

Abstract
Anterior cruciate ligament injury and the associated long-term sequelae, such as immediate reductions in physical inactivity, increased adiposity and increased risk of osteoarthritis throughout adulthood, are a major health concern for adolescent athletes. Current interventions for injury prevention may have limited effectiveness, are susceptible to issues of compliance and have not achieved the widespread acceptance necessary to promote full adoption. Neuromuscular training (NMT) is a well-established training intervention introduced to affect change in modifiable biomechanical risk factors to reduce the risk of injury in these athletes. Despite moderate success, neuromuscular training is still limited by its reliance on subjective feedback and after the fact (i.e., offline) objective feedback techniques. The purpose of this commentary is to discuss technological tools that could be used to enhance and objectify targeted biofeedback interventions to complement NMT. Electromyography, force plates, motion sensors, and camera-based motion capture systems are innovative tools that may have realistic feasibility for integration as biofeedback into NMT programs to improve training outcomes. Improved functional deficit identification and corrective analysis may further improve and optimize athletic performance, and decrease the risk of sports-related injury during sport performance.
Key points.
Specific, targeted interventions that isolate injury risk factors and can help correct modifiable neuromuscular deficits are essential.
Current training interventions for anterior cruciate ligament (ACL) injury prevention have only demonstrated limited effectiveness and have not achieved the widespread acceptance necessary to promote full adoption to reduce ACL injury rates.
The paper provides an overview of innovative strategies and technological tools that could be used to enhance and objectify targeted biofeedback interventions to complement neuromuscular training (NMT) including electromyography, force plates, motion sensors, and camera-based motion capture systems.
These strategies utilize biomechanical, physiological, or neuromotor variables for training, automate the quantitative measurement of those variables through a variety of technological modalities, and then feed those measured variables via software to provide information in simplified form for online, visual biofeedback displays.
Key words: Neuromuscular training, anterior cruciate ligament injury, biofeedback, electromyography, force platforms, motion sensors, 3D motion capture
Introduction
Anterior cruciate ligament (ACL) injuries are debilitating to adolescent athletes, and these injuries create short- and long-term pain and disability for individuals throughout the processes of reconstructive surgery, rehabilitation, return to sport, and the maintenance of a healthy, active lifestyle into adulthood. This, combined with a strong association that links ACL injury to the development of post-traumatic knee osteoarthritis at a relatively young age, evidences a tremendous need for interventions that reduce the risk and contribute to both primary and secondary injury prevention as it relates to ACL injuries. Unfortunately, current standardized interventions are largely inefficient at relative risk reduction (Sugimoto et al., 2012) and are susceptible to non-compliance (Sugimoto et al., 2012). In response to these issues, neuromuscular training (NMT)—a targeted set of strength and conditioning activities that promote correct movement technique and competence—was developed and has demonstrated proven injury risk factor reduction benefits (Myer et al., 2011b; 2013a).
A primary component of NMT is training instruction and feedback from qualified and specially trained instructors. Standard NMT provides verbal feedback after the movement has been completed based on what the instructor might subjectively decide is the most egregious error in movement. It also encourages the athlete to explicitly focus attention internally on bodily movement patterns despite the preponderance of evidence that externally focused attention provides more robust motor learning outcomes (Benjaminse and Otten, 2011; Gokeler et al., 2013). Thus, injury prevention effects of NMT have only been modest and there is a need to more effectively and objectively guide an athlete to improve movement technique to further reduce injury risk (Myer et al., 2013b).
To combat this, effective biofeedback should be premised on the principle that sensorimotor learning and performance are enhanced when trainees focus attention on the external consequences of their actions rather than on their limbs, segments or joints (McNevin et al., 2003; Shea and Wulf, 1999; Wulf, 2013; Wulf and McNevin, 2003; Wulf and Prinz, 2001; Wulf et al., 2001; 2002; 2010). These two principles stem from the natural linkage between neuromuscular actions and their perceptual outcomes (i.e., the perception-action cycle) and the robustness of automatic, implicit motor learning and control processes compared to conscious, effortful motor control, which is relatively fragile and inefficient. One potential limitation of current injury prevention programs could be a deficiency in the transition from conscious awareness of desired biomechanical adaptations achieved during training sessions to unexpected and automatic movements required for athletic activities on the field (Benjaminse and Otten, 2011). Learning strategies with an internally directed focus have traditionally been utilized, but those may be less suitable for the acquisition of the control of complex motor skills required for transfer into sport (Benjaminse and Otten, 2011; Gokeler et al., 2013). A second and related potential limitation is that verbal feedback (subjective and internally focused) may be more difficult and less effective for athletes to translate into neuromuscular adaptive strategies than visual biofeedback. (Benjaminse and Otten, 2011; Gokeler et al., 2013; Myer et al., 2013a) Accordingly, analytic-driven, implicit and external biofeedback techniques may have the potential overcome these practice barriers.
