

Abstract
To examine changes in dyadic communication, as well as links between communication and long-term relationship outcomes, 134 distressed couples randomly assigned to either Traditional Behavioral Couple Therapy (TBCT; Jacobson & Margolin, 1979) or Integrative Behavioral Couple Therapy (IBCT; Jacobson & Christensen, 1998) were observed in video-recorded interactions. Observers rated discussions of relationship problems at 3 time points (pre-therapy, post-therapy, 2-year follow-up) and relationship outcomes (i.e., treatment response and relationship stability) were measured at a 5-year follow-up. Consistent with previous examinations of individual partner communication (K.J.W. Baucom et al., 2011; Sevier et al., 2008), TBCT produced greater improvements from pre-therapy to post-therapy (d = .27 – .43) and superior communication at post-therapy (d = .30 – .37). However, IBCT produced greater improvements from post-therapy to 2-year follow-up (d = .32 – .39). Both levels of, and changes in, dyadic communication were associated with relationship outcomes, even when controlling for individual communication. Our findings lend additional support for theoretical and practical differences between these two therapies and the utility of assessment at the level of the couple. Furthermore, they contribute to a broader pattern of findings in which relationship outcomes are more consistently linked with constructive communication than with destructive communication.
Keywords: couple therapy, couple communication, observation methods, behavioral assessment, long-term treatment response
Interdependence theory defines a close relationship as one in which person A’s outcomes are related to person B’s outcomes (Thibaut & Kelley, 1978). Consistent with this theoretical framework, couple therapists and researchers alike consider patterns or sequences of interaction in which each member influences the other (e.g., demand/withdraw, negative reciprocity) to be a key relationship process and one of the most robust indicators of relationship functioning (Heyman, 2001). Despite the relevance of dyadic (i.e., couple-level) communication to both relationship theory and clinical practice, traditional observational rating systems used in treatment outcome research have been limited in their ability to adequately capture communication at the level of the couple. As a result, treatment outcome research has primarily focused on communication at the level of the individual (e.g., Halford, Sanders, & Behrens, 1993; Sevier, Eldridge, Jones, Doss, & Christensen, 2008). In the current study we examine changes in observed dyadic communication over the course of behavioral couple therapy and follow-up in a large sample of distressed couples. In addition to our examination of dyadic communication in isolation, we examine whether dyadic interaction patterns evidence unique links with long-term relationship outcomes when considered in concert with observed individual communication.
Observational coding systems used to assess communication during couples’ time-limited laboratory assessments typically provide detailed descriptions of specific individual behaviors to be coded such that inter-rater reliability is high and replication across sites meaningful (Kerig & Baucom, 2004). Examinations of changes in observed individual communication over the course of behavioral couple therapies typically demonstrate increases in positive communication and decreases in negative communication from pre-therapy to post-therapy (e.g., K.J.W. Baucom, Sevier, Eldridge, Doss, & Christensen, 2011; Halford et al., 1993; Sevier et al., 2008). Despite significant contributions of this work to the broader literature, there are several important limitations to these traditional observational approaches. First, the typical focus of these systems on individual partner communication largely neglects the defining characteristic of close relationships: interdependence (Thibaut & Kelley, 1978). Second, the methodological rigor of the large number of observational systems in existence may limit the ecological validity of work in the area of couple communication (e.g., Waldinger, Schulz, Hauser, Allen, & Crowell, 2004).
The vast majority of observational systems do not include a focus on dyadic communication. However, early microanalytic systems allowed for examination of dyadic interaction patterns via sequential analysis (e.g., Margolin & Wampold, 1981). Although treatment outcome work using this approach has demonstrated the importance of examining dyadic rather than individual communication in isolation (e.g., Hahlweg, Revenstorf, & Schindler, 1984), the utility of this approach is limited by low base rates of the initial (e.g., demand) and consequential (e.g., withdraw) behavior, as well as how soon after the initial behavior the consequential behavior must occur in the course of an interaction to assess the pattern (i.e., examination of lag-1 and lag-2 associations). As a result, sequences are usually low in frequency. Macroanalytic (global) ratings of dyadic interaction patterns address these limitations to microanalytic approaches, although only a small number of macroanalytic systems (e.g., Kline et al., 2004) include dyadic codes. In outcome research using these systems, dyadic and individual codes have been collapsed into composite positive and negative communication scales (e.g., Laurenceau, Stanley, Olmos-Gallo, Baucom & Markman, 2004).
Waldinger et al. (2004) argued that traditional observational systems force coders to adhere to researchers’ operationalizations of communication constructs, thus limiting their intuitive ability to make judgments. Recent empirical work in couple and family research demonstrates that untrained or naïve observers can rate complex interactional constructs with high interobserver agreement and high external validity (Baker, Haltigan, Brewster, Jaccard, & Messinger, 2010; K.J.W. Baucom, Baucom, & Christensen, 2012; Lorber, 2006; Waldinger et al., 2004). In the current study we examine dyadic communication rated by naïve1 observers using the Naïve Observational Rating System (NORS; Christensen, 2006). NORS ratings are associated with both trained ratings of individual communication and relationship outcomes (K.J.W. Baucom et al., 2012), but they have not yet been used to examine changes in communication over the course of behavioral couple therapies.
Behavioral Couple Therapies
In the current study we examine dyadic communication over the course of Traditional Behavioral Couple Therapy (TBCT; Jacobson & Margolin, 1979) and Integrative Behavioral Couple Therapy (IBCT; Jacobson & Christensen, 1998) and long term follow up. TBCT and IBCT have different ways of bringing about improvements in communication. TBCT provides rules and guidelines to teach couples specific, positive communication strategies (“rule-governed strategy”) while IBCT shapes new communication by exploring partners’ emotional reactions to each other’s communication (“contingency-shaped strategy”). As a result, TBCT may produce more rapid and obvious changes in communication: couples are explicitly trained in how to communicate and in the presence of the therapist or during a videotaped assessment might engage in those trained behaviors. In contrast, IBCT may produce slower but more enduring changes in communication: couples are not told exactly how to communicate, but as a result of more open communication that reveals the emotional impact of each partner’s behavior on the other, they may naturally shift their communication.
Based on social learning theory (Bandura, 1977), the traditional behavioral perspective is that distressed couples lack the necessary communication skills to solve their problems and as a result engage in excessive negative behavior and limited positive behavior when interacting about problems. As such, TBCT (Jacobson & Margolin, 1979) focuses on increasing positive behaviors and decreasing negative behaviors through the use of three main components: behavioral exchange, communication training, and problem solving training. In behavioral exchange, partners identify behaviors of the other that are positively reinforcing, and work to increase the instances of such behaviors. Behavioral exchange is typically used early in therapy to produce quick (though often short-lived) increases in relationship satisfaction that enable couples to engage in more difficult work on their relationship (Jacobson & Margolin, 1979). In communication training, partners are taught ways in which they can more effectively communicate with each other by use of both speaker skills (e.g., “I” statements rather than blaming “you” statements) and listener skills (e.g., paraphrasing). Finally, in problem solving training, couples learn to communicate differently about areas of disagreement, with the goal being that they come up with mutually agreed upon solutions to problems.
