

Abstract
Introduction
To evaluate and compare the rate of intrusion and root resorption of maxillary incisors by three different intrusion techniques: Rickett's utility arch, Kalra's Simultaneous Intrusion & Retraction arch and arch with Reverse Curve of Spee.
Methods
The study was conducted over 30 patients aged between 14 and 25 yrs with deep bite requiring at least 2–4 mm intrusion of maxillary incisors. These patients were equally divided into three groups based on intrusion technique used, Rickets utility arch (Group I), K-SIR arch (Group II) and RCS arch (Group III). For each patient, amount of intrusion and root resorption occurring during intrusion was measured. Seven angular and six linear cephalometric measurements were made to evaluate skeletal and dental changes before and after incisor intrusion.
Results
The mean true incisor intrusion achieved with utility arch was 1.6 mm, with K-SIR, 1.25 mm and with RCS, 0.70 mm respectively. The rate of intrusion of utility arch was 0.44 mm/month, K-SIR – 0.33 mm/month, RCS – 0.35 mm/month, the difference was not statistically significant (p = 0.451). Utility arch had significantly higher mean root resorption of 1.56 mm as compared to K-SIR of 1.08 mm and RCS of 0.96 mm.
Conclusion
Both the intrusion rate and root resorption is more by utility arch while with K-SIR arch, though the rate of intrusion is almost same; the root resorption is much less.
Keywords: Biomechanics, Cepahlometrics, Deep bite, Root resorption
1. Introduction
Deep bite is a condition of excessive vertical overlapping of mandibular incisors by maxillary incisors when mandible is brought into habitual or centric occlusion. Deep bite usually leads to incisor wear, palatal impingement, gingival recession and compromised esthetics. This condition can be corrected by flaring of anterior teeth or uprighting of posteriors, intrusion of incisors, extrusion of posteriors or combination of both. Extrusion of posterior teeth for deep bite correction is more difficult to accomplish and also less stable in non growing patients than when it is attempted on patients with appreciable growth remaining.1 Furthermore, conditions like elongated incisors with gummy smile would be better treated by intruding the incisors.2
There are many intrusion methods such as Ricketts utility arch, K-SIR, RCS, J-headgear, implant, Connecticut intrusion arch, Burstone arch, three piece arch, vertical loops and many more. Since it is difficult to choose which method is better, an attempt is made through the present study to compare the rate of intrusion, root resorption and effect on maxillary central incisors achieved by three different methods: Ricketts utility arch, K-SIR arch and RCS arch, which are commonly used in our day to day clinical practice.
2. Materials and method
The study was conducted over 30 subjects aged between 14 and 25 yrs. A consent form was signed by each subject and approval was taken from the Human Research Ethical Committee. The inclusion criteria involved subjects requiring intrusion of 2.0–4.0 mm of maxillary incisors with no history of trauma to maxillary central incisors, complete incisor root formation, no previous orthodontic treatment, no growth remaining and showing average growth pattern. All subjects had initial leveling and aligning completed.
All subjects were randomly divided equally into three groups; Group I: Rickett's utility arch (0.017 × 0.025 TMA with cinch back and rectangular wire in premolar and molar region), Group II: K-SIR arch (0.017 × 0.025 TMA with cinch back and rectangular wire in premolar and molar region), Group III: RCS arch (0.016 × 0.022 NiTi with cinch back distal to molar).
Pre treatment lateral cephalograms in Natural Head Position3 (NHP) were taken after aligning the dental arches and just before starting any intrusion mechanics. Post treatment cephalograms in NHP were taken just after the intrusion of maxillary incisors, because if the cephalograms were obtained after complete orthodontic treatment, various other factors would have effected the maxillary incisors, especially during detailing. Additional torque is often added to the incisors; this would have obscured the real effect of the intrusion mechanics used. Seven angular and six linear cephalometric measurements were made to evaluate skeletal and dental changes before and after incisor intrusion (Figs. 1 and 2).
Fig. 1.
