

Abstract
This study examined respiratory muscle strength using the POWERbreathe® inspiratory muscle trainer (i.e., ‘S-Index’) before and after repeated-sprint cycling for comparison with maximal inspiratory pressure (MIP) values obtained during a Mueller maneuver. The S-Index was measured during six trials across two sessions using the POWERbreathe® and MIP was measured during three trials in a single session using a custom-made manometer in seven recreationally active adults. Global respiratory muscle strength was measured using both devices before and after the performance of sixteen, 6-s sprints on a cycle ergometer. Intraclass correlation coefficients for the POWERbreathe® S-index indicated excellent (p < 0.05) trial-to-trial (r = 0.87) and day-to-day (r = 0.90) reliability yet there was no significant correlation (r = -0.35, p = 0.43) between the S-Index measured using the POWERbreathe® and MIP measured during a Mueller maneuver. Repeated-sprint cycling had no effect on respiratory muscle strength as measured by the POWERbreathe® (p > 0.99) and during the Mueller maneuver (p > 0.99). The POWERbreathe® S-Index is a moderately reliable, but not equivalent, measure of MIP determined during a Mueller maneuver. Furthermore, repeated-sprint cycling does not induce globalized respiratory muscle fatigue in recreationally-active adults.
Key points.
The S-Index as measured by the POWERbreathe® is a reliable measure of respiratory muscle strength
The S-Index does not accurately reflect maximal inspiratory pressure obtained from a Mueller maneuver
Repeated-sprint cycling does not induce respiratory muscle fatigue as measured by the POWERbreathe® and the Manometer
Key words: Maximal inspiratory pressure, respiratory muscle fatigue, repeated-sprint ability, mouth pressure, manometer
Introduction
Inspiratory muscle fatigue can occur after prolonged (i.e., >2 h) submaximal running and after short-term maximal exercise (i.e., <15 min; approx. 95% peak oxygen uptake; Inbar et al., 2000; Johnson et al., 1993; Volianitis et al., 2001). It is however not known whether repeated-sprint exercise elicits respiratory muscle fatigue. The total duration of a repeated-sprint exercise protocol is typically between 10 and 15 min, (Mendez-Villaneuva et al., 2008; Spencer et al., 2005) and the average minute ventilation during repeated-sprinting (including the recovery periods) is >120 L·min-1, often peaking above 200 L·min-1 in elite male team-sport athletes, it is therefore reasonable to hypothesize that repeated-sprint exercise would result in inspiratory muscle fatigue.
Maximum inspiratory pressure (MIP) is an effective, non-invasive measure of global inspiratory muscle strength, particularly the strength of the diaphragm (Loke et al., 1982). The determination of MIP is simple, and is typically obtained by measuring mouth pressure during a maximal isometric inspiratory maneuver performed at residual lung volume (i.e., Mueller maneuver). MIP is then determined as the most negative 1-s average of mouth pressure generated during the maximal inspiratory effort (reported in units of centimeters of water; cmH2O). The Mueller maneuver is currently the gold standard for measuring MIP and several authors have demonstrated its validity and reliability (Hamnegard et al., 1994; McConnell and Copestake, 1999; Sachs et al., 2009).
With advancing technology there are now commercially available handheld devices such as the POWERbreathe® K5 inspiratory muscle trainer (POWERbreathe International Ltd, Warwickshire, UK) that provides an index of global inspiratory muscle strength (termed the ‘S-index’), enabling respiratory muscle performance to be monitored and evaluated in the field. Whereas MIP is typically obtained with a maximal static inspiratory effort, the POWERbreathe® S-index is measured during an unobstructed, dynamic maximal inspiratory maneuver. While the POWERbreathe® S-index cannot measure an individual’s true MIP, we hypothesize that the POWERbreathe® S-index can offer a reliable alternate measure of respiratory muscle fatigue to the gold-standard technique, the Mueller maneuver.
This study will provide coaches and sport scientists with preliminary information regarding the ability of the POWERbreathe® S-index to reliably provide information about the development of respiratory muscle fatigue during repeated-sprint exercise.