While behavioral researchers initially argued that a lack of positive behavior and a preponderance of negative behavior created distress in relationships, Jacobson and Christensen (1998) argued that distress is caused not just by a lack of skills but also by the individual differences between partners, their emotional sensitivities, the stressful environments in which they function, and the polarizing communication process that often occurs as they attempt to resolve the problems created by their differences, sensitivities and stressors. The therapy they developed, IBCT, was designed to target the couples that did not significantly improve from TBCT or that relapsed soon after treatment ended. In IBCT there is an added emphasis on emotional reactions to one’s partner, and in particular on emotional acceptance, in addition to TBCT’s focus on change in problem behavior. Three strategies for promoting emotional acceptance - empathic joining, unified detachment, and tolerance building - are the main focus of intervention in IBCT but TBCT techniques are also used. In empathic joining, therapists work to elicit the often hidden “soft emotions” that accompany conflict (e.g., hurt, disappointment) in addition to the often surface “hard emotions” (e.g., irritation, anger). The goal of empathic joining is to help partners experience intimacy around their problems, which can lead to both acceptance and behavior change. In unified detachment, the therapist helps partners to take a more objective, nonjudgmental view of their problems as distant from themselves and their relationship (i.e., to frame a problem as an “it” rather than a “you”). Finally, therapists use tolerance building to increase partners’ acceptance of one another, aiming to reduce the conflict that is associated with specific behaviors often by putting that behavior in context (e.g., “it is frustrating that your partner often gets home late from work, but that dedication is also something that you appreciate in her when it is applied to your family”). These interventions may not create immediate changes in communication in that partners are not told what to do differently but the eventual changes in communication and acceptance may come about more naturally and be more enduring.
Consistent with theoretical and practical differences between these two behavior therapies, research supports TBCT’s immediate impact and IBCT’s later impact on observed communication. Sevier et al. (2008) found TBCT produced greater improvements in individual communication from pre-therapy to post-therapy, as well as superior communication at post-therapy, in the current sample of distressed couples. However, K.J.W. Baucom et al. (2011) found the opposite pattern of results in changes in husband positivity and wife negativity from post-therapy to 2-year follow-up (i.e., IBCT produced greater improvements relative to TBCT). Although behavioral couple therapies include an explicit focus on dyadic communication, treatment outcome research to date has only examined individual communication. Building on these findings, in the current examination we expect TBCT to create greater change in dyadic communication from pre-therapy to post-therapy, and IBCT to create greater change in dyadic communication from post-therapy to 2-year follow-up.
Current Study
This study makes four important contributions to the existing literature. First, we focus on dyadic rather than individual communication. Research on communication as an outcome of behavioral couple therapies has focused on individual partners as the sole unit of analysis, despite theoretical and empirical support for interdependence between partners. In addition to our examination of dyadic communication, where possible we examine its unique associations with relationship outcomes (i.e., after controlling for the couple average of individual husband and wife communication). Second, we utilize naïve ratings of communication. Whereas standard observational systems capture subtle aspects of, and changes in, communication with much success, recent research suggests that untrained raters are able to use intuitive knowledge about relationships to reliably rate couple and family interactions in a way that provides similar (e.g., Lorber, 2006; Waldinger et al., 2004) – and at times even superior (K.J.W. Baucom et al., 2012) – information to that gleaned from highly trained coding systems. To our knowledge, no previous research has used naïve ratings to evaluate therapy outcome. Third, we test for differences in the trajectories of change in dyadic communication over the course of therapy (i.e., pre-therapy to post-therapy) and follow-up (i.e., post-therapy to 2-year follow-up) between two behavioral couple therapies. Previous research has rarely if ever examined observational data two years after treatment termination. Finally, we examine the extent to which levels of, and changes in, dyadic communication are associated with long-term relationship outcomes.
We predicted that couples’ dyadic communication would improve over time, but that improvements would depend on treatment type (Hyp. 1). Specifically, TBCT couples would display greater improvements in communication from pre-therapy to post-therapy and superior communication at post-therapy relative to IBCT couples. However, from post-therapy to 2-year follow-up, IBCT couples would evidence greater improvements in communication relative to TBCT couples. We expected that greater improvements in, and higher levels of, communication would be associated with greater likelihood of positive response to treatment and relationship stability at 5-year follow-up (Hyp. 2).
Method
Participants
Participants were 134 seriously and chronically distressed married heterosexual couples from a randomized clinical trial; all scored in the distressed range of relationship functioning at three different assessment points prior to beginning treatment. The sample was 77.6% Caucasian, 7.5% African American, 5.2% Asian American/Pacific Islander, 5.2% Latino, 0.6% Native American/Alaskan Native, and 4.1% other. The average ages of participants were 43.5 years (SD = 8.8) for husbands and 41.6 years (SD = 8.6) for wives. Couples were predominantly middle-class, college educated, and married an average of 10.0 years (SD = 7.6). Fifty-six percent of individuals in the study met criteria for a lifetime Axis I or Axis II psychiatric diagnosis, and 15.6% had a current diagnosis. A number of couples were excluded from the study due to wife-reported moderate to severe intimate partner violence from husbands (N = 101), not meeting the threshold for chronic distress (N = 94), or exclusionary psychiatric diagnoses (N = 3). See Christensen, Atkins, Berns, Wheeler, Baucom, et al. (2004) for additional details of the sample.
Procedure
Based on the average husband and wife pre-therapy relationship satisfaction reported on the Dyadic Adjustment Scale (DAS; Spanier, 1976) as well as the Global Distress Scale of the Marital Satisfaction Inventory-Revised (Snyder, 1997), couples were classified as either moderately or severely distressed (see Christensen et al., 2004 for additional details about stratification). Within distress stratification levels, couples were randomly assigned to either TBCT (68 couples) or IBCT (66 couples). Couples received an average of 22.9 (SD = 5.35) sessions of either TBCT or IBCT. At each of three time points (pre-therapy, post- therapy, and 2-year follow-up), couples completed two 10-minute video-recorded relationship problem discussions. The post-therapy assessment occurred 26 weeks after the pre-therapy assessment for all couples; some couples were still in the final sessions of active treatment at this time. The 2-year follow-up assessment occurred 2.5 years after the pre-therapy assessment for all couples. At each time point each spouse picked a topic for one of the two discussions, and the order of the discussions (i.e., husband’s topic first vs. wife’s topic first) was counterbalanced. Discussions included 133 couples at pre-therapy, 118 couples at post-therapy2, and 84 couples at 2-year follow up. See K.J.W. Baucom et al. (2011) for a flow chart of observational assessments.
Measures
Dyadic communication
The Naïve Observational Rating System (NORS; Christensen, 2006) is a 15-item global observational rating system developed to capture dyadic communication during interactions. Relationship quality and five of the six dyadic NORS codes were included in this paper. Relationship quality was rated on a 100-point scale (higher scores representing greater quality of the relationship), and five dyadic interaction patterns were rated on a Likert scale from 1 (low) to 10 (high). Inter-rater reliability coefficients for NORS codes were calculated separately within each of the two discussions (husband’s topic, wife’s topic) at each time point and averaged across the six interactions: relationship quality (.81), negative reciprocity (.82), positive reciprocity (.78), wife demand/husband withdraw (WD/HW; .68), husband demand/wife withdraw (HD/WW; .62), and vulnerability/empathy (.68). Mutual avoidance was the only dyadic interaction pattern in the NORS that was not included in the current paper (due to insufficient inter-rater reliability). Table 1 presents descriptive statistics for codes by time and therapy type.
Table 1.
Descriptive Statistics of Dyadic Communication by Time and Therapy
| Pre-Therapya
|
Post-Therapyb
|
2-yr Follow-Upc
|
||||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| Quality | ||||||
| TBCT | 46.01 | 12.69 | 49.76 | 13.57 | 48.65 | 14.01 |
| IBCT | 45.97 | 11.42 | 46.78 | 11.86 | 50.25 | 13.34 |
| Negative Reciprocity | ||||||
| TBCT | 4.76 | 1.96 | 3.82 | 1.72 | 3.99 | 1.76 |
| IBCT | 4.40 | 1.60 | 4.28 | 1.72 | 3.81 | 1.55 |
| Positive Reciprocity | ||||||
| TBCT | 3.20 | 1.47 | 3.97 | 1.70 | 3.78 | 1.79 |
| IBCT | 3.38 | 1.63 | 3.46 | 1.60 | 4.01 | 1.84 |
| WD/HW | ||||||
| TBCT | 4.13 | 1.68 | 3.65 | 1.52 | 3.69 | 1.51 |
| IBCT | 3.92 | 1.47 | 3.89 | 1.62 | 3.64 | 1.39 |
| HD/WW | ||||||
| TBCT | 3.35 | 1.25 | 3.00 | 1.28 | 3.05 | 1.26 |
| IBCT | 3.28 | 1.17 | 3.20 | 1.28 | 3.02 | 1.24 |
| Vulnerability/empathy | ||||||
| TBCT | 3.66 | 1.36 | 4.44 | 1.70 | 4.28 | 1.57 |
| IBCT | 3.80 | 1.32 | 3.94 | 1.46 | 4.30 | 1.46 |
Note. Descriptive statistics presented in this table are untransformed.
