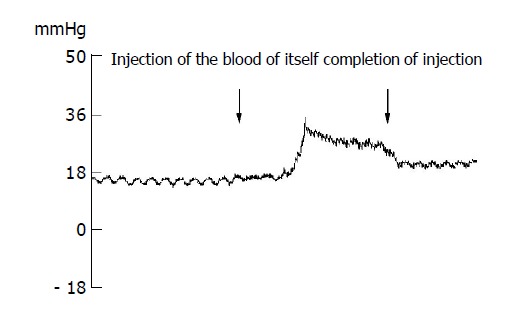
Changes in the pressure of the lateral ventricle during acute brainstem hemorrhage in rabbit.
Figure 2.
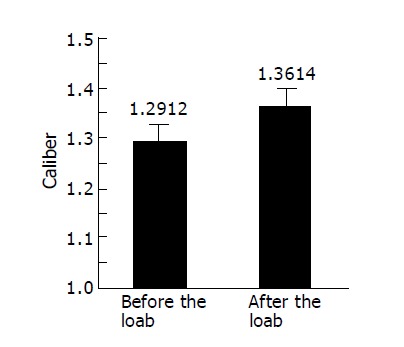
Changes in caliber of jejunal mesentery small vessels under the load of rabbit’s brainstem hemorrhage.
Figure 3.
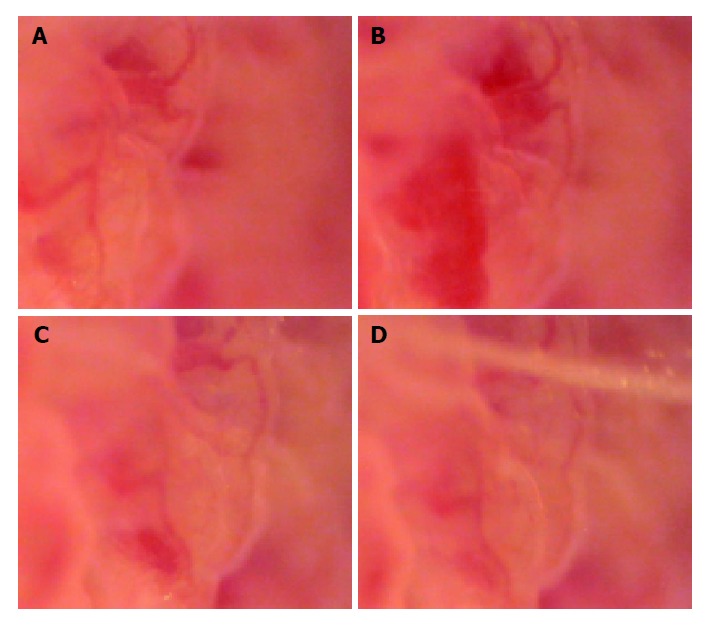
Changes of microcirculation of jejunal mucosa. A: Photograph of microcirculation of jejunal mucous membrane, 6 s before the load of rabbit’s brainstem hemorrhage (×185); B: Photograph of jejunal mucous membrane, 10 min 26 s after the load of rabbit’s brainstem hemorrhage; it showed the local congestion of villus mucosa (×185); C: Photograph of jejunal mucous membrane, 30 min 32 s after the load of rabbit’s brainstem hemorrhage; it showed that the local congestion of villus mucosa had relieved (×185); D: Photograph of jejunal mucous membrane, 40 min 46 s after the load of rabbit’s brainstem hemorrhage; it showed that the local congestion of villus mucosa had ameliorated obviously (×185).
Figure 4.