Methods
Experimental approach to the problem
Subjects attended the Griffith University Sport Science laboratory on three separate days (Session 1, 2, and 3). Session 1 involved preliminary health screening, explanation of the testing procedures, and familiarization will all testing equipment. The chief investigator described and demonstrated the correct techniques for the measurement of MIP during the Mueller maneuver, and the S-index using a POWERbreathe® inspiratory muscle trainer (Ironman K5, HaB Ltd, UK). Subjects were then instructed to sit on the cycle ergometer (Wattbike cycle ergometer, Wattbike Ltd, Nottingham, UK) and asked to practice the inspiratory maneuvers. Due to reliability of MIP measurements being highly dependent on subject effort and technique (Aldrich and Spiro, 1995), multiple breathing maneuvers were performed. Subjects were also familiarized with the Wattbike cycle ergometer and allowed to change both the handlebar and seat height before pedaling at the load to be applied during the repeated-sprint cycling protocol. During Session 2, six maximal inspiratory breathing maneuvers were performed; three trials using the POWERbreathe® and three trials of the Mueller maneuver. The order of the six trials was determined randomly using a coin flip until three breathing maneuvers had been performed on each device. At least 3 min of rest was allowed between trials. The repeated-sprint cycling protocol was performed during Session 3 and both devices were used only before and immediately after the repeated-sprint cycling protocol. The order of the devices both before and after the repeated-sprint exercise was determined by a coin flip. Heart rate (RS100, Polar, Oy Finland) and blood pressure was monitored throughout exercise during Session 3.
Subjects
Seven recreationally-active individuals (3 men, 4 women; age mean 22, sd = 1 yr, body mass mean 61.1, sd = 9.2 kg, stature mean 1.71, sd = 0.08 m) volunteered and provided written informed consent to participate in this study. All subjects were classified as “low risk” according to guidelines of the American College of Sports Medicine (2009, p. 20). The present study conformed to the principles outlined in the Declaration of Helsinki and was approved by the Griffith University Human Research Ethics Committee.
Procedures
Subjects performed a 10-min cycling warm up by pedaling at 60 rev·min-1 against a wind-only resistance setting of four. At minutes 6, 7 and 8 subjects were instructed to perform an ‘all-out’ sprint for 3 s against a wind-only resistance setting of 4. Following the warm up, subjects rested passively for 10 min. Subjects then returned to the cycle ergometer and performed four sets of, 4 x 6-s maximal sprint efforts on a 30-s cycle with sets separated by 2 min of passive rest. The wind-resistance setting was fixed at ten for both men and women whereas the magnetic setting was five for men and three for women. These settings were applied so to achieve the highest power output during sprinting and were predetermined in a pilot study in this laboratory. After the repeated-sprint exercise protocol was completed, subjects performed a 10-min warm down by cycling against a ‘wind-only’ resistance setting of four.
MIP was assessed on a custom-made Manometer by performing the Mueller maneuver immediately before and after the repeated-sprint protocol. The Mueller maneuver requires the subject to first exhale to residual lung volume, from which they are instructed to maximally, and then forcefully inhale against an obstructed mouthpiece for ~1.5–3.0 s (Green et al., 2002), while wearing a nose clip. Accordingly, the Mueller maneuver may be considered as a static contraction of the inspiratory muscles. Mouth pressure was sampled via a lateral port on the mouthpiece connected to a calibrated differential pressure transducer (PX138-005D5V, Omega Engineering Inc., Stamford, CT, USA). MIP was taken as the most negative 1-s average in mouth pressure during the maneuver.
The S-index was obtained using the POWERbreathe® K5 inspiratory muscle trainer during an unobstructed, maximal inspiratory effort from residual volume to total lung capacity. In this manner, the S-index was obtained during dynamic contraction of the inspiratory muscles. Subjects were coached by the investigators to achieve the highest inspiratory flow-rate possible during these tests. The PC software provided with the device (Breathe-Link, Version 1.0, 2012) was used to calculate the S-index, which is an indirect estimate of the subject’s “true” MIP (represented in cmH2O) obtained by using algorithms based on peak inspiratory flow, and a typical inspiratory muscle force-velocity profile. For comparison between the two devices, the maximum value of three maneuvers which varied by less than 20% was reported for each subject on each device (Green et al., 2002). All maneuvers were performed seated on the cycle ergometer in the exercise position.