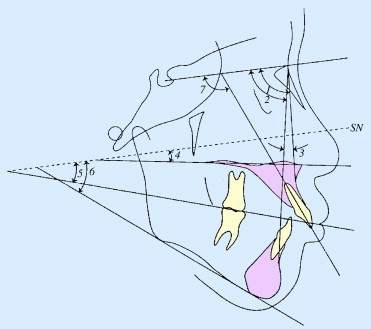
Cephalometric Linear measurements: 1, Anterior cranial base (S–N); 2, Horizontal distance between the maxillary and mandibular incisal edges (overjet); 3, Vertical distance between the maxillary and mandibular incisal edges (overbite); 4, Maxillary incisal edge to palatal plane (PP–U1); 5, Maxillary molar cusp to palatal plane (PP–U6); 6, Maxillary incisal edge to upper lip (UL-U1).
Fig. 2.
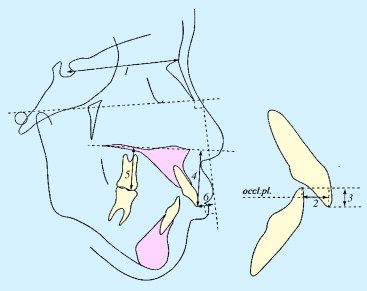
Cephalometric angular measurements: 1, Sella-Nasion-point A angle (SNA); 2, Sella-Nasion-point B angle (SNB); 3, Point A-Nasion-point B angle (ANB); 4, Sella-Nasion to palatal plane (PP-SN); 5 Sella-Nasion to occlusal plane (Occl-SN); 6, Sella-Nasion to mandibular plane (Mp-SN); 7, Upper incisor to Sella-Nasion (SN–U1).
2.1. Measurement of intrusion
For each patient, intrusion was measured as the length from the incisal edge of the upper incisor to the palatal plane of the maxilla.4 After the correction of the deep overbite, average duration of intrusion was 4.32 ± 0.7 months. The rate of intrusion of incisors per month was calculated by following formula.5
2.2. Measurement of root resorption
To measure the amount of root resorption, a precise, long-cone radiographic technique was used with the help of XCP film holder. There was neither distortion nor enlargement when the film was parallel to the tooth and the rays perpendicular to the film.6
Two radiographs were taken, one before the intrusion (but after alignment) and one after the intrusion. Thus, the observed resorption was limited to the resorption occurring during the active intrusion period. The central and lateral incisors of the same quadrant were registered on a single intraoral radiographic film to limit the patient's exposure to radiation.
The radiographs were examined on view box where the cement–enamel junctions at the mesial or distal aspects of the tooth in the pre and post treatment IOPA were marked and projected perpendicularly on the tooth axis.7 Total tooth length, crown length (defined as cementoenamel junction to incisal edge) and root length (defined as cementoenamel junction to apex of root) were measured with good illumination (Fig. 3).8 Although, it was believed that the precise distance between the incisal margin and tooth apex and the constructed cementoenamel junction could not be measured with sufficient accuracy, accurate measurement of absolute amounts of root resorption was not deemed possible.
Fig. 3.
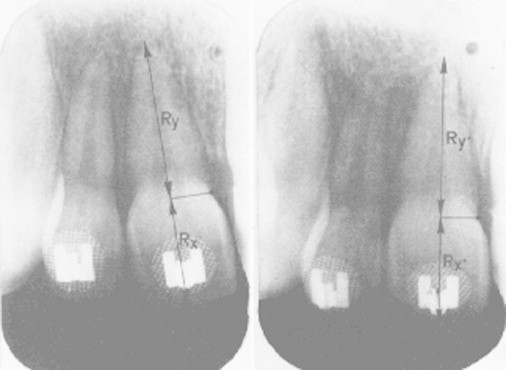
IOPA of maxillary incisors taken with long-cone technique.
Hence, the relation between the root length before (y) and after (y1) intrusion was calculated as follows6:
where, Rx: Distance from cementoenamel junction to incisal edge on x-ray films before intrusion Rx1: Distance from cementoenamel junction to incisal edge on x-ray films after intrusion, Ry: Root length on x-ray films before intrusion, Ry1: Root length on x-ray films after intrusion, x: Distance from cementoenamel junction to incisal edge before intrusion, x1: Distance from cementoenamel junction to incisal edge after intrusion.