N = 133 (65 IBCT, 68 TBCT).
N = 118 (61 IBCT, 57 TBCT).
N = 84 (41 IBCT, 43 TBCT).
We selected undergraduate student raters who seemed reasonably socially skilled but who had no previous coursework or research experience that specifically related to romantic relationships. They were uninformed as to the purpose of the larger research study, our hypotheses, and the spacing between and details of the three time points. Furthermore, the order of observational segments from the three time points was randomized. Each rater observed each of the three segments for a given couples’ interaction type and rated them in one sitting (e.g., in one sitting a rater observed couple 451’s three husband’s topic relationship problem interactions in the order of post therapy first, 2-year follow-up second, and pre-therapy third). We believed this arrangement would enable observers to make finer grained distinctions between the three interactions. Raters were given minimal descriptions of communication. For example, negative reciprocity instructions stated “To what extent did the couple exchange negative comments and negative nonverbal behavior in a ‘tit-for-tat’ like way (e.g., criticize each other or exchange sarcastic comments, put-downs, frowns, sneers, or looking away in anger or disgust)?” and included the note “You are to rate the extent to which partners exchange negative comments. If one partner is negative but the other never reciprocates that with negative behavior (instead is only neutral or positive), you would rate negative reciprocity as 1.” See K.J.W. Baucom et al. (2012) for additional details on the rating procedures.
Individual communication
Individual communication was assessed during the 10-min interactions using the 13-item Couple Interaction Rating System (CIRS; Heavey, Gill, & Christensen, 1998) and the 18-item Social Support Interaction Rating System (SSIRS; Jones & Christensen, 1998). These global observational rating systems were designed to assess problem-solving and communication behavior (Heavey et al., 1998) as well as emotional features of interactions (Jones & Christensen, 1998) on a Likert scale from 1 (none) to 9 (a lot). There were separate teams of coders for each of the two systems (SSIRS, CIRS), but coders in both systems were instructed to rate one partner at a time and consider the frequency, context, and intensity of behavior in making their global ratings. Coders were blind to study hypotheses and rated pre-therapy, post-therapy, and 2-year follow-up interactions in a random order for all couples (i.e., they did not rate a given couple’s interactions in one sitting as the naïve observers did). Although we examine only relationship problem interactions for those couples who underwent behavioral couple therapy in the current manuscript, coders assessed both relationship and personal problem interactions for the distressed couples in the current manuscript as well as for nondistressed control couples. Principal components analysis of items from both the CIRS and SSIRS revealed four individual communication scales: negativity, positivity, withdrawal, and problem solving (Sevier et al., 2008). We examine only negativity and positivity in the current manuscript. Both demonstrated good interobserver reliabilities (Cronbach’s alpha ranges were .86–.95 for negativity and .81–.95 for positivity) as well as good internal consistency among scale items (.88 for negativity and .71 for positivity). See Sevier et al. (2008) for a more detailed description of individual communication rating procedures.
Treatment response
We classified couples as either responders or nonresponders to treatment based on clinically significant change in DAS (Spanier, 1976) scores from pre-therapy to 5-year follow-up using Jacobson and Truax’s (1991) formula. Nonresponders to treatment included couples that reliably declined in relationship satisfaction, divorced or separated, or did not reliably change in either direction. Responders to treatment included couples that demonstrated reliable increases in relationship satisfaction. Of participants who were in the study through 5-year follow up, 62 couples were nonresponders (46%), 57 couples were responders (43%), and we did not have data on 15 couples (11%). There were no significant treatment differences in treatment response (Christensen, Atkins, Baucom, & Yi, 2010).
Relationship stability
Five years after treatment, marital status was obtained on all 134 couples: 98 (73.1%) couples were still married and 36 (26.9%) couples were divorced or legally separated. There were no significant treatment differences in stability (Christensen et al., 2010).
Results
Descriptive statistics revealed substantial skew in five of the six communication variables. Only relationship quality was normally distributed; we used natural log transformations of the other five variables in all analyses. We tested hypotheses using Hierarchical Linear and Nonlinear Modeling (HLM 7; Raudenbush, Bryk, Cheong, Congdon, & de Toit, 2011) with post hoc hypothesis tests of simple effects. Given space constraints, we limit discussion of results to the effects that directly test hypotheses.
Changes in Dyadic Communication over Time (Hypothesis 1)
Hypothesis 1 analyses
To test whether communication changed over time we ran separate models predicting each communication variable and modeled separate slopes for changes from pre-therapy to post-therapy and changes from post-therapy to 2-year follow-up. We modeled slopes separately since the spacing between time points was different and there was a qualitative difference between these two periods of time (i.e., in the first period couples went through therapy). Time variables were coded such that the overall intercept represented the predicted level of the outcome variable post-therapy (pre-therapy to post-therapy slope was coded pre-therapy = −1, post-therapy = 0; post-therapy to 2-year follow-up slope was coded post-therapy = 0, 2-year = 1). We included random effects on the intercepts and time slopes of all models.
In order to test our first hypothesis we included therapy type (TBCT = −.5, IBCT = .5) at Level 2. We controlled for which partner chose the topic (husband’s topic = −.5, wife’s topic = .5) at Level 1, as well as pre-therapy distress stratification (severely distressed = −.5, moderately distressed = .5) and its interaction with therapy type at Level 2. The following is the within-couple equation (Level 1):
Hypothesis 1 results
Post hoc hypothesis tests revealed no significant differences in communication between TBCT and IBCT couples at pre-therapy (ps > .10).3
Pre-therapy to post-therapy changes in communication
Table 2 presents results of these models, and Figure 1 displays trajectories of change in communication by therapy type. Consistent with hypotheses and published results examining individual communication (K.J.W. Baucom et al., 2011; Sevier et al., 2008), TBCT couples evidenced greater improvements in communication from pre-therapy to post-therapy than did IBCT couples on four of the six variables. TBCT couples’ negative reciprocity and WD/HW significantly decreased (χ2 = 21.06, p < .001 and χ2 = 13.14, p < .001, respectively) and positive reciprocity and vulnerability/empathy significantly increased (χ2 = 11.95, p < .001 and χ2 = 14.93, p < .001, respectively). There were no significant changes from pre-therapy to post-therapy in negative reciprocity (χ2 = 0.90, n.s.), WD/HW (χ2 = 0.60, n.s.), positive reciprocity (χ2 = 0.24, n.s.), or vulnerability/empathy (χ2 = 0.15, n.s.) for IBCT couples. In addition to these changes that varied across treatments, both IBCT couples and TBCT couples demonstrated significant increases in rated relationship quality and significant decreases in HD/WW from pre-therapy to post-therapy (ps < .01) but these changes did not depend on therapy type.
Table 2.