The focus of this commentary is to outline the utility for new and existing technologies that can provide the potential to remedy current limitations of NMT for injury prevention. The core concept of these strategies is to augment NMT through the selection of key biomechanical, physiological, or neuromotor variables for training through the automation of the quantitative measurement of those variables using a variety of technological modalities. This allows for the transformation of those measured variables to provide information in simplified form for real-time (i.e., online), visual biofeedback displays. The use of objective, real-time visual stimuli is an important component for delivery of feedback during NMT that oftentimes provides a more salient and effective form of corrective instruction than verbal or auditory feedback. (Moleiro and Cid, 2001) This is due, in large part, to the fact that the visual system is known to be a powerful pattern recognition system, and visual perception translates easily into modulations of behavior. (Meijer & Roth, 1988) In the following sections we discuss measurement and biofeedback-capable tools, including electromyography (EMG), force sensors and force platforms, inertial sensors, and camera-based motion capture systems that can be used to augment existing NMT feedback protocols. The choice of technology depends largely on the details of the training protocol, the specific exercises employed and, in the case of highly individualized training, the particular movement deficits of each athlete.
EMG
EMG is a measurement tool used to record the electrical activity produced by a specific muscle or group of muscles. (De Luca, 1997) The information provided by EMG signifies the degree to which a muscle is active. The electrical activity is recorded via surface electrodes that are placed on the skin, or less commonly via intramuscular needle electrodes, and muscle activation is characterized through detection of electrical potentials of neurally activated muscle cells. Thus, EMG provides an objective measurement of muscle activation level and recruitment order for biomechanical movement analysis (Robertson et al., 2013). These patterns of muscle activations can be converted into visual and/or auditory signals and can be observed by the clinician or instructor, and as feedback by the patient or athlete.
Applications of EMG to Augment NMT: EMG-based feedback can be utilized to improve muscle recruitment and thus technique during NMT. Feedback after the task (i.e., offline feedback) can be utilized to aid a practitioner in corrective intervention, but EMG is perhaps most useful in that it can provide online feedback to an athlete during a variety of movements to promote correct muscle activation and recruitment above and beyond classic offline, instructor-based feedback. For example, a fundamental NMT exercise and precursor to more intense exercise variation is the basic unloaded bilateral squat (Myer et al., 2008b). The squat requires the activation of specific muscles (i.e., the gluteals, hamstrings, and quadriceps) in correct sequences and ratios for optimal performance technique. (Schoenfeld, 2010) Classically, a trainer observes the maneuver and provides subjective, verbal feedback during and after the athlete performs the squat. The feedback often varies from instructor to instructor and the competency of the trainer can limit corrective outcome potential. (Myer et al., 2013a) Alternatively, stimuli based on EMG data would allow for analytic-driven, objective feedback as a supplement to trainer responses. In this context, the athlete would perform a vertical squat jump with the surface electrodes placed on her hamstrings, gluteals, and quadriceps. The relative activation and location of muscle activation would be visualized on a display to allow for the self-adjustment of muscle contractions in order to achieve the desired technique. For example, a display could map the EMG activation values for each muscle group as angles that form a triangle, and the athlete’s task would be to “control” the shape of the triangle (by contracting the muscles in the right order and to the right degree so that the triangle, which transforms in real time as a function of muscle group activation, exhibits equilaterality (see Figure 1 for an example). To simplify the task for the athlete, a template triangle could be displayed, and the task would be to match the shape of the stimulus to the template.
Figure 1.