Statistical analyses
Mean and standard deviation (s) values were calculated for the subjects’ physical characteristics, power output during cycling, as well as MIP and S-Index values. A fully factorial ANOVA with repeated-measures for trial and day was used to compare S-Index values across all six trials for the POWERbreathe® while a simple 1-way repeated measures ANOVA was used to determine differences in MIP values across three trials for the Mueller maneuver. When differences were detected, pairwise comparisons were performed to determine their source. Reliability was determined from intraclass correlation coefficients (ICC’s) calculated using S-Index values from all six trials of the POWERbreathe® and MIP values from all three trials of the Mueller maneuver. The coefficients for Trial 1 and Trial 2 were determined to investigate trial-to-trial reliability for both apparatus. Day-to-day reliability for the POWERbreathe® was determined by calculating the coefficients associated with the S-Index measured in Trial 3 during Session 1 and Trial 3 during Session 2 (i.e., Trial 6). The interpretation of the ICC’s was based on a scale described previously by Rosner (2005). Typical error and change in mean values were also used to characterize reliability. To examine the validity of the POWERbreathe®, a Pearson’s correlation coefficient was calculated using the highest values (cmH2O) recorded in Session 2 for both devices. Agreement between the two measurements was analyzed in a mean difference plot using all three trials for each subject (Bland and Altman, 1986). Statistical significance was set at P < 0.05 for all statistical tests.
Results
There were no differences in the S-Index among all six trials performed using the POWERbreathe® (F = 3.62, p = 0.06). Table 1 presents the ICC values, change in mean and typical error for S-Index using the POWERbreathe® calculated for Trial 1 and Trial 2 (trial-to-trial) as well as Trial 3 and Trial 6 (day-to-day) of testing. The ICC of all six trials was not notably different to the coefficient calculated for S-Index values determined during Trial 1 and Trial 2 only or compared to Trial 3 and Trial 6. There were no differences in MIP among all three Mueller maneuvers (F = 0.47, p = 0.63). The ICC’s for all three Mueller maneuvers was 0.95. The change in mean and typical error for MIP obtained during the Mueller maneuver calculated for Trial 1 and Trial 2 (trial-to-trial) was 1.60 and 8.32 cmH2O, respectively.
Table 1.
Determinants of reliability for maximal inspiratory strength (i.e., S-Index) measured with a POWERbreathe® inspiratory muscle trainer in seven recreationally-active individuals.
| ICC | Change in mean | Typical error | ||
|---|---|---|---|---|
| All 6 trials | .88 | |||
| Trial 1 & 2 | .87 | Mean (cmH2O) 90% CI’s Mean (%) 90% CI’s |
3.79 -3.93 – 11.52 5.2 -4.3 – 15.5 |
7.44 .36 – .99 9.5 6.5 – 18.9 |
| Trial 3 & 6 | .90 | Mean (cmH2O) 90% CI’s Mean (%) 90% CI’s |
4.36 -2.85 – 11.58 3.9 -3.0 – 11.1 |
6.95 4.80 – 13.31 6.7 4.6 – 13.3 |
Six maximal dynamic inspiratory breathing maneuvers (trials) were performed over two days; three trials each day. Trial-to-trial reliability (All 6 trials and Trial 1 & Trial 2) and day-to-day reliability (Session 1, Trial 3 and Session 2, Trial 3 i.e., Trial 6) was assessed. There were no differences in the mean values between Trial 1 & Trial 2 or between Trial 3 & Trial 6 (p > 0.05). ICC = intraclass correlation coefficient.
The peak power output determined for each set of 4 x 6-s sprints was significantly different (F = 10.80, p < 0.01) and is shown in Figure 1. The mean peak power of 715, s = 207 W determined for Set 1 was significantly higher than the mean peak power of 555, s = 174 W determined for Set 4 (p = 0.01). Also, Figure 1 illustrates no change in MIP (p = 0.57) or the S-Index (0.081) when measured before, compared to after the repeated-sprint protocol.
Figure 1.
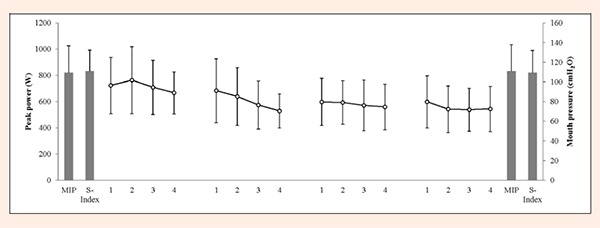
Peak power output measured during four sets of 4 x 6 s sprints on a 30-s cycle separated by 2 min of rest between sets in seven recreationally-active individuals. The columns represent maximal inspiratory pressure (MIP) measured during the Mueller maneuver and maximal inspiratory strength (S-Index) measured during dynamic inspiratory breathing maneuvers before and after repeated sprinting. There was no difference between the two measures of respiratory muscle strength, or before compared to after repeated sprinting (p < 0.05).
