

Abstract
Introduction
The determination of physiologic rest position of the mandible to the maxillae is of paramount importance in almost all fields of dentistry. The stability of vertical dimension at rest has been controversial if the rest position of mandible remains constant throughout life or not. Despite of several studies on the rest position of the mandible and facial vertical dimension, certain fundamental disagreements remain unresolved. The present study aims to compare the vertical dimension at rest, before and after extraction and after rehabilitation with complete denture.
Material & methods
This study was conducted in a total of ten randomly selected patients, who had some natural teeth present with one or more opposing posterior teeth with vertical occlusal stops but were advised for extraction because of poor prognosis. Digital lateral cephalograms were done and measurements recorded at three stages: prior to extraction of remaining natural teeth, post extraction and after complete denture rehabilitation.
Results
Vertical dimension at rest was found to be greatest in post rehabilitation followed by pre-extraction than post extraction state. The differences in changes were found to be statistically significant.
Conclusion
Vertical dimension at rest shows a decrease following extraction of natural teeth, the occlusal stops, and an increase on rehabilitation. It can be stated that vertical dimension at rest is not stable position and varies following extraction of natural teeth and rehabilitation.
Keywords: Complete denture, Cephalograms, Vertical dimension at rest
1. Introduction
The stability of vertical dimension at rest has been the most controversial aspect of prosthetic dentistry. It is debatable if the rest position of mandible remains constant throughout life or not. Rest is the postural position of the mandible when an individual is resting comfortably in an upright position and the associated muscles are in a state of minimal contractual activity.1–3 Several studies concluded that rest position remains constant throughout life irrespective of whether the patient is an infant, an adult or aged supported by several other investigators.4–7 However, during the same period several other studies8–10 demonstrated variability of rest position of mandible before and after extraction of natural teeth and after complete denture insertion.
The present study aims to determine cephalometrically, whether the vertical dimension at rest remains stable during the various phases, that is dentulous, edentulous and after rehabilitation with complete dentures.
2. Materials and methods
This study was conducted in the Department of Prosthodontics, Babu Banarsi Das College of Dental Sciences, Lucknow wherein a total of ten patients, who had some natural teeth present with one or more opposing posterior teeth with vertical occlusal stops but were advised for extraction because of poor prognosis (Fig. 1), were randomly selected after informed consent. The study was approved by the Institutional Ethical Committee. All subjects were medically fit and were at no surgical risk for extraction.
Fig. 1.

Few natural teeth with one or more opposing posterior teeth with vertical occlusal stops present, but advised for extraction because of poor prognosis.
The physiologic rest position of mandible was achieved by asking the patient to “swallow, say ‘m’ and relax”.11 The patients were well trained for maintaining their physiological rest position to minimize inaccuracies. Complete dentures were made conventionally and delineated for confirming the patient position at rest on radiographs by attaching stainless steel wire (22 gauge) at the level of plane of occlusion on buccal side of the maxillary and mandibular posterior teeth.
Digital lateral cephalograms of the subjects were taken on a digital cephalometric machine (Planmeca Proline XC, Finland) in standing position with relaxed lips and the subject's head in such a position that the Frankfort horizontal plane was parallel to the floor. The receptor – source distance was fixed at 60 inches. The exposure values were set at 68 kV, 5 mA, and exposure time of 23 s and the hard copies were printed. Cephalometric landmarks and planes (Figs. 5 and 6) were traced manually on tracing paper 0.003″ × 8″ × 10″ (Garware, India) using 0.5 mm HB pencil (Camel, India) on a view box using transilluminated light in a dark room. The length of VR-1 was measured with divider and metallic scale. This measurement was done at three stages of the study: Stage 1, before extraction of remaining natural teeth (Fig. 2). Stage 2, after extraction of remaining natural teeth. (Fig. 3) and stage 3, after complete denture rehabilitation (Fig. 4).
Fig. 5.
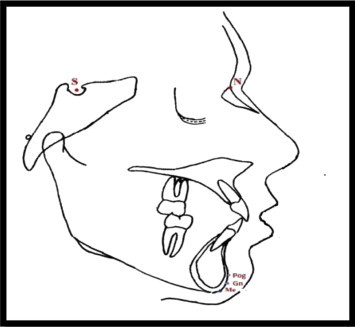
Cephalometric landmarks Nasion (N) – the most anterior point between the frontal and nasal bones on the frontonasal sutures, Sella (S) – the point representing the midpoint of pituitary fossa or sella turcica. It is a constructed point in the mid sagittal plane, Pogonion (Pog) – the most anterior point of the bony chin in the median plane, Menton (Me) – the most inferior midline point on the anterior surface of the mandible symphysis, and Gnathion (Gn) – the most antero-inferior point on the symphysis of the chin. It is marked by intersecting a line drawn perpendicular to the line connecting menton and pogonion.
Fig. 6.
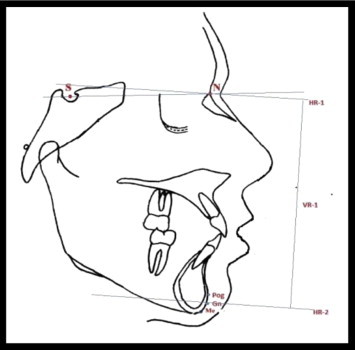
Cephalometric planes SN plane – it is the cranial base between the centre of sells tursica (S) and the anterior point of the frontonasal suture (N) and represents the anterior cranial base, HR-1 – this base line is a constructed horizontal plane, a surrogate Frankfort plane, constructed by drawing a line 7° to SN plane, to avoid vertical skeletal discrepancy in anterior, posterior or complex dysplasia of face.,11 HR-2 – A line passing through Gn, drawn parallel to HR-1, and VR-1 – A vertical line drawn from HR-1 to HR-2.
Fig. 2.