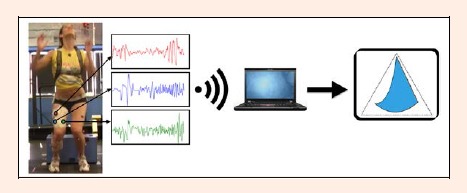
A schematic of how real-time EMG biofeedback might be utilized. The athlete is preparing for a full effort vertical jump as part of the drop vertical jump as the EMG activity is recorded at three sites (far left). This data is streamed in real-time to a PC where the data are converted into a dynamic stimulus (in this case a triangle shape) in which the three angles of intersection correspond with values of muscle activation. The goal in this case is for the athlete to “animate” a shape that matches the black outline of the equilateral triangle (far right).
Force Platforms and Sensors
Force measurement systems quantify the force that is generated by the body, generally at the feet, and can give feedback on an athlete’s force production and balance in the context of postural control, jumping and landing, and gait. The most basic force sensors measure the vertical components of force, while more advanced force platforms are able to provide multi-axis data in three dimensions (vertical, medial-lateral, and anterior-posterior). Force plate data allow for the calculation and extrapolation of acceleration, work, power output, jump angle, and jump distance. When combined with motion capture systems that capture spatial kinematics and relative joint angles (discussed later), additional inverse dynamic calculations of torque, work and power at each joint can be quantified.
Force feedback can be delivered via a visual display on a computer screen that demonstrates the changes in force output. (Barclay-Goddard et al., 2004) Traditionally, force plate systems have been restricted to laboratory or clinical environments due to high costs of the equipment and required accessories. More recently, however, the introduction of force measurement technology to game and entertainment platforms such as the Wii Balance Board™ by Nintendo™ provides consumer-grade technologies for real-time force feedback. Researchers have already begun to validate these technologies (Clark et al., 2010) and such devices have resulted in significant cost reductions and increased availability of force measurement systems in myriad contexts by the general population.
Applications of Force Platforms to Augment NMT: NMT currently utilizes force plates to identify ground reaction force (GRF) asymmetries before, during, and after training to quantify performance progress (Hewett et al., 2005; Myer et al., 2006). Thus, there are several possible applications of force feedback during NMT, predominantly during plyometric exercises (Myer et al., 2008b), to teach the athlete how to modulate force production during takeoff and force absorption during landing. Force plates can also support the optimization of postural control and balance. For example, offline force feedback has been utilized during performance of the tuck jump (Myer et al., 2008a; Myer et al., 2011a; Stroube et al., 2013). The tuck jump exercise involves repetitive vertical jumps where the athlete immediately brings the knees up toward the chest after takeoff. Force plates underneath the landing zone can enable GRF measurement and thus feedback of forces to provide information relative to excessive landing forces (i.e., lack of knee bend or force absorption at the ankle), landing force asymmetries, and overall balance during takeoff and landing (Myer et al., 2005; Paterno et al., 2004). Offline feedback could be replaced by online feedback during NMT to potentially enhance the effectiveness of this exercise. Similarly, online biofeedback could be utilized during a systematic plyometric exercise like the tuck jump—a series of repeated vertical jumps where the knees are pulled up as high as possible while airborne—as instantaneous feedback can be utilized to modify technique during consecutive jumps (Stroube et al., 2013). A visual display that provides the GRF and vector for each extremity provides a real-time evaluation of symmetry between limbs. In addition, a display that provides information relative to the athlete’s center of gravity—information that cannot be seen or observed by the naked eye under normal training—can be utilized to train the proper loading of the hips and spine (Figure 2; Benjaminse and Otten, 2011). Force feedback can be utilized in conjunction with another measurement device such as motion capture or EMG in order to gather additional data about the body in space rather than just the forces that the body exerts on the ground.
Figure 2.
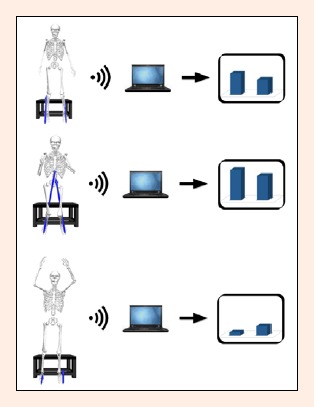
The GRF as represented by the blue arrows that originate at each foot for three phases of the drop vertical jump and a corresponding bar graph feedback display for each movement phase. The athlete is instructed to match the height of the bars throughout the movement.
Inertial Sensors (Accelerometers and Gyroscopes)
Inertial sensors, such as accelerometers and gyroscopes—the latter of which are devices that measure orientation based on the principles of angular momentum—measure information related to the motion of body segments, such as acceleration and orientation. (Schepers, 2009) These sensors have become miniaturized and more cost-effective over the last decade, primarily given their application in smart phones and tablets, and this has led to numerous applications in fitness tracking devices, as discussed below.