Post-therapy Levels of, and Changes in, Dyadic Communication over Time
| Pre-Post Change
|
Post-Therapy Levels
|
Post-Follow-up Change
|
|||||||
|---|---|---|---|---|---|---|---|---|---|
| B | SE | d | B | SE | d | B | SE | d | |
| Quality Intercept | 2.09** | 0.79 | 48.32*** | 0.97 | 0.28 | 0.82 | |||
| Therapy | −2.81† | 1.57 | −.22 | −3.78† | 1.93 | −.30 | 4.06* | 1.64 | .32 |
| Stratification | −0.90 | 1.57 | −.07 | 8.05*** | 1.93 | .63 | −5.39*** | 1.64 | −.42 |
| Therapy*Stratification | 0.28 | 3.15 | −2.57 | 3.86 | −1.39 | 3.28 | |||
|
| |||||||||
| Negative Reciprocity Intercept | −0.14*** | 0.03 | 1.30*** | 0.03 | −0.02 | 0.04 | |||
| Therapy | 0.19** | 0.07 | .43 | 0.16* | 0.07 | .35 | −0.17* | 0.07 | −.39 |
| Stratification | 0.01 | 0.07 | .02 | −0.23*** | 0.07 | −.53 | 0.23** | 0.07 | .53 |
| Therapy*Stratification | 0.17 | 0.13 | 0.21 | 0.13 | −0.04 | 0.15 | |||
|
| |||||||||
| Positive Reciprocity Intercept | 0.12** | 0.04 | 1.20*** | 0.04 | 0.01 | 0.04 | |||
| Therapy | −0.19* | 0.08 | −.38 | −0.17* | 0.07 | −.34 | 0.20* | 0.08 | .39 |
| Stratification | −0.02 | 0.08 | −.04 | 0.27*** | 0.07 | .55 | −0.24** | 0.08 | −.48 |
| Therapy*Stratification | 0.01 | 0.15 | 0.00 | 0.14 | −0.13 | 0.15 | |||
|
| |||||||||
| WD/HW Intercept | −0.09** | 0.03 | 1.22*** | 0.03 | 0.01 | 0.04 | |||
| Therapy | 0.12* | 0.05 | .27 | 0.08 | 0.06 | .20 | −0.08 | 0.07 | −.19 |
| Stratification | −0.03 | 0.05 | −.06 | −0.14* | 0.06 | −.32 | 0.21** | 0.07 | .48 |
| Therapy*Stratification | 0.21† | 0.11 | 0.38** | 0.12 | −0.40** | 0.14 | |||
|
| |||||||||
| HD/WW Intercept | −0.07** | 0.02 | 1.06*** | 0.03 | −0.05† | 0.03 | |||
| Therapy | 0.07 | 0.04 | .18 | 0.06 | 0.06 | .16 | −0.08 | 0.06 | −.21 |
| Stratification | 0.00 | 0.04 | −.01 | −0.05 | 0.06 | −.12 | 0.06 | 0.06 | .15 |
| Therapy*Stratification | 0.04 | 0.09 | −0.17 | 0.12 | 0.29** | 0.11 | |||
|
| |||||||||
| Vulnerability/Empathy Intercept | 0.10** | 0.03 | 1.35*** | 0.03 | 0.02 | 0.03 | |||
| Therapy | −0.17** | 0.06 | −.42 | −0.14* | 0.06 | −.37 | 0.13* | 0.07 | .33 |
| Stratification | 0.03 | 0.06 | .07 | 0.27*** | 0.06 | .69 | −0.23*** | 0.07 | −.59 |
| Therapy*Stratification | −0.03 | 0.13 | −0.05 | 0.13 | −0.14 | 0.13 | |||
Note. d = Cohen’s d. See text for results of tests of simple effects.
p < .10,
p < .05,
p < .01,
p < .001
Figure 1.
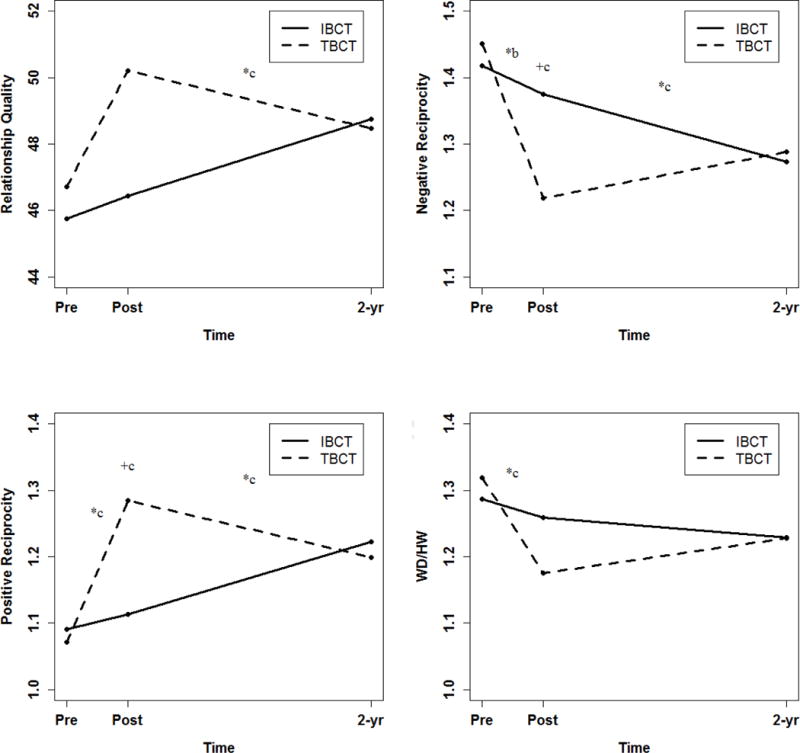
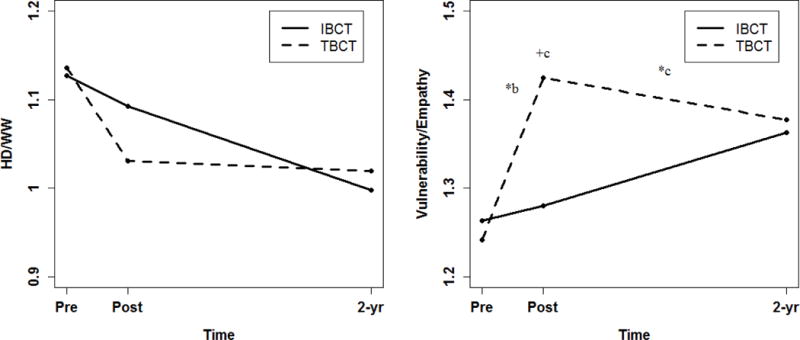
Predicted regression scores of dyadic communication by treatment type. *significant difference between treatments in communication change, +significant difference between treatments in communication level
ap < .001, bp < .01, cp < .05
Mean levels of communication at post-therapy
We also found some support for hypothesized treatment differences in levels of communication at post-therapy. TBCT couples used less negative reciprocity (p < .05), and more positive reciprocity and vulnerability/empathy (ps < .01) than IBCT couples. Therapy differences in levels of WD/HW at post-therapy depended on stratification. Moderately distressed IBCT couples displayed significantly more WD/HW than did moderately distressed TBCT couples (χ2 = 11.33, p < .01), but there were not significant treatment differences in severely distressed couples (χ2 = 1.42, n.s.). Within TBCT couples, severely distressed couples used significantly more WD/HW at post-therapy than did moderately distressed couples (χ2 = 18.08, p < .001) but there were no significant differences between levels of distress in IBCT (χ2 = 0.34, n.s.). There were no significant treatment differences in rated relationship quality or HD/WW at post-therapy.
Post-therapy to 2-year follow-up changes in communication
Also consistent with our hypothesis and previous findings, we found the reverse pattern of treatment effects from post-therapy to 2-year follow-up as we did from pre-therapy to post-therapy. Whereas IBCT couples’ relationship quality significantly increased over this time period (χ2 = 4.08, p < .05), TBCT couples’ relationship quality did not significantly change (χ2 = 2.22, p = .13). Similarly, IBCT couples’ negative reciprocity marginally decreased (χ2 = 3.71, p = .05), and positive reciprocity and vulnerability/empathy marginally increased (χ2 = 3.53, p = .06 and χ2 = 2.71, p < .1, respectively); however TBCT couples’ negative reciprocity and vulnerability/empathy did not significantly change (χ2 = 1.93, p = .16 and χ2 = 1.30, n.s., respectively), and positive reciprocity marginally decreased (χ2 = 2.98, p = .08). Changes in both WD/HW and HD/WW from post-therapy to 2-year follow-up depended on treatment type and stratification (described below).