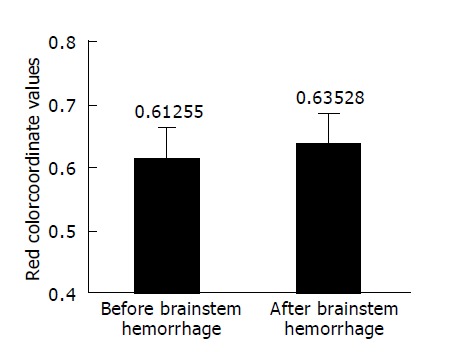
Paired t-test for red color coordinate mean values of jejunal mucous membrane before and after rabbit’s brainstem hemorrhage.
Figure 5.
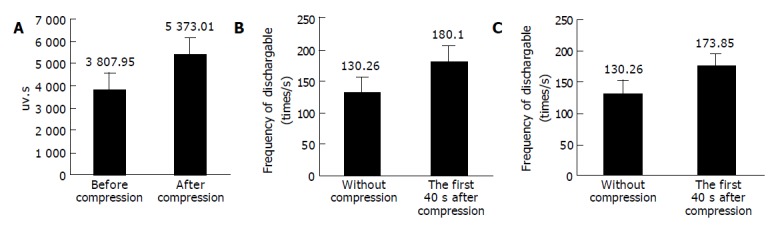
Comparison of electric discharge of vagus nerve. A: The comparison of the electric discharge of vagus nerve through analyzing the absolute value of an area of wave form before and after the compression (from 4 to 40 s under the intracranial hypertension), and the neural discharge of vagus nerve had increased after intracranial hypertension, n = 20, P<0.05; B: The comparison of the electric discharge of vagus nerve before and during the first 4 s after the rabbit’s lateral ventricle compression. We analyzed the electric discharge frequency of the dischargeable wave in each time segment by setting a single liminal value line, and the neural discharge of vagus nerve had increased after intracranial hypertension; C: The comparison of the electric discharge of vagus nerve before the compression and during continuous compression (from 4 to 40 s). We analyzed the electric discharge frequency of the dischargeable wave in each time segment by setting a single liminal value line, and the neural discharge of vagus nerve had increased after intracranial hypertension.
Figure 6.
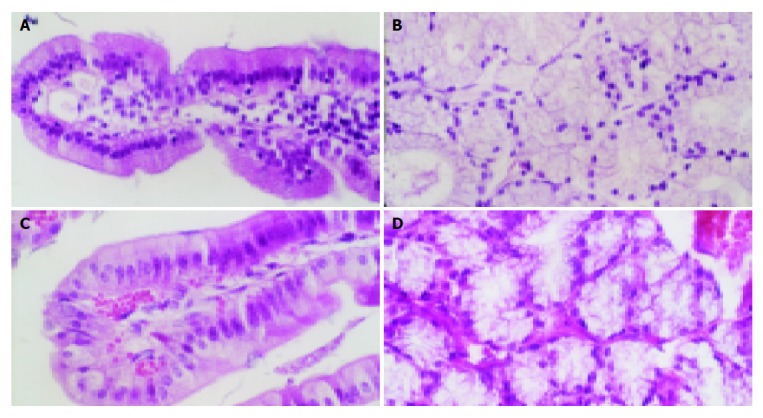
HE stain of duodenal structure of rabbits. A: HE stain of normal rabbit’s duodenal villus. The minute blood vessel had not dilated and red blood cells had not leaked out from capillary lumens; B: HE stain of normal rabbit’s mucous glands of duodenum. The minute blood vessel had not dilated; C: HE stain of the rabbit’s duodenal villus, which were 48 h after brainstem hemorrhage. The capillaries had obviously dilated and red blood cells had leaked out from capillary lumens; D: HE stain of the rabbit’s mucous glands of duodenum, which were 48 h after brainstem hemorrhage. The capillaries had obviously dilated and red blood cells had leaked out from capillary lumens.