Since.
2.3. Reliability of the method
The reliability of the intraoral, radiographic measuring method was tested in the control group. Assuming no measurable root resorption occurred (no therapy and a short investigation period), no change should be observed and measurements should be the same. Nevertheless, the relation y1/y was calculated for each of the control teeth with the procedure mentioned above. The mean was 0.99 (SD = 0.08). The t test showed no significant difference.
The observed values were subjected for statistical analysis using SPSS (Statistical Package for Social Sciences) version 15.0 statistical analysis software. The values were represented in number (%) and Mean ± SD.
3. Results
After treatment, statistically no significant difference among three groups under study was observed for any of the angular parameters except for ANB which was found to be significantly lower in Group I as compared to Groups II and III (Table 1).
Table 1.
Comparison change in angular and linear parameters among different groups.
| S.N. | Parameter | Group I (n = 10) |
Group II (n = 10) |
Group III (n = 10) |
Significance of difference (ANOVA) |
||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | F | P | ||
| Angular (in degrees) | |||||||||
| 1 | SNA | 0.30 | 1.57 | 0.00 | 1.63 | 0.00 | 0.67 | 0.162 | 0.852 |
| 2 | SNB | 0.60 | 0.97 | 0.10 | 1.10 | 0.00 | 0.67 | 1.197 | 0.318 |
| 3 | ANB | −0.10 | 1.29 | −0.10 | 0.74 | 0.00 | 0.00 | 0.045 | 0.956 |
| 4 | PP-SN | −0.30 | 2.11 | 0.40 | 2.63 | 0.40 | 0.84 | 0.405 | 0.671 |
| 5 | Occl-SN | −0.40 | 3.44 | 0.30 | 4.42 | 3.00 | 6.46 | 1.322 | 0.283 |
| 6 | Mp-SN | −0.50 | 2.22 | 0.40 | 1.43 | −0.60 | 0.84 | 1.182 | 0.322 |
| 7 | SN-U1 | 8.20 | 7.76 | 5.70 | 7.18 | 0.20 | 2.25 | 4.302 | 0.024 |
| Linear (in mm) | |||||||||
| 1. | S–N | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | – | – |
| 2. | Overjet | 1.80 | 0.92 | 1.60 | 0.70 | 0.80 | 1.03 | 3.500 | 0.045 |
| 3. | Overbite | 1.75 | 0.72 | 1.35 | 0.75 | 1.50 | 0.82 | 0.704 | 0.503 |
| 4. | PP-U1 | 1.60 | 0.52 | 1.25 | 0.98 | 0.70 | 0.63 | 3.800 | 0.035 |
| 5. | PP-U6 | 0.00 | 0.94 | 0.20 | 1.03 | −0.80 | 0.79 | 3.259 | 0.054 |
| 6. | UL-U1 | −1.50 | 1.96 | −0.20 | 1.48 | −0.40 | 1.07 | 2.051 | 0.148 |
n: number of patients, S.N.: Serial Number, SD: Standard Deviation, SNA: Angle formed by intersection of SN plane and a line joining nasion and point A, SNB: Angle formed by intersection of SN plane and a line joining nasion and point B, ANB: Angle formed by the intersection of lines joining nasion to point A and nasion to point B,PP-SN: angle between palatal plane and SN plane, Occl-SN: angle between Occlusal plane and SN plane, Mp-SN: Angle between Mandibular plane and SN plane,SN-U1: Angle formed by upper central incisor to SN plane, S–N: Distance from sella to nasion, PP-U1: Distance from palatal plane to upper central incisor, PP-U6: Distance from palatal plane to upper first molar, UL-U1: Distance from upper lip to upper central incisor.
All bold numbers are indicating significant results.
For linear parameters too, statistically no significant difference among three groups under study was observed for any parameter except overjet which was found to be significantly lower in Group II as compared to Groups I and III (p = 0.008) and UL-U1 which was significantly lower in Groups I and II as compared to Group III (p = 0.011) (Table 1).