Changes in WD/HW from post-therapy to 2-year follow-up were only significant in TBCT couples. WD/HW significantly decreased in severely distressed TBCT couples (χ2 = 8.09, p < .01), and significantly increased in moderately distressed TBCT couples over this time period (χ2 = 8.39, p < .01). There were no significant changes in WD/HW in IBCT couples from post-therapy to 2-year follow-up (χ2 = 0.17, n.s. in severely, and χ2 = 0.19, n.s. in moderately distressed couples). HD/WW decreased in severely distressed IBCT couples (χ2 = 10.302, p < .01) but did not significantly change in moderately distressed IBCT couples (χ2 = 1.21, n.s.) or in TBCT couples (χ2 = 0.45, n.s. in severely, and χ2 = 1.21, n.s. in moderately distressed couples).
Despite differences between IBCT and TBCT couples in the timing of changes in communication, there were no significant differences between treatments in levels of communication at 2-year follow-up (ps > .10).
Hypothesis 1 post hoc tests
One alternative explanation to our Hypothesis 1 results is that communication at 2-year follow-up represents regression to the mean, where communication that initially increased would tend to decrease, and vice versa. To rule out this explanation we ran a series of post-hoc hypothesis tests to determine whether communication was significantly different at 2-year follow-up relative to pre-therapy. All communication significantly changed from pre-therapy to 2-year follow-up in expected directions.4 These findings, in combination with meta-analytic findings that communication of treatment-seeking distressed couples on waitlists naturally improves over time (D.H. Baucom, Hahlweg, & Kuschel, 2003), provide support against the explanation that changes in the present study are due to regression to the mean.
Associations between Dyadic Communication and Relationship Outcomes (Hypothesis 2)
Hypothesis 2 analyses
To test whether levels of communication, and changes therein, were associated with relationship outcomes at 5-year follow-up, relationship variables were added at Level 2, with separate sets of models for each of the two relationship outcomes at 5-year follow-up (i.e., treatment response and relationship stability). Covariates were identical to those in Hypothesis 1 models with two exceptions: 1) we only included a Level-2 interaction term between therapy type and distress stratification when it was found to be significant in Hypothesis 1 (i.e., in WD/HW and HD/WW models), and 2) we included group (couple) mean centered ratings of average individual partners negativity and positivity (i.e., average of ratings of husband and wife at each time point) in models examining associations between relationship outcomes and negative reciprocity and positive reciprocity, respectively.5
Hypothesis 2 results
Table 3 presents associations between relationship outcomes and communication. Consistent with predictions, couples who demonstrated greater pre-therapy to post-therapy increases in rated relationship quality (p < .001), positive reciprocity after controlling for couple average individual positivity (p < .01), and vulnerability/empathy (p < .05) had significantly better treatment outcomes at 5-year follow-up. Whereas these types of communication did not significantly change from pre-therapy to post-therapy in nonresponders (χ2 = 0.59, n.s., χ2 = 0.05, n.s., and χ2 = 0.05, n.s., respectively), they significantly increased in responders (χ2 = 15.90, p < .001, χ2 = 10.49, p < .01, and χ2 = 11.89, p < .001, respectively). Couples who demonstrated higher post-therapy levels of rated relationship quality (p < .001), positive reciprocity after controlling for couple average individual positivity (p < .01), and vulnerability/empathy (p < .01) were also more likely to be classified as treatment responders at 5-year follow-up. Only changes in vulnerability/empathy from post-therapy to 2-year follow-up were associated with treatment response. Contrary to our predictions, increases in vulnerability/empathy were associated with worse treatment outcomes at 5-year follow-up. Whereas this communication did not significantly change from post-therapy to 2-year follow-up in responders (χ2 = 0.34, n.s.), it significantly increased in nonresponders (χ2 = 4.60, p < .05).
Table 3.
Associations between Dyadic Communication and Relationship Outcomes Five Years Post-Therapy
| Rating | Pre-therapy to Post-therapy Change
|
Post-therapy Levels
|
Post-therapy to 2-year Follow-up Change
|
|||
|---|---|---|---|---|---|---|
| B(SE) | d | B(SE) | d | B(SE) | d | |
| Associations between treatment response and communication | ||||||
| Quality | 5.94 (1.82)*** | .45 | 7.03 (2.11)*** | .54 | −2.09 (2.07) | −.16 |
| Negative Reciprocitya | −0.06 (0.05) | −.19 | −0.09 (0.06) | −.27 | −0.06 (0.07) | −.12 |
| Positive Reciprocitya | 0.17 (0.06)** | .41 | 0.20 (0.07)** | .50 | −0.03 (0.08) | −.05 |
| WD/HW | −0.05 (0.06) | −.11 | −0.03 (0.07) | −.08 | 0.05 (0.08) | .11 |
| HD/WW | 0.04 (0.05) | .09 | 0.04 (0.06) | .10 | −0.01 (0.07) | −.03 |
| Vulnerability/Empathy | 0.15 (0.07)* | .38 | 0.20 (0.06)** | .50 | −0.14 (0.07)* | −.36 |
|
| ||||||
| Associations between relationship stability and communication | ||||||
| Quality | 4.17 (2.06)* | .33 | 8.19 (2.37)*** | .64 | −1.40 (261) | −.11 |
| Negative Reciprocitya | −0.05 (0.06) | −.10 | −0.19 (0.07)** | −.44 | −0.16 (0.07)* | −.36 |
| Positive Reciprocitya | 0.08 (0.06) | .17 | 0.24 (0.08)** | .48 | −0.04 (0.12) | −.08 |
| WD/HW | −0.04 (0.06) | −.09 | −0.06 (0.08) | −.14 | 0.20 (0.08)* | .47 |
| HD/WW | 0.03 (0.05) | .08 | 0.01 (0.08) | .01 | 0.04 (0.10) | .09 |
| Vulnerability/Empathy | 0.14 (0.07) † | .35 | 0.25 (0.07)*** | .63 | −0.11 (0.11) | −.28 |
Note. Unstandardized regression coefficients for effects of treatment response and relationship stability represent the magnitude of the difference between the two levels (since for treatment response, nonresponder = −.5, responder = .5, and stability, divorced = −.5, intact = .5) controlling for therapy type and distress level. See text for results of tests of simple effects.
Negative reciprocity models included couple-average of individual negativity, and positive reciprocity models included couple-average individual positivity, as covariates. Thus, these results are unique associations between relationship outcomes and dyadic communication after controlling for individual communication.
d = Cohen’s d.
p < .10,
p < .05,
p <. 01,
p <. 001
In addition to links between communication and treatment outcome, we found a similar pattern of associations between communication and relationship stability at 5-year follow-up. Consistent with our hypothesis, couples who demonstrated greater increases in rated relationship quality from pre-therapy to post-therapy were more likely to remain married at 5-year follow-up (p < .05). Whereas quality did not significantly change from pre-therapy to post-therapy in couples who subsequently divorced (χ2 = 0.42, n.s.), it significantly increased in those who remained together (χ2 = 11.70, p < .001). Couples who demonstrated higher post-therapy levels of rated relationship quality, positive reciprocity after controlling for couple-average positivity, and vulnerability/empathy (ps < .01), as well as lower post-therapy levels of negative reciprocity after controlling for couple-average negativity (p < .01), were more likely to remain married at 5-year follow-up. Changes in negative reciprocity and WD/HW from post-therapy to 2-year follow-up were associated with relationship stability. Although both couples who subsequently divorced and those who remained together evidenced significant increases in negative reciprocity from post-therapy to 2-year follow-up (χ2 = 15.58, p < .001, and χ2 = 15.13, p < .001, respectively), those who ultimately divorced increased more over this time period (B = 0.27) than those who remained together (B = 0.11). Contrary to our predictions, WD/HW significantly decreased from post-therapy to 2-year follow-up in couples who subsequently divorced (χ2 = 5.45, p < .05), but did not significantly change in those who remained together (χ2 = 0.79, n.s.).