Figure 2a illustrates the relationship between peak MIP measured during a maximal isometric inspiration using the Manometer (i.e., Mueller maneuver) and the S-Index determined during a maximal dynamic inspiration using the POWERbreathe®. The Pearson’s correlation coefficient was -0.35 (p = 0.43) indicating that the two measurements were not closely related. Furthermore, agreement between the two measurements using all three trials for each subject is presented in Figure 2b. The increasing variance toward higher values implies that agreement between the two methods is poor.
Figure 2.
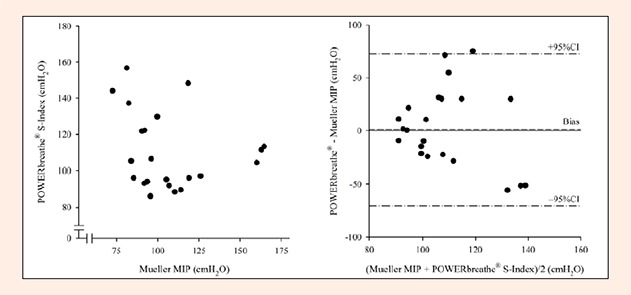
a. Left panel - The relationship between maximal inspiratory pressure (MIP) obtained during the Mueller maneuver and the S-Index determined using the POWERbreathe® (n = 21; 7 subjects x 3 trials); r = -0.35 (p = 0.43). b. Right panel - A mean difference plot17 depicting the level of agreement between inspiratory pressures measured during a Mueller maneuver and estimated from S-Index values measured on a POWERbreathe® device.
Discussion
The main findings of the present study demonstrate that the S-index provided by the POWERbreathe® is “acceptably” reliable (Cardinet et al., 2011). However, the POWERbreathe® S-index is not an equivalent measure of MIP when obtained during the gold-standard test, the Mueller maneuver. In addition to these findings, it is reported that repeated-sprint cycling does not induce globalized inspiratory muscle fatigue in recreationally-active men and women.
The measurement of MIP during the Mueller maneuver yielded an ICC of 0.95 indicating “almost perfect” reliability. These findings are consistent with the results of Dimitriadis et al. (2011) who reported excellent reliability of a handheld manometer (ICC > 0.90). The MIP values recorded during the Mueller maneuver for men and women in the present study (mean 109, sd = 27 cmH2O) were similar to the values previously reported in a meta-analysis by Sclauser et al. (2013) for men (approx. 116-140 cmH2O) and women (approx. 88-105 cmH2O).
The S-index measured using the POWERbreathe® inspiratory muscle trainer for seven recreationally-active individuals did not change across six trials, and there was no change in the ICC value when calculated for the first two trials (r = 0.87) compared with the value calculated for all six trials (r = 0.88). Furthermore, we established that the S-index could be measured reliably on separate days (r = 0.90). We conclude that the S-Index measured by the POWERbreathe® can be obtained from young, recreationally-active men and women with good trial-to-trial and day-to-day reliability.
The day-to-day reliability reported for the S-Index using the POWERbreathe® in the present study (6.7%) is similar to typical error values reported in previous studies that have investigated the reliability of power in physical performance tests (3.1 – 7.3%; Hopkins et al., 2001). An increase in MIP of ~24% has been reported for recreationally-active men and women (aged 22-40 yr) after 10 wk of respiratory muscle training (Aldrich and Spiro, 1995). The present study suggests that smaller changes in the S-Index measured before and after an intervention could be considered “worthwhile” (as defined by Hopkins, 2004) given the typical error value of 6.7% reported here for day-to-day reliability. For example, an increase in the S-Index of 3.35% (i.e., half the typical error), or about 3.5 cmH2O, measured after respiratory muscle training would allow coaches to be “reasonably confident of a worthwhile change” (Hopkins, 2004). Equally, coaches could assume that a 3.5 cmH2O decrease in the S-Index measured after intense exercise indicates respiratory muscle fatigue. Nevertheless, it should be noted that this error value was derived from a small group of subjects and therefore no firm conclusions can be drawn in relation to real changes in respiratory muscle strength using the POWERbreathe® respiratory muscle trainer.