Applications of Inertial Sensors to Augment NMT: Most often, standard NMT is conducted in a formal training center and often requires a laboratory or clinical setting to provide precise forms of feedback and instruction. Thus, the number of training sessions and the lack of qualified supervision when the athlete goes home limit both types of training. Accelerometers may therefore have enormous potential in their ability to monitor and promote physical activity outside of a training or laboratory facility. For example, an athlete may attend NMT to improve activity levels for pre-season conditioning, and as part of their program an accelerometer device could monitor the athlete’s physical activity levels and alert them, their parent(s), and even the training professional to the athlete’s activity levels and quality of adherence. Advanced pedometers offer audible measures of tempo that can promote higher frequency movements, and provide auditory cues during training to indicate the transition between various tasks (e.g., running, jumping, stepping, etc.).
These types of sensors can also provide real-time movement correction feedback during NMT. Accelerometers can be attached to multiple body segments to track movement frequencies and acceleration patterns in order to improve movement efficiency. For example, an athlete can be presented with visual feedback as to whether their limb accelerations are symmetric, and can correct accelerations in real-time during repetitive exercises like the tuck jump. Similarly, gyroscopes can provide feedback for the appropriate orientation of the trunk during these types of maneuvers. Much like a spirit level or bubble level used in construction, feedback displays could provide information as to where the athlete’s balance is located within a visual base of support (see Figure 3). As an athlete lands and attempts to stabilize their balance, this type of feedback can allow them to train stabilizing muscle groups for more efficient and effective balance control.
Figure 3.
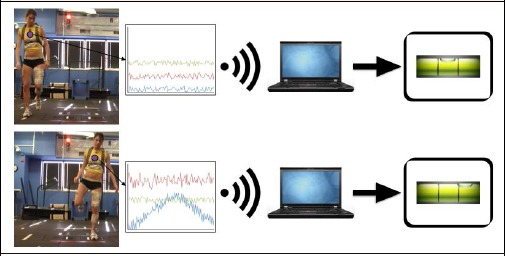
A lateral jump and hold task in which the athlete stands on the right leg (left) and then jumps laterally (middle) and lands on a predefined point on the floor with the opposite leg (right). During this task it is possible to compute a center of mass through the use of an accelerometer or gyroscrope and display a bubble level type of display to orient the athlete to her balance performance throughout the trial. The goal of this task is to keep the bubble in the center of the bubble level display.
Camera-based 3D Motion Capture
Camera-based motion capture systems enable the objective examination of movement patterns, as opposed to standard video cameras that allow for qualitative assessment of motion and less refined 2-D kinematic measurements. Thus, camera based systems can be divided into two separate groups: 2D video and 3D motion capture systems. Our focus here will be on 3D motion capture systems: While 2D systems have some utility as well, their potential for real-time biofeedback is limited. Typically, 3D tracking systems quantify movement through the detection of a series of markers placed on the body of a patient or athlete. In passive motion capture systems, infrared light is sent out from each camera and reflected back via highly reflective markers attached to the body segments of the user. Active motion capture systems work similarly but the markers emit infrared signals that are detected by the cameras and provide high-fidelity kinematic data to facilitate a more detailed observation of movement at variable scales, angles, and speeds.
Applications of 3D Motion Capture to Augment NMT: With regard to NMT, motion capture-based NMT that utilized offline feedback has already demonstrated to lead to improved limb symmetry and a reduction in joint-position risk during landing tasks, and this has led to a significant reduction in lower musculoskeletal injuries. (Hewett et al., 1999) Real-time biofeedback based on motion capture data may be even more effective. For example, real-time biofeedback was used to successfully modify performance of a repetitive double leg squat. Subjects were delivered either kinetic or kinematic biofeedback via a monitor that displayed a real-time animation of the subject, and a data curve with a highlighted goal region for the subject to achieve via technique modification (Figure 4; Ford et al., 2014). Subjects were able to significantly improve their technique for both kinetic and kinematic technique with this system.
Figure 4.