Hypothesis 2 post hoc tests
In light of a pair of counterintuitive findings in Hypothesis 2 linking greater improvements in communication from post-therapy to 2-year follow-up (i.e., increases in vulnerability/empathy and decreases in WD/HW) to worse 5-year relationship outcomes, we ran a series of additional post hoc hypothesis tests in HLM to determine whether nonresponders and couples who later divorced were actually demonstrating superior communication relative to their counterparts. We tested for differences between couples who had good long-term outcomes (i.e., couples classified as intact and treatment responders at 5-year follow-up) and those who had poor long-term outcomes (i.e., couples who separated/divorced or were classified as treatment nonresponders at 5-year follow-up) in: (1) levels of communication at 2-year follow-up, and (2) changes in communication over the entire course of observational assessments (i.e., from pre-therapy to 2-year follow-up). There were not significant differences between responders and nonresponders in levels of vulnerability/empathy at 2-year follow-up (χ2 = .52, n.s.) or in changes from pre-therapy to 2-year follow-up (B = −0.02, SE = 0.08, n.s.). Similarly, there were not significant differences between divorced couples and those that remained married in levels of WD/HW at 2-year follow-up (χ2 = 2.89, p = 0.09) or in changes from pre-therapy to 2-year follow-up (B = 0.18, SE = 0.09, p = .061). Thus, while several of our findings related to changes in communication are counterintuitive, when considered in the context of overall levels of communication and changes over the entire course of the study they are less surprising.
Discussion
We examined trajectories of change in dyadic communication of couples from a large randomized clinical trial of behavioral couple therapies. Undergraduate research assistants unfamiliar with relationship research assessed aspects of communication at each of three time points (pre-therapy, post-therapy, and 2-year follow-up). This study focused on differences between therapies in trajectories of change in communication, as well as the extent to which communication was associated with long-term relationship outcomes. We discuss our findings in the context of theoretical and practical differences between therapies, as well as previous empirical work in this sample and couple research more broadly.
Differences in Trajectories of Dyadic Communication in IBCT and TBCT
The first aim of the study was to examine whether communication changed over the course of therapy and follow-up, and if these changes depended on treatment type. We found strong support for hypothesized changes and moderate support for treatment differences in these changes. As hypothesized, TBCT couples showed immediate improvements in communication that were superior to those produced by IBCT. However, IBCT couples displayed improvements after treatment termination while TBCT couples did not evidence further gains. These effects are consistent with previous examinations of changes in individual communication over this time period in both direction and effect size (K.J.W. Baucom et al., 2011; Sevier et al., 2008), but differences between treatments were more consistent across codes in the current examination.
We interpret these findings to represent differential effects of the respective change strategies in TBCT and IBCT. In TBCT partners are instructed to do positive things for one another (behavior exchange), interact with one another in a specific manner that is thought to be most effective (communication training), and use a series of steps to solve problems that arise (problem solving training). We generally found improvements in communication in TBCT couples over the short-term (i.e., from pre-therapy to post-therapy), consistent with previous observational studies of individual partner behavior (e.g., D.H. Baucom, Sayers, & Sher, 1990; Sevier et al., 2008). However, our findings suggest a similar effect on dyadic communication to that on individual communication (K.J.W. Baucom et al., 2011) following TBCT in that gains ended along with treatment. This pattern of findings may also result from demand characteristics, in that TBCT couples at post-therapy may feel pressure to show what they have learned but may not experience such pressure two years later. In the outcome study that provided the data for the current investigation, couples in TBCT showed rapid improvement in relationship satisfaction followed by a leveling off of improvement during treatment while IBCT couples showed consistent, gradual improvement in relationship satisfaction during treatment (Christensen et al., 2004). Although there was no significant difference between treatments in relationship satisfaction at termination, couples in IBCT maintained gains in satisfaction significantly more than their TBCT counterparts during the first two years of follow-up (Christensen et al., 2010).
While IBCT utilizes change-focused strategies to some extent, it is distinct from TBCT in its focus on acceptance through three strategies: empathic joining, unified detachment, and tolerance building. Voicing soft rather than hard emotions (in empathic joining) is likely difficult for a partner in the short-term since it puts them in a vulnerable position, but is likely more easily received by the other partner relative to hard emotions such as judgment or criticism. This intervention, in combination with a nonjudgmental view of a couple’s problematic interaction pattern as an “it” (unified detachment) and contextual consideration of the behavior of one’s partner that really irks him or her (tolerance building), targets problematic relationship functioning through a focus on specific examples of dyadic interaction patterns that exemplify broader themes in the relationship. Through these strategies, communication is not altered directly by instructions about how to communicate but indirectly by eliciting emotional reactions from each, by encouraging dyadic analysis by both, and by facilitating contextual understanding of each partner’s behavior. Despite this less explicit focus on changing specific behaviors, IBCT produced additional improvements in communication following treatment termination, suggesting that while these strategies produce limited immediate change (or change due to demand characteristics), it is possible that they ultimately create more lasting change in communication. We believe that TBCT therapists’ instruction of partners in how to interact with one another more effectively (rule-governed change), and IBCT therapists’ facilitation of naturally occurring changes in communication through a focus on the functional impact of one partner’s behavior on the other (contingency-shaped change) likely account for this difference.
Associations between Dyadic Communication and Relationship Outcomes
We found moderate support for our second hypothesis, such that greater improvements in communication from pre-therapy to post-therapy, as well as superior levels of communication at post-therapy, were linked with better relationship outcomes (i.e., treatment response and relationship stability at 5-year follow-up). Negative reciprocity, and to a greater extent positive reciprocity, demonstrated links with relationship outcomes even after controlling for couple-average individual communication, highlighting the need for examination of communication at the level of the couple. Consistent with interdependence theory (Thibaut & Kelley, 1978), these results suggest that couple communication is greater than the sum (or in this case, the average) of its parts.
Across the communication ratings we examined, links with relationship outcomes were most consistent for constructive communication (i.e., rated relationship quality, positive reciprocity, and vulnerability/empathy). These findings contribute to a pattern across published work from the current sample, in that observed constructive communication is more consistently associated with long-term outcomes than is destructive communication. In addition to the current study three other published works examined associations between observed constructive and destructive aspects of communication and relationship outcomes in the current sample (i.e., K.J.W. Baucom et al., 2011; K.J.W. Baucom et al., 2012; Sevier et al., 2008). In total, these four studies examined associations between relationship outcomes at three different time points (post-therapy, 2-year follow-up, 5-year follow-up) and five constructive as well as six destructive aspects of communication. There were a grand total of 76 hypothesis tests of associations involving constructive communication and 78 hypothesis tests of associations involving destructive communication. The proportion of significant findings involving constructive communication (42.1%) was significantly higher than the proportion of significant findings involving destructive communication (12.8%), χ2(1) = 16.64, p < .001.
In examinations of observed individual communication in this sample, greater increases in positivity and problem solving from pre-therapy to post-therapy were consistently associated with concurrent improvements in relationship satisfaction (Sevier et al., 2008), and both higher post-therapy levels and greater increases in these same communication variables were associated with superior 2- and 5-year outcomes (K.J.W. Baucom et al., 2011). Increases in individual partner negativity, but not withdrawal, from pre-therapy to post-therapy were associated with concurrent improvements in relationship satisfaction (Sevier et al., 2008). Only higher post-therapy levels of wife negativity and increases in husband withdrawal from pre-therapy to post-therapy were associated with wife satisfaction at 2-year follow-up but there were no other significant associations between destructive communication and 2- and 5-year relationship outcomes (K.J.W. Baucom et al., 2011). Finally, in our examination of the validity of naïve ratings of dyadic communication, increases in relationship satisfaction were strongly related to increases in both rated relationship quality and positive reciprocity, and to a lesser extent to decreases in negative reciprocity, HD/WW, and WD/HW (K.J.W. Baucom et al., 2012).