DISCUSSION
Duodenal wall is usually divided into four layers structurally, which are mucous layer, submucous layer, muscular layer, and adventitia. Mucous layer and submucous layer protrude into the intestinal lumens to form the plica. Many duodenal glands can be seen in the connective tissue of the submucous layer. Muscular layer consists of two layers of smooth muscles, inner-ring and outer-vertical. Adventitia is the plasma membrane. At present, it is considered that the digestive tract ulcer is caused by the imbalance between the attacking factors (gastric juice) that has the function of digestion and the defense factors (mucus, mucosa, blood stream of mucosa) that prevent the stomach and duodenum from being digested[15,23-32]. In recent years, some experiments emphasize that the bloodstream of duodenal mucosa and the buffer capacity of mucosa endothelial cell are important factors that protect mucosa cell from being injured; experimental study of the stress ulcer shows that the nutrition of gastrointestinal tract (such as glucose) can prevent the stress ulcer[19]. The excessive breeding of the bacterium and infection can influence the bloodstream of mucosa, and weaken the gastric mucosal protective barrier function[29]. The balance can be broken by the stimulation from brain through the action of the autonomic nerve[22,33]. This type of ulcer is not only a digestive disease, but also the result that was comprehensively effected by multiple factors. The occurrence is related to the disturbance of body neuroendocrine, the weakness of gastric mucosal protective barrier function and the augment of gastric mucosa injury factors[27,33,34]. It was reported that the integrity of midbrain structure can influence the hemodynamics during the hemorrhage, according to the result of empirical studying in recent years. In this experiment we investigated the upper gastrointestinal stress ulcer bleeding, with the animal model of hemorrhage in inferior colliculus (midbrain), and found that it could influence the changes of bloodstream of the upper gastrointestinal mucosa[11]. After the primary and secondary lesion in brainstem, on one hand, the activities of sympathoadrenal system reinforced, the secretion of catecholamine in vivo had increased, the blood vessels in gastric mucosa contracted intensely, which caused the injury of the gastric mucosa; on the other hand, it stimulated the vagus nerve, which caused the increased excretion of gastric acid and pepsin, thus it aggravated the injury of gastric mucosal barrier. In the empirical study of observing and measuring the changes of bloodstream of gastroduodenal mucosa of shigellosis patients’ biopsies by fluorescence microscopy, some researchers found that there were microcirculatory changes of leukocyte movement and platelet aggregation in mucosal blood vessels, and the injury of gastric mucosa was related to the movement of leukocyte and platelet activation[30,31]. The proportion of midbrain hemorrhage in the brainstem hemorrhage has increased in recent years. In our experiment, we observed that the baseline of intracranial pressure wave increased in the acute brainstem hemorrhage. We thought that it was caused by the local high intracranial pressure, the occupation of hematoma in the brainstem at the level of inferior colliculus, and cerebrospinal fluid circulation disorder through hematoma compressing in aqueduct of midbrain. We also observed the reduction of the duodenal mucous membrane bloodstream, the dilatation of jejunal mesentery arterioles, and the transient increase in the congestion