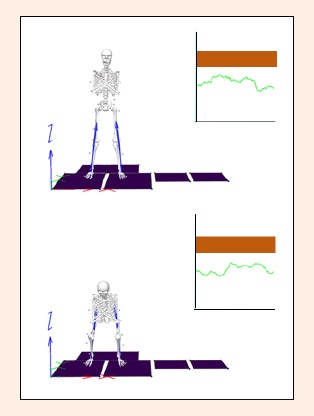
Real-time feedback of the right knee moment during a standing squat maneuver. The shaded region on the plot represents the target knee moment and the time series data represents the participant’s actual knee moment. The vertical pointing arrows that originate at the skeleton’s feet represent the GRF for each foot. In this case the athlete is not executing the movement within the targeted range, as computed via the hip moment.
3D motion capture has been utilized to facilitate learning of complex, whole-body, closed-chain movement tasks (Faugloire et al., 2005). In the context of postural control, participants were tasked with learning to produce dynamic postural coordination patterns of the lower leg and trunk about the ankle and hip joints (Faugloire et al., 2005). Rather than instructing subjects explicitly to perform specific coordination patterns, they were simply instructed to view an online feedback display and discover how to move the body so as to create either a circular pattern or downward-sloping diagonal line. The feedback display was, unbeknownst to participants, a simple angle-angle diagram (ankle vs. hip joint rotations). In the joint angle space, the goal circular shape corresponded to in-phase (0° relative phase angle) ankle-hip coordination and the diagonal line to anti-phase (180° relative phase angle) ankle-hip coordination. Participants quickly learned to produce the ankle-hip coordination patterns by “drawing” the desired shapes in the feedback display. Those participants who had this feedback available produced better postural coordination patterns faster than those who did not. Moreover, when stroke patients performed this task as a balance intervention they showed long-lasting improvements in balance performance (Varoqui et al., 2011). In the future, such a protocol could be expanded in NMT as participants “control” the shape of a feedback stimulus to guide the acquisition of desired biomechanical profiles. This type of application during dynamic activities, for example, can allow for fine-grained adjustments of the athlete’s lower limbs in real-time and lead to a fun, motivational game of self-correction independent of the instructor. It also promotes implicit, externally focused training that is known to enhance motor learning and skill transfer to sport (Benjaminse and Otten, 2011; Gokeler et al., 2013).
A limiting factor for these types of applications at present is cost and lack of portability to the home or school setting. With the advent of Microsoft Kinect™ and Kinect for Xbox One™, these new systems may facilitate the arrival of 3D motion capture as a training tool for the general population. Microsoft’s Kinect Deep Camera Technology™ offers a real solution and efforts are already underway to utilize this technology for range of motion measurements in clinical settings (Barandas, 2013). However, it is important to note that the Kinect™ has demonstrated to be an order of magnitude less accurate than more expensive, laboratory motion capture technologies (Dutta, 2012). Thus, while the Kinect is an important step for the portability of these technologies, and may provide a useful, cost-effective system for off-site NMT training and feedback, it should be employed with caution.
Visual Display Techniques to Deliver Biofeedback
The proposed approach to provide feedback to athletes through the use of visual displays requires discussion relative to the display medium through which such feedback can be utilized. Traditional approaches have incorporated computer monitors and projector screens for the display of video feedback, including our own recent work (Ford et al., 2014; Myer et al., 2008b; 2011b; 2013; Stroube et al., 2013). While the usefulness of these displays is obvious, they are limited in their position relative to the athlete. The very nature of the stationary position of the display has the potential to negatively influence the movement patterns during performance of a given task. For example, an athlete performing a drop vertical jump task is forced to fixate on the screen in front of them, thus modifying their head position in a way that may be sub-optimal for efficient performance. Moreover, such displays limit where the athlete can perform the task, may take up valuable real estate in a laboratory or training setting, and may not provide a compelling, immersive experience for the athlete, which could negatively affect adherence.
New, highly innovative alternatives to such limitations are augmented reality (i.e., see-through) and smart-eye heads-up displays (HUDs). These HUDs are light-weight, low-profile sport-style glasses that enable the child to move freely in the training environment with a display that is easily accessible by adjusting the gaze of their right eye either up or down to a miniature screen display mounted just outside their central field of view (see Figure 5). The benefits of such a display are numerous and include the ability to move freely during training, a personalized training display simultaneously for every athlete during group training, the ability to interact with other athletes and instructors without visual occlusion, and the ability to take such a display outside and onto the field of play with minimal impact on the child’s movements. Such displays are becoming more cost-effective by the day (i.e., Recon Instruments’ Jet HUD™) and provide an efficient method to provide feedback during NMT.