Stage 1, before extraction of remaining natural teeth.
Fig. 3.

Stage 2, after extraction of remaining natural teeth.
Fig. 4.

Stage 3, after complete denture rehabilitation.
Data was analysed statistically using SPSS (Statistical Package for Social Sciences) Version 15.0 statistical Analysis Software. Formulas used were mean, standard deviation, paired “t” test, level of significance.
3. Observations
Among the ten subjects included in the study, eight were male and two female, aged between 50 and 70 years.
Vertical dimension at rest was found to be greatest in post rehabilitation followed by pre-extraction than post extraction state. The differences in changes were found to be statistically significant (Table 1).
Table 1.
Comparison of VDR at three stages.
| No | Pre-extraction VDR |
Post extraction VDR |
Difference (A−B) |
Post rehabilitation VDR |
Difference (B−D) |
Difference (A−D) |
|---|---|---|---|---|---|---|
| (A) | (B) | (C) | (D) | (E) | (F) | |
| 1 | 9.3 | 9.0 | −0.3 | 9.6 | +0.6 | +0.3 |
| 2 | 12.5 | 12.0 | −0.5 | 12.7 | +0.7 | +0.2 |
| 3 | 9.4 | 9.2 | −0.2 | 9.6 | +0.4 | +0.2 |
| 4 | 9.1 | 8.6 | −0.5 | 9.4 | +0.8 | +0.3 |
| 5 | 11.1 | 11.00 | −0.1 | 11.4 | +0.4 | +0.3 |
| 6 | 11.4 | 11.2 | −0.2 | 11.6 | +0.4 | +0.2 |
| 7 | 11.6 | 11.4 | −0.2 | 12.0 | +0.6 | +0.4 |
| 8 | 10.5 | 10.2 | −0.3 | 10.3 | +0.1 | −0.2 |
| 9 | 10.4 | 10.1 | −0.3 | 10.3 | +0.2 | −0.1 |
| 10 | 10.7 | 10.5 | −0.2 | 10.9 | +0.4 | 0.2 |
| Mean | 10.60 | 10.32 | −0.28 | 10.78 | +0.46 | +0.18 |
| SD | 1.10 | 1.19 | 0.13 | 1.13 | 0.22 | 0.19 |
| Pre versus post extraction | “t” = 6.725; p < 0.001a |
| Pre versus post rehabilitation | “t” = 6.702; p < 0.001a |
| Post extraction versus post rehabilitation | “t” = 3.038; p = 0.014a |
Paired “t” test.
4. Discussion
Accurate recording of maxillomandibular relationships is an integral part of fabrication of complete dentures. It has been a long standing debate in the field of dentistry if the vertical dimension at rest changed or not, over the entire period of an individual's life. The removal of occlusal contacts is a major, sudden, pathologic insult to the entire stomatognathic system.7 The proprioceptive nerve endings in the periodontal membrane are destroyed which could be a principle influence on change in the rest position of the mandible. Thus, the loss of these nerve endings may hamper the orientation of the mandible8,11,12 thereby resulting in a decrease in vertical dimension at rest. This study showed a decrease in vertical dimension at rest in all the subjects following extraction of their occlusal stops. The change in vertical dimension at rest (range – 0.1–0.5 cm) was found to be statistically significant in all the subjects following extraction Graph 1.
Graph 1.
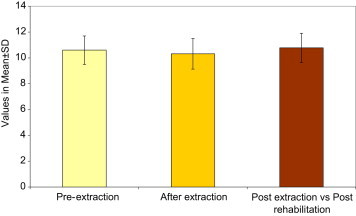
Vertical dimension at rest was found to be greatest in post rehabilitation followed by pre-extraction than edentulous state.
In this study, following insertion of complete dentures, there was an increase in vertical dimension at rest with the mean value of 10.78 cm, which was higher than the pre-extraction mean value of 10.6 cm. This can be explained on the basis that in edentulous patient there is a loss of perception of static jaw position and to recognize oral kinaesthetic perceptual abilities because of the lack of periodontal mechano-receptors.13–17 The presence of dentures provides artificial tooth contacts and pressure to the exteroceptors in the mucosa of the denture supporting area, mechano-receptors of temporomandibular joint and muscle (Golgi Tendon Organs and Muscle Spindles) which contribute to the regulating mechanism of mandibular posture.18 A change in the mandibular load and gravity also influences the rest position of the mandible.19
5. Conclusion
On basis of the observations, statistical analysis and discussion, it can be concluded that the vertical dimension at rest, shows a decrease following extraction of natural teeth (occlusal stops), while there is an increase in vertical dimension at rest on insertion of complete denture prosthesis.