No significant difference in mean change in angular variables among different groups was observed except for change in U1-SN which was found to be significantly lower in Group II as compared to Groups I and III (p = 0.024). However, with respect to change in linear parameters, a significant difference among groups was observed for overjet and U1-PP. It was observed that overjet correction and change in U1-PP in Group III was significantly lower as compared to that in Groups I and II (p < 0.05). For other parameters the differences among groups were not statistically significant (Table 1).
No significant difference among groups was observed with respect to rate of intrusion. Although, rate of root resorption showed statistically significant inter group differences (p = 0.006) (Table 2).
Table 2.
Comparison of rate of intrusion and root resorption among different groups.
| SN | Parameter | Group I (n = 10) |
Group II (n = 10) |
Group III (n = 10) |
Significance of difference (ANOVA) |
||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | F | P | ||
| 1 | Rate of intrusion (mm/month) | 0.44 | 0.18 | 0.33 | 0.19 | 0.35 | 0.21 | 0.821 | 0.451 |
| 2 | Root resorption (mm) | 1.56 | 0.36 | 1.08 | 0.41 | 0.96 | 0.43 | 6.320 | 0.006 |
SD: Standard Deviation, rate of root resorption showed statistically significant inter group differences (p = 0.006).
Table 3 showed that maximum difference for rate of intrusion was observed between Groups I and II and minimum between Groups II and III whereas for root resorption maximum difference was observed between Groups I and III and minimum difference was observed between Groups II and III. However, statistically significant differences between groups were observed only for root resorption for Groups I and II and for Group I and III. It was observed that Group I had significantly higher mean root resorption as compared to Groups II and III. The order of root resorption in different groups was as follows:
Table 3.
Inter Group Comparison of Rate of intrusion and root resorption (Tukey HSD test).
| SN | Comparison | Rate of intrusion |
Root resorption |
||||
|---|---|---|---|---|---|---|---|
| Mean diff. | SE | “P” | Mean diff. | SE | “P” | ||
| 1. | Group I vs II | 0.105 | 0.088 | 0.467 | 0.481 | 0.179 | 0.032 |
| 2. | Group I vs III | 0.088 | 0.088 | 0.583 | 0.603 | 0.179 | 0.006 |
| 3. | Group II vs III | −0.017 | 0.088 | 0.979 | 0.122 | 0.179 | 0.777 |
Statistically significant difference observed only for root resorption for Groups I and II and for Group I and III.
4. Discussion
In our study, the difference between the intrusion achieved by utility arch and K-SIR was not significant whereas the difference between these two and RCS was very much significant. Rate of intrusion of utility arch was 0.44 mm/month, K-SIR – 0.33 mm/month, RCS – 0.35 mm/month, the difference was not statistically significant (p = 0.451). Rate of intrusion by utility arch achieved in our study is similar to the results obtained by Neslihan Ebru Senisik9 and Esen Aydogdua10 while comparing the incisors intrusion using mini-implants and the utility arch which was 0.31 mm/month and 0.25 mm/month respectively. Frank J. Weiland (1996)8 concluded that for intrusion low forces of segmented arch technique is better than continuous arch technique.
It was observed that overjet correction and change in U1-PP in Group III was significantly lower as compared to that in Groups I and II (p < 0.05). It can be presumed that in group III (RCS) no overjet correction has been done and the leveling of the COS takes place more by premolar extrusion than incisor intrusion11 whereas with group I and II, retraction was simultaneously occurring due to tight cinch back.
It was observed that Group I (utility arch) had significantly higher mean root resorption of 1.56 mm as compared to Groups II (K-SIR) of 1.08 mm and group III (RCS) of 0.96 mm. It explains that more the movement of root towards apex, more will be the root resorption.12,13 It has also been reported that the greater the distance apex has to travel through the bone, the longer the time it is in close proximity to inflammatory process including osteoclastic activity,12,14 the result of this study reinforce this concept, as the group I has shown the maximum intrusion and maximum root resorption too. It can also be supported by studies done by Meha Verma (2010)12 and Goerigk B, Diedrich P and Wehrbein H (1992).15
However, Dermaut and Munck6 found no correlation between the amount of root resorption and the amount and duration of intrusion. They stated that in combination with the apical movement of the root, the nasal floor is also a limiting factor for intrusion and this may have caused root resorption. Similarly, McFadden et al7 stated that high resorptive potential root shortening in few patients can also be understood as intrusion achieved.