Figure 5.
A schematic of a smart-eye display (in this case, Google GlassTM) as worn by an athlete, and as viewed from the front (left) or from inside the display (right). The display can be either transparent as is the case here or, alternatively, a small monitor-like display that is opaque. Heads-up displays such as these may provide a more unobtrusive display for the relay of biofeedback to the athlete.
Conclusion
While the current evidence indicates that biofeedback is the critical component to success in interventions aimed to reduce injury, (Myer et al., 2005; 2013a; 2013b; 2013c), there is the potential that this commentary is open to bias as to the benefits of biofeedback. Thus, future research should target research questions specific to externally focused learning, and more generally with regard to biofeedback, in the context of neuromuscular training to elucidate the influence of biofeedback on injury prevention efforts. Regardless, the removal of barriers to feedback interventions (e.g., subjective, potentially erroneous or uninterpretable feedback) through the proposed real-time automated techniques that provide implicit, analytic-driven biofeedback may make it possible to significantly overcome current limitations. Specific targeted interventions that isolate injury risk factors and can help correct modifiable neuromuscular deficits are essential for prevention of ACL injury. NMT is a proven regimen that has been shown to reduce ACL injuries via analyses of the movement biomechanics and retrospective feedback to the athlete regarding proper body position and technique (Myer et al., 2013b). Traditionally, qualified instructors provide subjective feedback and awareness to an athlete during training. The initiation of real-time feedback throughout NMT may improve the intervention via the application of measurement technologies that could supplement instructor-based feedback practices. Through the use of these technologies it may be possible to provide more efficient and effective interventions that target and correct specific deficits with the additional benefit of engaging implicit, procedural learning techniques to direct the athlete’s attention externally toward the consequences of their movements. We have provided a review of what we believe to be the most promising of these tools, and ultimately, these technologies will likely need to be combined for optimal training outcomes. As manufacturing costs come down and these technologies continue to develop, instructors, parents and the adolescent athletes themselves will have a number of promising feedback devices for a well-rounded and effective training program designed to prevent injury and sustain a healthy, physically active lifestyle into and throughout adulthood.
Biographies
Adam W. KIEFER
Employment
Cincinnati Children’s Hospital Medical Center; University of Cincinnati College of Medicine; University of Cincinnati
Degree
PhD
Research interests
Augmented/virtual reality; behavioral dynamics; biofeedback; dynamical disease; eye tracking; individual/team coordination; nonlinear dynamics; quantitative methods; sports medicine
E-mail: adam.kiefer@cchmc.org

Adam KUSHNER
Employment
Cincinnati Children’s Hospital Medical Center
Degree
BSc, CSCS
Research interests
Neuromuscular training, knee injury prevention training, sports performance training, psychosocial implications of training youth
E-mail: adam.kushner@cchmc.org
John GROENE
Employment
University of Cincinnati College of Medicine
Degree
BSc
Research interests
Sports medicine, ACL injury prevention, concussion injury prevention
E-mail: groenejj@mail.uc.edu
Christopher WILLIAMS
Employment
University of Dayton
Degree
BSc
Research interests
Cardiopulmonary therapy, lymphatic therapy, fatigue mechanisms in high intensity training, fatigue mechanisms in neuromuscular training
E-mail: Williamsc30@udayton.edu

Michael A. RILEY
Employment
University of Cincinnati
Degree
PhD
Research interests
Sensorimotor control, behavioral dynamics, nonlinear dynamics, postural control, time series analysis
E-mail: michael.riley@uc.edu

Greg D. MYER
Employment
Cincinnati Children’s Hospital Medical Center; University of Cincinnati College of Medicine; The Ohio State University Medical Center; The Micheli Center for Sports Injury Prevention
Degree
PhD, FACSM, CSCS*D
Research interests