Various methods are used to measure maximal respiratory mouth pressure and aside from the subjects themselves, values for MIP will inherently vary due to numerous variables including: the chosen device and technique, trial duration, definition of maximum pressure, type of mouth piece and pressure gauge, etc. (Evans and Whitelaw, 2009; Green et al., 2002). Nonetheless, maximal static respiratory pressures generated at the mouth after full expiration (i.e., Mueller maneuver) is the most widely used method of measuring MIP (McConnell and Copesake, 1999; Sclauser et al., 2013) and has been considered as a useful voluntary test of respiratory muscle strength (Green et al., 2002). There are no previous data indicating whether the S-Index determined by a POWERbreathe® during maximal dynamic inspiration is equivalent to the MIP obtained during a Mueller maneuver in humans. The correlation coefficient and the mean difference plot presented in Figure 2 shows that the S-index and MIP are not linearly related, nor do these measurements exhibit an appreciable level of absolute agreement (Altman and Bland, 1983).
Before concluding that the S-Index determined by the POWERbreathe® is invalid, one should consider the distinct difference between the muscle function qualities being tested during the Mueller maneuver compared to the dynamic contraction of the respiratory muscle using the POWERbreathe® (Baker et al., 1994). The POWERbreathe® demands a rapid and powerful dynamic contraction of the respiratory muscles (i.e., specific muscle function) whereas the inspiratory maneuver made during the Mueller maneuver is against a totally blocked airway and is therefore isometric (i.e., general muscle function). This distinction may help to explain both the absolute difference in the mean values, as well as the disagreement across the range of values measured. Furthermore, the small sample size in the present study should be considered as a limitation to the correlational analysis.
Previous studies have examined the relationship between isometric and dynamic muscle strength in skeletal muscle groups. Murphy and Wilson (1996) reported that isometric strength of the upper-limbs was a poor predictor of dynamic strength in the same muscle groups. They further illustrated that there are significant differences in the muscles’ neural activation patterns during isometric compared to dynamic contractions. Mechanisms that contribute to dynamic strength maybe unrelated to the mechanisms that contribute to isometric strength. Consequently, if respiratory muscle strength is contraction specific, this calls into question the efficacy of using the S-Index measured during a dynamic contraction to estimate MIP during a Mueller maneuver. Therefore, the two methods of respiratory muscle strength measurement in the present study are not comparable; that is, the S-Index measured using the POWERbreathe® cannot replace MIP measured during a Mueller maneuver with sufficient accuracy.
We found no change in the S-Index measured using the POWERbreathe® after compared to before repeated-sprint cycling. This result was confirmed by measuring MIP before and after sprinting during a Mueller maneuver. Although respiratory muscle fatigue has been observed after short-term continuous maximal exercise (Coast et al., 1990), it is reasonable to suggest that the intermittent nature of repeated sprinting provides sufficient time for the respiratory muscles to remove fatigue-inducing metabolites and recover oxygen debt. This notion is supported by McKenzie et al. (1991) who demonstrated that the diaphragm has a significantly increased ability to recover from fatigue when compared to other muscle groups. Although respiratory muscle fatigue was not demonstrated after repeated-sprint cycling in the present study, Romer et al. (2002) suggests that IMT might be warranted given the evidence that IMT improved recovery time and reduced blood lactate concentration during repeated-sprint running in team-sport athletes. Therefore, additional research is required to explore the efficacy of using IMT to improve RSA. It should also be noted that although reporting a “recreational” level of physical activity, peak aerobic power was not measured in the present study. Therefore, it is possible that some of the subjects were more than recreationally-active and this is why the sprint protocol was unsuccessful in inducing inspiratory-muscle fatigue.
The ability to measure global respiratory muscle strength reliably using a POWERbreathe® K5 device enables coaches and sport scientists to conveniently: i. Monitor changes in global respiratory muscle strength as a result of an exercise session or in response to training, ii. Establish a goal for a respiratory muscle training program, and iii. Establish normative values for global respiratory muscle strength specific to the POWERbreathe® device; all of which can be performed in the field. The change in mean and typical error values reported for the S-Index in the present study will allow coaches and Sport Scientists to identify physiologically meaningful changes in respiratory muscle strength. Furthermore, if the intended purpose of measurement is noted e.g., respiratory muscle strength during a dynamic inspiratory maneuver, the POWERbreathe® can provide a reliable measure of respiratory muscle strength. It is also suggested that when determining the maximal values of repeated efforts, the relative variability that should be accepted could be reduced from 20% (Green et al., 2002) to 10%.