of jejunal mucous membrane in the early stage of acute brainstem hemorrhage model. The changes of bloodstream distribution were probably related to the changes of activities of sympathetic nerve and parasympathetic nerve[21]. It was indicated in a recent research that the decrease of gastroduodenal mucosal bloodstream, which is one of the important defense factors of mucosa, is related to the lack of NO synthetase and endothelium-derived relaxing factor in mucosal vascular endothelial cell[27]. The vagus nerve of rabbits initiates from the dorsal nucleus of vagus, its truncus goes into pectoral cavity and abdominal cavity through cervical part; it has branches which distribute to stomach and intestines. We calculated and measured the electric discharge activities of cervical vagus nerve continuously. It showed that the electric discharge of vagus nerve increased after intracranial hypertension. The average electric discharge intensity of vagus nerve increased rapidly during the first 4 s after the beginning of compression (P<0.002). Compared with the level before the compression of lateral ventricle, it also had significant increase during the 40 s followed (P<0.002). It implies that the factor of intracranial pressure should be considered in the mechanism of brainstem hemorrhage combined with the changes of digestive tract bloodstream. The intracranial hypertension could excite the vagus nerve to increase its electric discharge and influence the bloodstream of duodenum, jejunal mesentery and mucosa. Pathological slices, 48 h after acute brainstem hemorrhage, were analyzed and showed that there was a significant congestion of blood capillary in the duodenal villi and duodenal glands; some red blood cells leaked out into tissue space of submucous layer. These pathological changes are possibly the pathological basis of upper gastrointestinal hemorrhage caused by the stress ulcer in the condition of brainstem hemorrhage. It was reported that the weak stimulation of vagus nerve can cause the inhibition of intestinal movement; it was also reported that the vagotomy in the gastric mucosa can cause the reduction of gastric acid secretion. In this experiment, we found that the activity of vagus nerve has increased after the brainstem hemorrhage, and so we consider that the secretion of gastric acid should increase. We observed that the bloodstream of duodenal mucosa has decreased 20 s after the brainstem hemorrhage, and the minute blood vessel of duodenal mucosa, submucosa has obviously dilated and congested after the brainstem hemorrhage, for example, at 48 h after the brainstem hemorrhage. The stress ulcer with brainstem hemorrhage may relate to the activity of autonomic nerve and the blood stream of mucosa.
Footnotes
Supported by the Natural Science Foundation of Tianjin, No. 023610711; the Project Sponsored by SRF for ROCS, SEM; and the Teaching Research Foundation of Tianjin Medical University
Science Editor Zhu LH and Guo SY
Language Editor Elsevier HK
References
- 1.Suzaki F, Suzuki R, Sugiyama M. Relationship between location of stress erosive gastritis and brain damage in resuscitated patients. Nihon Shokakibyo Gakkai Zasshi. 2002;99:264–269. [PubMed] [Google Scholar]
- 2.Smirnov VM, Ivanchenko LM, Kromin AA. The mechanism of inhibition of small intestine contractions following irritation of rabbit's vagus nerve. Aviakosm Ekolog Med. 2001;35:53–57. [PubMed] [Google Scholar]
- 3.Lammie GA, Lindley R, Keir S, Wiggam MI. Stress-related primary intracerebral hemorrhage: autopsy clues to underlying mechanism. Stroke. 2000;31:1426–1428. doi: 10.1161/01.str.31.6.1426. [DOI] [PubMed] [Google Scholar]