Neuromuscular training, augmented biofeedback, biomechanics of knee injury, sports performance, knee injury prevention training
E-mail: greg.myer@cchmc.org
References
- Barandas M.D.S.G. (2013) Range of motion measurements based on depth camera for clinical rehabilitation. Doctoral thesis. The Universidade Nova Lizbon; Avalibale form URL: http://run.unl.pt/handle/10362/11046. [Google Scholar]
- Barclay-Goddard R., Stevenson T., Poluha W., Moffatt M., Taback S. (2004) Force platform feedback for standing balance training after stroke. Cochrane Database of Systematic Reviews 4, 1-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benjaminse A., Otten E. (2011) ACL injury prevention, more effective with a different way of motor learning? Knee surgery, sports traumatology. Knee surgery, sports traumatology, Arthroscopy 19, 622-627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark R.A., Bryant A.L., Pua Y., Mccrory P., Bennell K., Hunt M. (2010) Validity and reliability of the Nintendo Wii Balance Board for assessment of standing balance. Gait & Posture 31, 307-310. [DOI] [PubMed] [Google Scholar]
- De Luca C. J.1997. The use of surface electromyography in biomechanics. Journal of Applied Biomechanics 13, 135-163. [Google Scholar]
- Dutta T. (2012) Evaluation of the Kinect sensor for 3-D kinematic measurement in the workplace. Applied Ergonomics 43, 645-649. [DOI] [PubMed] [Google Scholar]
- Faugloire E., Bardy B.G., Merhi O., Stoffregen T.A. (2005) Exploring coordination dynamics of the postural system with real-time visual feedback. Neuroscience Letters 374, 136-141. [DOI] [PubMed] [Google Scholar]
- Ford K.R., Dicesare C., Myer G.D., Hewett T.E. (2014) Real-Time Biofeedback to Target Risk of Anterior Cruciate Ligament Injury: A Technical Report for Injury Prevention and Rehabilitation. Journal of Sport Rehabilitation 23, 1-6. [DOI] [PubMed] [Google Scholar]
- Gokeler A., Benjaminse A., Hewett T.E., Paterno M.V., Ford K.R., Otten E., Myer G.D. (2013) Feedback techniques to target functional deficits following anterior cruciate ligament reconstruction: implications for motor control and reduction of second injury risk. Sports Medicine 43, 1065-1074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hewett T.E., Lindenfeld T.N., Riccobene J.V., Noyes F.R. (1999) The Effect of Neuromuscular Training on the Incidence of Knee Injury in Female Athletes A Prospective Study. The American Journal of Sports Medicine 27, 699-706. [DOI] [PubMed] [Google Scholar]
- Hewett T.E., Myer G.D., Ford K.R., Heidt R.S., Colosimo A.J., Mclean S.G., VanDen Bogert A.J., Paterno M.V., Succop P. (2005) Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. The American Journal of Sports Medicine 33, 492-501. [DOI] [PubMed] [Google Scholar]
- Meijer O.G., Roth K. (1988) Complex Movement Behaviour: ‘The'Motor-Action Controversy. Elsevier. [Google Scholar]
- Moleiro M.Á., Cid F.V. (2001) Effects of biofeedback training on voluntary heart rate control during dynamic exercise. Applied Psychophysiology and Biofeedback 26, 279-292. [DOI] [PubMed] [Google Scholar]
- Myer G.D., Brent J.L., Ford K.R., Hewett T.E. (2011a) Real-time assessment and neuromuscular training feedback techniques to prevent ACL injury in female athletes. Strength & Conditioning Journal 33, 21-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myer G.D., Faigenbaum A.D., Chu D.A., Falkel J., Ford K.R., BEST T.M., Hewett T.E. (2011b) Integrative training for children and adolescents: techniques and practices for reducing sports-related injuries and enhancing athletic performance. The Physician and Sports Medicine 39, 74-84. [DOI] [PubMed] [Google Scholar]
- Myer G.D., Ford K.R., Hewett T.E. (2008a) Tuck Jump Assessment for Reducing Anterior Cruciate Ligament Injury Risk. Athletic Therapy Today 13, 39-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myer G.D., Ford K.R., Mclean S.G., Hewett T.E. (2006) The effects of plyometric versus dynamic stabilization and balance training on lower extremity biomechanics. The American Journal of Sports Medicine 34, 445-455. [DOI] [PubMed] [Google Scholar]
- Myer G.D., Ford K.R., Palumbo J.P., Hewett T.E. (2005) Neuromuscular training improves performance and lower-extremity biomechanics in female athletes. The Journal of Strength & Conditioning Research 19, 51-60. [DOI] [PubMed] [Google Scholar]