Conclusion
In conclusion, the POWERbreathe® S-Index is a reliable measure of respiratory muscle strength in recreationally-active individuals. However, our results indicate that the S-Index does not accurately reflect MIP obtained from a Mueller maneuver. Finally, repeated-sprint cycling does not induce respiratory muscle fatigue as measured by the POWERbreathe® and the Manometer.
Biographies
Clare MINAHAN
Employment
Griffith University Sports Science, Gold Coast campus, Australia
Degree
PhD
Research interests
Sport science, acute responses and chronic adaptations to severe-intensity exercise, gender-related differences in the responses to exercise and training
Email: c.minahan@griffith.edu.au
Beth SHEEHAN
Employment
Griffith University Sports Science, Gold Coast campus, Australia
Degree
BSc (Hons), Masters candidate
Research interests
Sport science, disability and exercise, international health
Email: b.sheehan@griffith.edu.au
Rachel DOUTREBAND
Employment
Griffith University Sports Science, Gold Coast campus, Australia
Degree
BSc
Research interests
Allied health sciences
Email: r.doutreband@griffithuni.edu.au
Tom KIRKWOOD
Employment
Griffith University Sports Science, Gold Coast campus, Australia
Degree
BSc
Research interests
Allied health sciences
Email: t.kirkwood@griffithuni.edu.au
Daniel REEVES
Employment
Griffith University Sports Science, Gold Coast campus, Australia
Degree
BSc
Research interests
Allied health sciences
Email: d.reeves@griffithuni.edu.au
Troy CROSS
Employment
Division of Cardiovascular Diseases, Mayo Clinic, Rochester, MN, USA; Heart Foundation Research Centre, Gold Coast campus, Griffith University, Australia
Degree
PhD
Research interests
Applied respiratory mechanics; Locomotor and respiratory muscle blood flow in health and disease; Gas-exchange and respiratory dynamics during exercise
Email: t.cross@griffith.edu.au
References
- Aldrich T., Spiro P. (1995) Maximal inspiratory pressure: does reproducibility indicate full effort? Thorax 50, 40-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Altman D., Bland J. (1983) Measurement in Medicine: the Analysis of Method Comparison Studies. Statistician 32, 307-317. [Google Scholar]
- American College of Sports Medicine. (2009) ACSM’s Guidelines for Exercise Testing and Prescription. 7th edition. Philadelphia, PA: Lippincott Williams & Wilkins. [Google Scholar]
- Baker D., Wilson G., Carlyon B. (1994) Generality versus specificity: a comparison of dynamic and isometric measures of strength and speed-strength. European Journal of Applied Physiology and Occupational Physiology 68, 350-355. [DOI] [PubMed] [Google Scholar]
- Bland J.M., Altman D.G. (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 327, 307-310. [PubMed] [Google Scholar]
- Cardinet J., Johnson S., Pini G. (2011) Applying Generalizability Theory Using EduG. Taylor & Francis. [Google Scholar]
- Catham K., Baldwin J., Griffiths H., Summers L., Enright S. (1999) Inspiratory muscle training improves shuttle run performance in healthy subjects. Physiotherapy, 85, 676-683. [Google Scholar]
- Coast J., Clifford P., Henrich T., Stray-Gundersen J., Johnson R. (1990) Maximal inspiratory pressure following maximal exercise in trained and untrained subjects. Medical Sciences in Sports and Exercise 22, 811-815. [DOI] [PubMed] [Google Scholar]
- Dimitriadis Z., Kapreli E., Konsantinidou I., Oldham J., Strimpakos N. (2011) Test/retest reliability of maximum mouth pressure measurements with the MicroRPM in health volunteers. Respiratory Care 56, 776-82. [DOI] [PubMed] [Google Scholar]
- Evans J., Whitelaw W. (2009) The assessment of maximal respiratory mouth pressures in adults. Respiratory Care 54, 1348. [PubMed] [Google Scholar]