- 4.Ceremuga TE, Yao XL, Alam HB, McCabe JT. Alterations of cullin-5 mRNA levels in the rat central nervous system following hemorrhagic shock. Neurol Res. 2003;25:211–216. doi: 10.1179/016164103101201229. [DOI] [PubMed] [Google Scholar]
- 5.Jones J. Stress responses, pressure ulcer development and adaptation. Br J Nurs. 2003;12:S17–S18, S20, S22 passim. doi: 10.12968/bjon.2003.12.Sup2.11321. [DOI] [PubMed] [Google Scholar]
- 6.Takeda H, Tsuji M, Hayashi M, Yamada T, Matsumiya T, Koizumi M, Kimura S. Pathophysiologic characteristics of the activity-stress paradigm in animal models: inhibitory effect of glucose on these responses. Nutr Rev. 2003;61:S75–S79. doi: 10.1301/nr.2003.may.S75-S79. [DOI] [PubMed] [Google Scholar]
- 7.Morales T, Sawchenko PE. Brainstem prolactin-releasing peptide neurons are sensitive to stress and lactation. Neuroscience. 2003;121:771–778. doi: 10.1016/s0306-4522(03)00522-0. [DOI] [PubMed] [Google Scholar]
- 8.Chen CH, Young YH. Vestibular evoked myogenic potentials in brainstem stroke. Laryngoscope. 2003;113:990–993. doi: 10.1097/00005537-200306000-00014. [DOI] [PubMed] [Google Scholar]
- 9.Arboix A, Comes E, García-Eroles L, Massons J, Oliveres M, Balcells M, Targa C. Site of bleeding and early outcome in primary intracerebral hemorrhage. Acta Neurol Scand. 2002;105:282–288. doi: 10.1034/j.1600-0404.2002.1o170.x. [DOI] [PubMed] [Google Scholar]
- 10.Inobe JJ, Mori T, Ueyama H, Kumamoto T, Tsuda T. Neurogenic pulmonary edema induced by primary medullary hemorrhage: a case report. J Neurol Sci. 2000;172:73–76. doi: 10.1016/s0022-510x(99)00295-6. [DOI] [PubMed] [Google Scholar]
- 11.Troy BP, Heslop DJ, Bandler R, Keay KA. Haemodynamic response to haemorrhage: distinct contributions of midbrain and forebrain structures. Auton Neurosci. 2003;108:1–11. doi: 10.1016/S1566-0702(03)00152-8. [DOI] [PubMed] [Google Scholar]
- 12.Chung SC. Current management of acute gastrointestinal bleeding. Scand J Gastroenterol Suppl. 2003;237:9–12. doi: 10.1080/00855910310001412. [DOI] [PubMed] [Google Scholar]
- 13.Goadsby PJ. Neurovascular headache and a midbrain vascular malformation: evidence for a role of the brainstem in chronic migraine. Cephalalgia. 2002;22:107–111. doi: 10.1046/j.1468-2982.2002.00323.x. [DOI] [PubMed] [Google Scholar]
- 14.Guven H, Amanvermez R, Malazgirt Z, Kaya E, Doganay Z, Celik C, Ozkan K. Moderate hypothermia prevents brain stem oxidative stress injury after hemorrhagic shock. J Trauma. 2002;53:66–72. doi: 10.1097/00005373-200207000-00014. [DOI] [PubMed] [Google Scholar]
- 15.Sung JJ. The role of acid suppression in the management and prevention of gastrointestinal hemorrhage associated with gastroduodenal ulcers. Gastroenterol Clin North Am. 2003;32:S11–S23. doi: 10.1016/s0889-8553(03)00058-x. [DOI] [PubMed] [Google Scholar]
- 16.Faisy C, Guerot E, Diehl JL, Iftimovici E, Fagon JY. Clinically significant gastrointestinal bleeding in critically ill patients with and without stress-ulcer prophylaxis. Intensive Care Med. 2003;29:1306–1313. doi: 10.1007/s00134-003-1863-3. [DOI] [PubMed] [Google Scholar]
- 17.Kawakubo K, Fujishima M. Management of gastrointestinal mucosal damage in patients with cerebrovascular disease. Nihon Rinsho. 2002;60:1573–1579. [PubMed] [Google Scholar]
- 18.Chen D, Yang X, Jiang X. Clinical and experimental study on effect of rhubarb on gastrointestinal blood flow perfusion. Zhongguo ZhongXiYi JieHe ZaZhi. 2000;20:515–518. [PubMed] [Google Scholar]