Therefore, it can be stated that vertical dimension at rest is not stable position and varies following extraction of natural teeth and rehabilitation.
Conflicts of interest
All authors have none to declare.
References
- 1.Academy of Prosthodontics . 7th ed. Mosby; St Louis: 1994. The Glossary of Prosthodontic Terms. [Google Scholar]
- 2.Murphy W.M. Rest position of the mandible. J Prosthet Dent. 1961;17(4):329–332. doi: 10.1016/0022-3913(67)90003-0. [DOI] [PubMed] [Google Scholar]
- 3.Swerdlow H. Vertical dimension literature review. J Prosthet Dent. 1965;15(2):241–247. doi: 10.1016/0022-3913(65)90093-4. [DOI] [PubMed] [Google Scholar]
- 4.Duncan E.T., Williams S.T. Evaluation of rest position as a guide in prosthetic treatment. J Prosthet Dent. 1960;10(4):643–650. [Google Scholar]
- 5.Fayz F., Eslami A. Determination of occlusal vertical dimension: a literature review. J Prosthet Dent. 1998;59:321–323. doi: 10.1016/0022-3913(88)90182-5. [DOI] [PubMed] [Google Scholar]
- 6.Gillis R.R. Establishing vertical dimension full denture construction. JADA. 1934;28:430–436. [Google Scholar]
- 7.Sicher H. Positions and movements of the mandible. JADA. 1954;48:620–625. doi: 10.14219/jada.archive.1954.0100. [DOI] [PubMed] [Google Scholar]
- 8.Atwood D.A. The cephalometric study of the clinical rest position of the mandible part I. J Prosthet Dent. 1956;6(4):504–509. Part II. J Prosthet Dent 1957; 7; 544-52; Part III. J Prosthet Dent 1958; 8(4); 698-08. [Google Scholar]
- 9.Coccaro P., Lloyd R. Cephalometric analysis of morphologic face height. J Prosthet Dent. 1965;15:35–44. doi: 10.1016/0022-3913(65)90064-8. [DOI] [PubMed] [Google Scholar]
- 10.Tallgren A. Changes in adult face height due to aging, wear and loss of teeth and prosthetic treatment. Acta Odontol Scand Suppl. 1957;24(15):1–12. [Google Scholar]
- 11.Silverman M.M. Determination of vertical dimension by phonetics. J Prosthet Dent. 1956;6(4):465–471. [Google Scholar]
- 12.Ismail Y.H., George A., Sassouni V. Cephalometric study of the changes occurring in the face height following prosthetic treatment. J Prosthet Dent. 1968;19(4):321–330. doi: 10.1016/0022-3913(68)90033-4. [DOI] [PubMed] [Google Scholar]
- 13.Lambadakis J., Karkazis H.C. Changes in the mandibular rest position after removal of remaining teeth and insertion of complete dentures. J Prosthet Dent. 1992;68(1):74–77. doi: 10.1016/0022-3913(92)90289-m. [DOI] [PubMed] [Google Scholar]
- 14.Strajnic L., Sinobad D.S. Application of cephalometric analysis for determination of vertical dimension of occlusion–a literature review. Med Pregl. 2012;65(5–6):217–222. doi: 10.2298/mpns1206217s. [DOI] [PubMed] [Google Scholar]
- 15.Sakar O., Sulun T., Kurt H. Reliability and comparison of two facial measurements to detect changes of occlusal vertical dimension in complete denture wearers. Gerodontology. 2011;28(3):205–208. doi: 10.1111/j.1741-2358.2009.00353.x. [DOI] [PubMed] [Google Scholar]
- 16.Ochiai K.T., Hojo S., Nakamura C. Impact of facial form on the relationship between conventional or implant-assisted mandibular dentures and masticatory function. J Prosthet Dent. 2011;105(4):256–265. doi: 10.1016/S0022-3913(11)60041-3. [DOI] [PubMed] [Google Scholar]
- 17.Millet C., Leterme A., Jeannin C. Vertical dimension in the treatment of the edentulous patient. Rev Stomatol Chir Maxillofac. 2010;111(5–6):315–330. doi: 10.1016/j.stomax.2010.09.001. [DOI] [PubMed] [Google Scholar]
- 18.Shah F.K., Gebreel A., Elshokouki A.H. Comparison of immediate complete denture, tooth and implant-supported overdenture on vertical dimension and muscle activity. J Adv Prosthodont. 2012;4(2):61–71. doi: 10.4047/jap.2012.4.2.61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Klineberg I. Osseoperception: sensory function and propioreception. Adv Dent Res. 1999:120–129. doi: 10.1177/08959374990130010101. [DOI] [PubMed] [Google Scholar]