- Goosey-Tolfrey V., Foden E., Perret C., Degens H. (2010) Effects of inspiratory muscle training on respiratory function and repetitive sprint performance in wheelchair basketball players. Journal of Sports Medicine 44, 665-668. [DOI] [PubMed] [Google Scholar]
- Green M., Road J., Sieck G., Similowski T. (2002) Tests of Respiratory Muscle Strength. ATS/ERS Statement on respiratory muscle testing. American Journal of Respiratory and Critical Care Medicine 166, 518-624. [DOI] [PubMed] [Google Scholar]
- Hamnegard C-H., Wragg S., Kyroussis D., Aquilina R., Moxham J., Green M. (1994) Portable measurement of maximal mouth pressures. European Respiratory Journal 7, 398-401. [DOI] [PubMed] [Google Scholar]
- Hopkins W.G., Schabort E.J., Hawley J.A. (2001) Reliability of power in physical performance tests. Sports Medicine 31, 211-234. [DOI] [PubMed] [Google Scholar]
- Hopkins W.G. (2004) How to interpret changes in an athletic performance test. Sportscience 8, 1-7. [Google Scholar]
- Inbar O., Weiner P., Azgad Y., Rotstien A., Weinstein Y. (2000) Specific inspiratory muscle training in well-trained endurance athletes. Medicine and Science in Sports and Exercise 32, 1233-1237. [DOI] [PubMed] [Google Scholar]
- Johnson B., Babcock M., Suman O., Dempsey J. (1993) Exercise-Induced Diaphragmatic Fatigue in Healthy Humans. Journal of Physiology 460, 385-405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koutedakis Y., Sharp N. (1990) Fitness assessment of elite competitors. Rh eumatology Now 1, 18-20. [Google Scholar]
- Loke J., Mahler D., Virgulto J. (1982) Respiratory muscle fatigue after marathon running. Journal of Applied Physiology 52, 821. [DOI] [PubMed] [Google Scholar]
- McConnell A.K., Copestake A.J. (1999) Maximum static respiratory pressures in healthy elderly men and women: Issues of reproducibility and interpretation. Respiration 66, 251-258. [DOI] [PubMed] [Google Scholar]
- McKenzie D.K., Gandevia S.C. (1991) Recovery from fatigue of human diaphragm and limb muscles. Respiratory Physiology 84, 49-60. [DOI] [PubMed] [Google Scholar]
- Mendez-Villaneuva A., Hamer P., Bishop D. (2008) Fatigue in repeated-sprint exercise is related to muscle power factors and reduced neuromuscular activity. European Journal of Applied Physiology 103, 411-419. [DOI] [PubMed] [Google Scholar]
- Murphy A.J., Wilson G.J. (1996) Poor correlations between isometric tests and dynamic performance: relationship to muscle activation. European Journal of Applied Physiology and Occupational Physiology 73, 353-357. [DOI] [PubMed] [Google Scholar]
- Romer L.M., McConnell A.K., Jones D.A. (2002) Effects of inspiratory muscle training upon recovery time during high intensity, repetitive sprint activity. International Journal of Sports Medicine 23, 353-360. [DOI] [PubMed] [Google Scholar]
- Rosner B. (2005) Fundamentals of Biostatistics. Belmont, CA: Duxbury Press. [Google Scholar]
- Sachs M., Enright P., Hinckley K., Jiang R., Barr G. (2009) Performance of maximum inspiratory pressure test and maximum inspiratory pressure reference equations for 4 race/ethnic groups. Respiratory Care 54, 1321-1328. [PMC free article] [PubMed] [Google Scholar]
- Sclauser P. I., Franco P. V., Fregonezi G. A., Sheel A. W., Chung F., Reid W. D. (2013) Reference values for maximal inspiratory pressure: a systematic review. Canadian Respiratory Journal 21, 43-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spencer M., Bishop D., Dawson B., Goodman C. (2005) Physiological and metabolic responses of repeated-sprint activities specific to field-based team sports. Sports Medicine 35, 1025-1041. [DOI] [PubMed] [Google Scholar]
- Volianitis S., McConnell A., Koutedakis Y., Jones D. (2001) Specific respiratory warm-up improves rowing performance and exertional dyspnea. Medicine and Science in Sports Exercise 3, 1189-1193. [DOI] [PubMed] [Google Scholar]