- 19.Ephgrave KS, Scott DL, Ong A, Cullen JJ, Broadhurst KA. Are gastric, jejunal, or both forms of enteral feeding gastroprotective during stress? J Surg Res. 2000;88:1–7. doi: 10.1006/jsre.1999.5727. [DOI] [PubMed] [Google Scholar]
- 20.Heslop DJ, Keay KA, Bandler R. Haemorrhage-evoked compensation and decompensation are mediated by distinct caudal midline medullary regions in the urethane-anaesthetised rat. Neuroscience. 2002;113:555–567. doi: 10.1016/s0306-4522(02)00161-6. [DOI] [PubMed] [Google Scholar]
- 21.Perkins E, Kimura H, Parent AD, Zhang JH. Evaluation of the microvasculature and cerebral ischemia after experimental subarachnoid hemorrhage in dogs. J Neurosurg. 2002;97:896–904. doi: 10.3171/jns.2002.97.4.0896. [DOI] [PubMed] [Google Scholar]
- 22.Landa García JI, Carabias Hernández A, Rodríguez Dapena S, Alcalde Escribano J, Ortega Medina L, Balibrea Cantero JL. Protective effect of vagotomy on the gastric mucosa in a stress model in rats. Rev Esp Enferm Dig. 2002;94:737–744. [PubMed] [Google Scholar]
- 23.Akbulut KG, Gönül B, Türkyilmaz A, Celebi N. The role of epidermal growth factor formulation on stress ulcer healing of the gastric mucosa. Surg Today. 2002;32:880–883. doi: 10.1007/s005950200171. [DOI] [PubMed] [Google Scholar]
- 24.Khadzhiev OC, Lupal'tsov VI, Simonenkov AP, Klimenko NA, Tatarko SV. Microcirculatory disturbances in gastric mucosa during ulcer disease and effects of serotonin on their dynamics. Bull Exp Biol Med. 2000;130:843–845. [PubMed] [Google Scholar]
- 25.Brzozowski T, Konturek PC, Konturek SJ, Drozdowicz D, Kwiecieñ S, Pajdo R, Bielanski W, Hahn EG. Role of gastric acid secretion in progression of acute gastric erosions induced by ischemia-reperfusion into gastric ulcers. Eur J Pharmacol. 2000;398:147–158. doi: 10.1016/s0014-2999(00)00287-9. [DOI] [PubMed] [Google Scholar]
- 26.Lee A. Animal models of gastroduodenal ulcer disease. Baillieres Best Pract Res Clin Gastroenterol. 2000;14:75–96. doi: 10.1053/bega.2000.0060. [DOI] [PubMed] [Google Scholar]
- 27.Abe Y, Itoh K, Arakawa Y. Altered vascular response to acetylcholine in conditions of endothelial damage in the isolated perfused rat stomach. J Gastroenterol. 2000;35:93–98. doi: 10.1007/s005350050020. [DOI] [PubMed] [Google Scholar]
- 28.Werther JL. The gastric mucosal barrier. Mt Sinai J Med. 2000;67:41–53. [PubMed] [Google Scholar]
- 29.Kaunitz JD, Akiba Y. Integrated duodenal protective response to acid. Life Sci. 2001;69:3073–3081. doi: 10.1016/s0024-3205(01)01413-8. [DOI] [PubMed] [Google Scholar]
- 30.Koshi R, Chandy G, Mathan M, Mathan VI. Vascular changes in duodenal mucosa in shigellosis and cholera. Clin Anat. 2003;16:317–327. doi: 10.1002/ca.10068. [DOI] [PubMed] [Google Scholar]
- 31.Kalia N, Bardhan KD, Reed MW, Jacob S, Brown NJ. Effects of chronic administration of Helicobacter pylori extracts on rat gastric mucosal microcirculation in vivo. Dig Dis Sci. 2000;45:1343–1351. doi: 10.1023/a:1005504019868. [DOI] [PubMed] [Google Scholar]
- 32.Bode JC, Bode C. Alcohol, the gastrointestinal tract and pancreas. Ther Umsch. 2000;57:212–219. doi: 10.1024/0040-5930.57.4.212. [DOI] [PubMed] [Google Scholar]
- 33.Lazebnik LB, Arbuzova VG, Sokolova GN, Astaf'eva OV, Petrakov AV, Nilova TV, Chikunova BZ. Role of stress in the etiopathogenesis of duodenal ulcer in young patients. Eksp Klin Gastroenterol. 2002;(5):30–33, 126-127. [PubMed] [Google Scholar]
- 34.Dyba S, Tychowska I, Klukowska L, Nadulska A. The influence of baclofen on reflex circulatory reactions evoked by stimulation of the vagus nerve in the rabbit. Ann Univ Mariae Curie Sklodowska Med. 2002;57:67–73. [PubMed] [Google Scholar]