Taken together, this pattern of findings across four examinations of observed communication offers strong support for the role of constructive communication in the long-term outcomes of couples following behavioral couple therapy. Previous treatment outcome research has generally demonstrated improvements in both constructive and destructive communication, but associations with relationship outcomes are generally weak across type of communication (Snyder, Castellani, & Whisman, 2006). The current findings, in combination with basic longitudinal (Johnson et al., 2005) and meta-analytic (Woodin, 2011) work, provide support for an increased focus on constructive aspects of communication in couple interactions.
Of note, we found virtually no support for associations between communication changes from post-therapy to 2-year follow-up and relationship outcomes. Many of the couples who had poor outcomes did not participate in the observational assessment at 2-year follow-up due to separation or divorce, a fact that may have limited our ability to detect links between this observational assessment and relationship outcomes. Despite this possibility, the significant Hypothesis 2 associations between relationship outcomes and communication changes from post-therapy to 2-year follow-up that were found in the current study were largely in the opposite direction of our predictions. Couples that remained together and those that responded well to therapy did not evidence respective changes in either direction in WD/HW or vulnerability/empathy over this time period. However, couples that later divorced and nonresponders to therapy evidenced significant decreases in WD/HW and increases in vulnerability/empathy, respectively. This is surprising and contrary to behavioral models of couple therapy as well as our hypothesis. One potential explanation for these findings is that these couples, having expended a great deal of time and energy in couple therapy to improve their relationship without a positive outcome, yet still together to participate in the 2-year follow-up assessment, are in a state of resignation. As such, they may evidence less maladaptive (WD/HW) and more adaptive communication (vulnerability/empathy) at 2-year follow-up relative to post-therapy because they have given up the fight for their relationship. Some support for this notion is gained from the fact that couples with missing data at 2-year follow-up evidenced lower levels of vulnerability/empathy at post-therapy relative to those with complete data. Post hoc hypothesis tests clarified that, although couples with poor long-term outcomes evidenced some improvements in communication after therapy ended, their final levels of communication and improvements over the course of all three time points were not superior to those with good long-term outcomes.
There are several important strengths of the observational methods employed in this study that increase our confidence in the results. First, we examined dyadic rather than individual communication, with a primary focus on patterns of interaction. These ratings of the overall extent to which a consequential behavior by one partner followed an initial behavior of the other (e.g., one partner’s negativity following the other’s negativity in negative reciprocity) offer a unique perspective on couple interactions that traditional observational systems are unable to directly capture. Second, the reliance on intuitive judgments of raters increases the likelihood that the NORS could be used in clinical practice, where the time to learn and apply traditional observational methods is often not feasible (Snyder, Heyman, & Haynes, 2005). Third, the manner in which judgments were made in the current study likely optimized the intuitive ability of naïve raters. Ratings for a given couple from all three time points were completed in one sitting. For example, a naïve rater might observe communication in pre-therapy, 2-year follow-up, and post-therapy husband’s topic for couple 105 before rating a different couple. The examination of a given type of interaction at all three time points in succession for a given couple may have allowed raters in the current study to make finer distinctions in communication at each time point.
Despite strengths, our results should be considered in the context of some limitations. First, we consider the pattern of missing observational data at 2-year follow-up to be missing not at random or nonignorable (Schafer & Graham, 2002), which may have impacted our results. These data likely produced more generous Hypothesis 1 estimates of improvements in communication from post-therapy to 2-year follow-up than we would find if the couples with the lowest relationship functioning (i.e., those who divorced) had complete data. Furthermore, the limited range of observational data at the 2-year follow-up may have reduced the likelihood of detecting links between this assessment and relationship outcomes. Second, the inter-rater reliabilities of communication scores were not uniformly high. The demand/withdraw and vulnerability/empathy scores’ reliabilities were below .7. Although scores on single-item measures have lower reliability than multi-item scales, the reliability coefficient constrains the strength of links with other variables (Schmitt, 1996). It is therefore possible that our results produced underestimates of links between communication and other variables in the study. Third, we were only able to control for individual communication in two of the six ratings in the current study. Although results suggesting that negative reciprocity and positive reciprocity are associated with relationship outcomes even after controlling for couple-average individual communication are encouraging, we cannot be certain that this would be the case for other forms of individual communication (e.g., vulnerability/empathy). Last, the couples in the current sample were relatively non-diverse. All couples were married, and the overwhelming majority of couples identified as Caucasian, middle-class, and well-educated. Thus, there are limitations to the generalizability of our findings given the demographic characteristics of our sample.
Conclusions
This examination of observed dyadic communication across three time points in a large sample of couples undergoing behavioral couple therapy makes several contributions to relationship research. First, it demonstrates the utility of measuring communication at the level of the couple. Second, it adds to the burgeoning area of research on the utility of untrained ratings of behavior (e.g., Waldinger et al., 2004). Third, it builds on previous investigations of communication changes following treatment termination (K.J.W. Baucom et al., 2011) and provides strong support for differential trajectories of change produced by TBCT and IBCT, but similar levels of communication in the final assessment. Finally, it adds to research on links between communication and outcome over the longest period of follow-up assessment in a randomized clinical trial of behavioral couple therapy to date.
Highlights.
We examine changes in communication over 3 time points in behavioral couple therapy
Couple-level communication rated by naïve (untrained) raters
We examine communications’ associations with 5-year relationship variables
Trajectories of change in communication depend on therapy type
Acknowledgments
We would like to thank Benjamin Karney, Theodore Robles, and Megan Sweeney for their comments on an earlier draft of this manuscript.
This research was supported by research grants to Andrew Christensen at UCLA (MH56223) and Neil S. Jacobson at the University of Washington (MH56165) for a two-site clinical trial of couple therapy. After Jacobson’s death, William George served as PI at the University of Washington. The preparation of this manuscript was supported by fellowships awarded to Katherine J.W. Baucom (F31HD062168) and Brian R. Baucom (F32HD060410) from the Eunice Kennedy Shriver National Institute of Child Health & Human Development. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The Association for Behavioral and Cognitive Therapies’ Virginia Roswell Dissertation Award, received by the first author in 2011, also supported this study.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
We use the term “naïve raters” to indicate naïveté with respect to research on couples and training in traditional observational systems. However, we think it is this very naïveté that allows for quite sophisticated intuitive judgments of communication that cannot be made with traditional systems (see K.J.W. Baucom et al., 2012, for discussion of this methodology).
Post-therapy data from one additional IBCT couple was included in this paper. Although the video equipment failed in their post-therapy assessment the raters in the current study evaluated communication based on an audio recording.
We ran a series of post hoc tests to determine whether there were pre-therapy or post-therapy differences in communication between couples that completed the 2-year follow-up observational assessment and those who did not. There were no pre-therapy differences between couples with missing 2-year data and those with complete data. Only vulnerability/empathy differed between groups at post-therapy (p < .05), such that couples with missing 2-year data evidenced lower levels of vulnerability/empathy at post-therapy than those with complete data.
Vulnerability/empathy increased from pre-therapy to 2-year follow-up in severely distressed IBCT and TBCT couples (ps < .05) but did not change in moderately distressed couples. HD/WW only decreased in severely distressed IBCT couples and moderately distressed TBCT couples (ps < .01).
Due to the small number of couples in each cell for tests of simple effects we were unable to examine whether associations of interest differed by treatment type and/or pre-therapy distress stratification in Hypothesis 2.