Studies by De Shields,16 Nelson and Artun17 and Harris18 have shown a correlation between change in axial inclination of incisors and root resorption which is also evident in our study, as group I (utility arch) showed maximum change in SN-U1 of 8.6° and also maximum of mean root resorption of 1.56 mm. The reason for this could be presumed as more the distance travelled by the root through the bone friction greater will be the root resorption.1 Whereas according to McFadden et al7 who studied various factors as age, sex, facial type, treatment time, extraction versus nonextraction therapy, width of the symphysis and the angle of the incisors to skeletal reference planes; for their relationship to intrusion and root shortening, using utility arches in the bioprogressive technique, found root shortening was 1.84 mm for maxillary incisors and 0.61 mm for mandibular incisors and change in angulation of the maxillary incisors with the use of utility arch during intrusion was not related to the amount of root shortening.
In the present study uprighting of incisors, with reduction in angle SN-U1 was seen, most with the utility arch followed by K-SIR and least with the RCS. Similarly Verma12 on comparing the effects of Burstone and Connecticut intrusion arches found uprighting of incisors while intrusion. We presume that the tight cinch back done prevented the flaring of incisors in our study.1 Although this was in contrast to other studies2,8,19 where significant intrusion was achieved with different intrusion methods like Connecticut utility implant, a flaring of upper incisors was always seen with utility arch and Connecticut intrusion arch.
We studied only patients with Class II Division1 malocclusion with specifically defined parameters. Our results cannot be arbitrarily extrapolated to the success that can be achieved with other categories of malocclusions such as those characterized by growth patterns. Since our sample size was limited and the results might not be the same with a larger sample size, further investigation is necessary to elucidate the relationship of force, rate of intrusion and root resorption. The findings of this study seem to emphasize that consideration should be given to treatment time when evaluating the possible occurrence of root shortening. When treatment is prolonged, a continued high degradative activity with osteoclasia causes severe root resorption.7 Therefore control of treatment time is of importance in most cases when intrusion of the maxillary incisors is performed.
5. Conclusion
We observed that there was a statistically significant difference in the mean true incisor intrusion achieved with utility arch 1.6 mm, K-SIR 1.25 mm and RCS 0.70 mm respectively (p = 0.035). The rate of intrusion was not statistically significant in the three groups (p = 0.451). Utility arch had significantly higher mean root resorption of 1.56 mm as compared to K-SIR 1.08 mm and RCS 0.96 mm.
We conclude that root resorption is directly related to the distance moved by the root towards the apex. Both the intrusion rate and root resorption is more by utility arch while with K-SIR arch though the rate of intrusion is almost same, the root resorption is much less.
Conflicts of interest
All authors have none to declare.