- Myer G.D., Kushner A.M., Faigenbaum A.D., Kiefer A., Kashikar-Zuck S., Clark J.F. (2013a) Training the developing brain, part I: cognitive developmental considerations for training youth. Current Sports Medicine Reports 12, 304-10. [DOI] [PubMed] [Google Scholar]
- Myer G.D., Paterno M.V., Ford K.R., Hewett T.E. (2008b) Neuromuscular training techniques to target deficits before return to sport after anterior cruciate ligament reconstruction. The Journal of Strength & Conditioning Research 22, 987-1014. [DOI] [PubMed] [Google Scholar]
- Myer G.D., Stroube B.W., Dicesare C.A., Brent J.L., Ford K.R., Heidt R.S., Hewett T.E. (2013b) Augmented feedback supports skill transfer and reduces high-risk injury landing mechanics a double-blind, randomized controlled laboratory study. The American Journal of Sports Medicine 41, 669-677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myer G.D., Sugimoto D., Thomas S., Hewett T.E. (2013c) The influence of age on the effectiveness of neuromuscular training to reduce anterior cruciate ligament injury in female athletes. A Meta-Analysis. The American Journal of Sports Medicine 41, 203-215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paterno M.V., Myer G.D., Ford K.R., Hewett T.E. (2004) Neuromuscular training improves single-limb stability in young female athletes. Journal of Orthopaedic & Sports Physical Therapy 34, 305-316. [DOI] [PubMed] [Google Scholar]
- Robertson G., Caldwell G., Hamill J., Kamen G., Whittlesey S. (2013) Research Methods in Biomechanics. Human Kinetics; 2E. [Google Scholar]
- Schepers H.M. (2009) Ambulatory assessment of human body kinematics and kinetics, University of Twente. [Google Scholar]
- Schoenfeld B.J. (2010) Squatting kinematics and kinetics and their application to exercise performance. The Journal of Strength & Conditioning Research 24, 3497-506. [DOI] [PubMed] [Google Scholar]
- Shea CH., Wulf G. (1999) Enhancing motor learning through external-focus instructions and feedback. Human Movement Science 18 (4), 553-571. [Google Scholar]
- Stroube B.W., Myer G.D., Brent J.L., Ford K.R., Heidt R.S., Hewett T.E. (2013) Effects of task-specific augmented feedback on deficit modification during performance of the tuck-jump exercise. Journal of Sport Rehabilitation 22, 7-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sugimoto D., Myer G.D., Bush H.M., Klugman M.F., Mckeon J.M., Hewett T.E. (2012) Compliance with neuromuscular training and anterior cruciate ligament injury risk reduction in female athletes: a meta-analysis. Journal of Athletic Training 47, 714-723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sugimoto D., Myer G. D., Mckeon J.M., Hewett T.E. (2012) Evaluation of the effectiveness of neuromuscular training to reduce anterior cruciate ligament injury in female athletes: a critical review of relative risk reduction and numbers-needed-to-treat analyses. British Journal of Sports Medicine 46, 979-988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varoqui D., Froger J., Pelissier J.Y., Bardy B.G. (2011) Effect of coordination biofeedback on (re)learning preferred postural patterns in post-stroke patients. Motor Control 15, 187-205. [DOI] [PubMed] [Google Scholar]
- Wulf G. (2013) Attentional focus and motor learning: a review of 15 years. International Review of Sport and Exercise Psychology 6, 77-104. [Google Scholar]
- Wulf G., Dufek J.S., Lozano L., Pettigrew C. (2010) Increased jump height and reduced EMG activity with an external focus. Human Movement Science 9, 440-448. [DOI] [PubMed] [Google Scholar]
- Wulf G., McConnel N., Gartner M., Schwarz A. (2002) Enhancing the learning of sport skills through external- focus feedback. Journal of Motor Behavior 34, 171-182. [DOI] [PubMed] [Google Scholar]
- Wulf G., Mcnevin N. (2003) Simply distracting learners is not enough: More evidence for the learning benefits of an external focus of attention. European Journal of Sport Science 3, 1-13. [Google Scholar]
- Wulf G., McNevin N., Shea CH. (2001) The automaticity of complex motor skill learning as a function of attentional focus. The Quarterly Journal of Experimental Psychology: Section A 54, 1143-1154. [DOI] [PubMed] [Google Scholar]
- Wulf G., Prinz W. (2001) Directing attention to movement effects enhances learning: A review. Psychonomic Bulletin & Review 8, 648-660. [DOI] [PubMed] [Google Scholar]