References
- Baker JK, Haltigan JD, Brewster R, Jaccard J, Messinger D. Non-expert ratings of infant and parent emotion: Concordance with expert coding and relevance to early autism risk. International Journal of Behavioral Development. 2010;34:88–95. doi: 10.1037/a0021275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bandura A. Social Learning Theory. New York: General Learning Press; 1977. [Google Scholar]
- Baucom DH, Hahlweg K, Kuschel A. Are waiting-list control groups needed in future marital therapy outcome research? Behavior Therapy. 2003;34:179–188. doi: 10.1016/S0005-7894(03)80012-6. [DOI] [Google Scholar]
- Baucom DH, Sayers SJ, Sher TG. Supplementing behavioral marital therapy with cognitive restructuring and emotional expressiveness training: An outcome investigation. Journal of Consulting and Clinical Psychology. 1990;58:636–645. doi: 10.1037/0022-006X.58.5.636. [DOI] [PubMed] [Google Scholar]
- Baucom KJW, Baucom BR, Christensen A. Do the naïve know best? The predictive power of naïve ratings of couple interactions. Psychological Assessment. 2012;24:983–994. doi: 10.1037/a0028680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baucom KJW, Sevier M, Eldridge KA, Doss BD, Christensen A. Observed communication in couples two years after Integrative and Traditional Behavioral Couple Therapy: Outcome and link with 5-year follow-up. Journal of Consulting and Clinical Psychology. 2011;79:565–576. doi: 10.1037/a0025121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christensen A. Unpublished document. University of California; Los Angeles: 2006. The Naïve Observational Rating System. [Google Scholar]
- Christensen A, Atkins DC, Baucom BR, Yi J. Marital status and satisfaction 5 years following a randomized clinical trial comparing Traditional versus Integrative Behavioral Couple Therapy. Journal of Consulting and Clinical Psychology. 2010;78:225–235. doi: 10.1037/a0018132. [DOI] [PubMed] [Google Scholar]
- Christensen A, Atkins D, Berns S, Wheeler J, Baucom D, Simpson LE. Traditional versus integrative behavioral couple therapy for significantly and chronically distressed married couples. Journal of Consulting and Clinical Psychology. 2004;72:176–191. doi: 10.1037/0022-006X.72.2.176. [DOI] [PubMed] [Google Scholar]
- Halford WK, Sanders MR, Behrens BC. A comparison of the generalization of behavioral marital therapy and enhanced behavioral marital therapy. Journal of Consulting and Clinical Psychology. 1993;61:51–60. doi: 10.1037/0022-006X.61.1.51. [DOI] [PubMed] [Google Scholar]
- Hahlweg K, Revenstorf D, Schindler L. Effects of behavioral marital therapy on couples’ communication and problem solving skills. Journal of Consulting and Clinical Psychology. 1984;52:553–566. doi: 10.1037/0022-006X.52.4.553. [DOI] [PubMed] [Google Scholar]
- Heavey CL, Gill D, Christensen A. Unpublished document. University of California; Los Angeles: 1998. The Couple Interaction Rating System. [Google Scholar]
- Heyman RE. Observation of couple conflicts: Clinical assessment applications, stubborn truths, and shaky foundations. Psychological Assessment. 2001;13:5–35. doi: 10.1037//1040-3590.13.1.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacobson NS, Christensen A. Acceptance and change in couple therapy: A therapist’s guide to transforming relationships. New York: Norton; 1998. [Google Scholar]
- Jacobson NS, Margolin G. Marital therapy: Strategies based on social learning and behavior exchange principles. New York: Brunner/Mazel; 1979. [Google Scholar]
- Jacobson NS, Truax P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychology. 1991;59:12–19. doi: 10.1037/0022-006X.59.1.12. [DOI] [PubMed] [Google Scholar]
- Johnson MD, Cohan CL, Davila J, Lawrence E, Roggee RD, Karney BR, Bradbury TN. Problem-solving skills and affective expressions as predictors of change in marital satisfaction. Journal of Consulting and Clinical Psychology. 2005;73:15–27. doi: 10.1037/0022-006X.73.1.15. [DOI] [PubMed] [Google Scholar]
- Jones JT, Christensen A. Unpublished document. University of California; Los Angeles: 1998. The Social Support Interaction Rating System. [Google Scholar]
- Kerig PK, Baucom DH. Couple observational coding systems. New Jersey: Lawrence Erlbaum; 2004. [Google Scholar]
- Kline GH, Julien D, Baucom BR, Hartman S, Gilbert K, Gonzalez T, Markman HJ. The Interactional Dimensions Coding System (ICDS): A global system for couple interactions. In: Kerig PK, Baucom DH, editors. Couple observational coding systems. New Jersey: Lawrence Erlbaum; 2004. pp. 113–126. [Google Scholar]
- Laurenceau JP, Stanley SM, Olmos-Gallo A, Baucom B, Markman HJ. Community-based prevention of marital dysfunction: Multilevel modeling of a randomized effectiveness study. Journal of Consulting and Clinical Psychology. 2004;72:933–943. doi: 10.1037/0022-006X.72.6.933. [DOI] [PubMed] [Google Scholar]
- Lorber MF. Can minimally trained observers provide valid global ratings? Journal of Family Psychology. 2006;20:335–338. doi: 10.1037/0893-3200.20.2.335. [DOI] [PubMed] [Google Scholar]
- Margolin G, Wampold BE. Sequential analysis of conflict and accord in distressed and nondistressed marital partners. Journal of Consulting and Clinical Psychology. 1981;49:554–567. doi: 10.1037/0022-006X.49.4.554. [DOI] [PubMed] [Google Scholar]
- Raudenbush SW, Bryk AS, Cheong YF, Congdon RT, du Toit M. HLM 7: Hierarchical Linear and Nonlinear Modeling. Lincolnwood, IL: SSI; 2011. [Google Scholar]
- Schafer JL, Graham JW. Missing data: Our view of the state of the art. Psychological Methods. 2002;7:147–177. doi: 10.1037/1082-989X.7.2.147. [DOI] [PubMed] [Google Scholar]
- Schmitt N. Uses and abuses of coefficient alpha. Psychological Assessment. 1996;8:350–353. doi: 10.1037/1040-3590.8.4.350. [DOI] [Google Scholar]
- Sevier M, Eldridge K, Jones J, Doss BD, Christensen A. Observed changes in communication during Traditional and Integrative Behavioral Couple Therapy. Behavior Therapy. 2008;39:137–150. doi: 10.1016/j.beth.2007.06.001. [DOI] [PubMed] [Google Scholar]
- Snyder DK. The Marital Satisfaction Inventory – Revised. Los Angeles: Western Psychological Services; 1997. [Google Scholar]
- Snyder DK, Castellani AM, Whisman MA. Current status and future directions in couple therapy. Annual Review of Psychology. 2006;57:317–44. doi: 10.1146/annurev.psych.56.091103.070154. [DOI] [PubMed] [Google Scholar]
- Snyder DK, Heyman RE, Haynes SN. Evidence-based approaches to assessing couple distress. Psychological Assessment. 2005;17:288–307. doi: 10.1037/1040-3590.17.3.288. [DOI] [PubMed] [Google Scholar]
- Spanier GB. Measuring dyadic adjustment: New scales for assessing the quality of marriage and similar dyads. Journal of Marriage and the Family. 1976;38:15–28. doi: 10.2307/350547. [DOI] [Google Scholar]
- Thibaut JW, Kelley HH. Interpersonal relations: A theory of interdependence. New York: Wiley; 1978. [Google Scholar]
- Waldinger RJ, Schulz MS, Hauser ST, Allen JP, Crowell JA. Reading others’ emotions: The role of intuitive judgments in predicting marital satisfaction, quality, and stability. Journal of Family Psychology. 2004;18:58–71. doi: 10.1037/0893-3200.18.1.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woodin EM. A two-dimensional approach to relationship conflict: Meta-analytic findings. Journal of Family Psychology. 2011;25:325–335. doi: 10.1037/a0023791. [DOI] [PubMed] [Google Scholar]