References
- 1.Bell W., Jacobs J., Legan H. Treatment of class II deep bite by orthodontic and surgical means. Am J Orthod. 1984;85:1–19. doi: 10.1016/0002-9416(84)90118-0. [DOI] [PubMed] [Google Scholar]
- 2.Krishna Nayak U.S., Goyal V., Godhrawal F. Comparison of skeletodental changes occurring during deep overbite correction with mini implant anchorage system and the utility arches reinforced by a transpalatal arch. J Indian Orthod Soc. 2011;45:9–14. [Google Scholar]
- 3.Sollow B., Tallgren A. Natural head position in standing subjects. Acta Odontol Scand. 1971;29:591–607. doi: 10.3109/00016357109026337. [DOI] [PubMed] [Google Scholar]
- 4.Deguchi T., Murakami T., Kuroda S. Comparison of the intrusion effects on the maxillary incisors between implant anchorage and J-hook headgear. Am J Orthod. 2008;133:654–660. doi: 10.1016/j.ajodo.2006.04.047. [DOI] [PubMed] [Google Scholar]
- 5.Mittal R., Patil A.K. Correction of deep overbite with mini-implants in adult patients. Orthod Cyber J. 2009;1:1–12. [Google Scholar]
- 6.Dermaut L.R., De Munck A. Apical root resorption of upper incisors caused by intrusive tooth movement: a radiographic study. Am J Orthod Dentofacial Orthop. 1986;90:321–326. doi: 10.1016/0889-5406(86)90088-0. [DOI] [PubMed] [Google Scholar]
- 7.McFadden Michael W., Engstrom C., Anholm J.M. A study of the relationship between incisor intrusion and root shortening. Am J Orthod Dentofacial Orthop. 1989;96:390–396. doi: 10.1016/0889-5406(89)90323-5. [DOI] [PubMed] [Google Scholar]
- 8.Weiland F.J., Bantleon H.P., Droschl H. Evaluation of continuous arch and segmented arch leveling techniques in adult patients a clinical study. Am J Orthod Dentofacial Orthop. 1996;110:647–652. doi: 10.1016/s0889-5406(96)80042-4. [DOI] [PubMed] [Google Scholar]
- 9.Ebru Senisik N., Turkkahraman H. Treatment effects of intrusion arches and mini-implant systems in deep bite patients. Am J Orthod Dentofacial Orthop. 2011;141:723–733. doi: 10.1016/j.ajodo.2011.12.024. [DOI] [PubMed] [Google Scholar]
- 10.Aydogdua E., Ozsoy O.P. Effects of mandibular incisor intrusion obtained using a conventional utility arch vs bone anchorage. Angle Orthod. 2011;81:767–775. doi: 10.2319/120610-703.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bernstein R.L., Preston C.B., Lampasso J. Leveling the curve of Spee with a continuous archwire technique: a long term cephalometric study. Am J Orthod Dentofacial Orthop. 2007;131:363–371. doi: 10.1016/j.ajodo.2005.05.056. [DOI] [PubMed] [Google Scholar]
- 12.Verma M. Comparative evaluation of intrusion and root resorption using Burstone and Connecticut intrusion arches – a vivo study. J Indian Orthod Soc. 2010;44:4–11. [Google Scholar]
- 13.Linge L., Ohm Linge B. Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment. Am J Orthod Dentofacial Orthop. 1991;99:35–43. doi: 10.1016/S0889-5406(05)81678-6. [DOI] [PubMed] [Google Scholar]
- 14.Burstone C.R. Deep overbite correction by intrusion. Am J Orthod Dentofacial Orthop. 1977;72:1–22. doi: 10.1016/0002-9416(77)90121-x. [DOI] [PubMed] [Google Scholar]
- 15.Goerigk B., Diedrich P., Wehrbein H. Intrusion of the anterior teeth with the segmented-arch technic of Burstone–a clinical study. Fortschr Kieferothop. 1992;53:16–25. doi: 10.1007/BF02165141. [DOI] [PubMed] [Google Scholar]
- 16.De Shields R.W. A study of root resorption in treated Class II, Division 1 malocclusions. Angle Orthod. 1969;39:231–245. doi: 10.1043/0003-3219(1969)039<0231:ASORRI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 17.Nelson P.A., Artun J. Alveolar bone loss of maxillary anterior teeth in adult orthodontic patients. Am J Orthod Dentofacial Orthop. 1997;111:328–334. doi: 10.1016/s0889-5406(97)70192-6. [DOI] [PubMed] [Google Scholar]
- 18.Harris E.F., Butler M.L. Pattern of incisor root resorption before and after orthodontic correction in cases with anterior open bites. Am J Orthod Dentofacial Orthop. 1992;101:112–119. doi: 10.1016/0889-5406(92)70002-R. [DOI] [PubMed] [Google Scholar]
- 19.Mihri A., Deniz S., Seyin H., Erol A., Seniz K. Intrusive effects of the connecticut intrusion arch and the utility intrusion arch. Turk J Med Sci. 2005;35:407–415. [Google Scholar]