

Abstract
Enterococci are one of the major agents of community-acquired and nosocomial infections. In this study we aimed to analyze the clonal relation of the vancomycin-resistant Enterococci outbreak seen at the Neonate Intensive Care Unit (NICU) of Uludag University Hospital. Vancomycin resistance gene was investigated in the Enterococcus faecium strains and pulsed field gel electrophoresis (PFGE) was used to investigate the genetic relation between outbreak strains. Enterococci grown in all patient samples were identified as Enterococcus faecium by BD Phoenix 100 (Becton Dickinson, USA). We found vanA resistance gene in all of the swab samples by Xpert VanA/B test on Cepheid (Cepheid, USA). PFGE band patterns revealed two different strains, of which the majority of them (22/24) had the same clonal origin. The common clonal origin was also isolated from rectal probes. Perianal swab culture positivity was evaluated as colonization but culture growth in two blood cultures, two urine cultures and one wound culture was evaluated as infection and treated with linezolid. All of the patients survived the outbreak. Besides the infection control precautions determining the genetic relation between outbreak strains which can be done in the microbiology laboratory is necessary to control an outbreak. PFGE is a reliable method in the microbiologic analysis of outbreaks. Molecular microbiologic analysis of outbreak strains will contribute to prove the epidemiologic and evolution of outbreaks.
Keywords: Enterococcus, neonatal, outbreak, PFGE
Introduction
Enterococci are one of the major agents of community-acquired and nosocomial infections. Antimicrobial resistance in Enterococci has posed challenges for treatment in recent years [1,2]. Vancomycin-resistant Enterococci (VRE) emerged in the 1970s and are a great problem in hospitals because of their ability to colonize and infect high risk patients [3]. Vancomycin-resistance is usually concomitant with penicilin and aminoglycoside resistance which restricts treatment options [2]. The capacity of enterococci to survive outside the human body for prolonged periods of time contributes to cross-contamination, through either the hands of healthcare workers, equipment, or surfaces, leading to nosocomial infections and outbreaks [4,5]. VRE is an epidemiologically important pathogen and contact precautions should be implemented in VRE colonized and infected patients [6]. Nosocomial infections are considered to be caused by direct contact with the hands of medical personnel [7].
In the management of outbreaks, rapid and reliable determination of genetic relation between outbreak strains is a very important tool to organize the infection control precautions [8]. Pulsed field gel electrophoresis is the gold standard method to investigate the genetic relation [5,8]. In this study we aimed to analyze the clonal relation of the VRE outbreak seen at the Neonate Intensive Care Unit (NICU) of Uludag University Hospital.
Materials and methods
Patients
Patients were newborn premature infants, who were being treated at the Neonate Intensive Care Unit (NICU) of Uludag University Hospital. Patient 4 and 6 had additonal diseases; patient 4 had a congenital heart disease and, patient 6 had bronchopulmonary dysplasia. Patient 1 was born in a different medical center and referred to our hospital on the 1st day of his life.
Culture samples and Enterococci strains
Routine VRE screening as an infection control policy has been established in our instutition for many years. During our routine screening, we investigated 15 perianal swab samples from the patients at the NICU; we also investigated two blood culture samples, two urine samples and a wound sample from 2 other patients and totally 17 patients were investigated for an outbreak at the NICU. We also investigated four swab samples from three rectal temperature probes. Bacterial identification and antibiotic susceptibility tests were done by BD Phoenix 100 (Becton from the patients at the NICU; we also investigated two blood culture samples, two urine samples and a wound sample from 2 other patients and totally 17 patients were investigated for an outbreak at the NICU. We also investigated four swab samples from three rectal temperature probes. Bacterial identification and antibiotic susceptibility tests were done by BD Phoenix 100 (Becton Dickinson, USA) system. Vancomycin resistance tests were repeated according to Clinical and Laboratory Standards Institute (CLSI) recommendations by Vancomycin E-test [9].
Vancomycin resistance gene detection by real-time PCR
Perianal swabs were analyzed for vancomycin resistance gene by Xpert VanA/B test on Cepheid (Cepheid, USA) according to the manufacturer’s instructions. Xpert VanA/B test detects Vancomycin resistance genes transmitted by transposons. These plasmids are usually found in E. faecium strains. Cepheid Xpert VanA/B is a qualitative in vitro diagnostic test for rapid detection of Vancomycin resistance genes (The primers and probes used was not given in test manual as it is a commercial secret).
Pulsed field gel electrophoresis (PFGE)
Colonies grown on solid media were transferred to cell suspension buffer including 10 mM Tris-HCl, 50 mM EDTA and 20 mM NaCl and then centrifuged at 13.000 g at 4°C for two minutes. Pellet was added into 2% low melt agarose and after adding 2 μl lysostaphine (10 mg/ml), it was incubated at 4°C until solidification. Cells in the agarose were lysed by cell lysis solution 1 including 10 mM Tris- HCl, 50 mM NaCl, 50 mM EDTA-0.2% sodyum deoxicholate-0.5% sarkosyl. After lysis agarose was incubated on ice for solidification. Cells in the agarose were lysed by cell lysis solution 2 including 30 μl proteinase K (50 mg/ml) and 5970 μl ES solution (250 mM EDTA, 1% sarkosyl). Agarose molds were washed three times at 50°C for 30 minutes by Tris-HCl- EDTA buffer (10 mM Tris-HCl, 0.1 mM EDTA). Plug molds were divided into two by lancet of which, one was used for PFGE and the other was kept as a spare. Plug molds were incubated at 30°C by SmaI in water bath. Plug molds were loaded on electrophoresis gel. All gels were electrophoresed in 0.5x TBE buffer at 6 V/cm for 20 hours 14°C with a pulse duration of 5.3 to 34.9 seconds ramped linearly in CHEF-DR II system (Bio-Rad Laboratories, Belgium). Gels were stained with etidium bromide, destained in distilled water and photographed with Biometra Gel Documentation Module (Biometra GmBH, Germany). Band profiles were inspected by Bio Doc Analyze Software (Biometra GmBH, Germany). These data were used to produce dendograms showing unwighted pair group method with mathematical averaging (UPGMA) cluster analysis of Dice similarity coefficients produced from pair-wise comparisons of the coded profiles which was taken as 1%. Results were interpreted accoding to Tenover criteria [10].
Results
Enterococci grown in all patient samples were identified as Enterococcus faecium by BD Phoenix 100 (Becton Dickinson, USA). All of the strains were resistant to vancomycin, teicoplanin, penicilin, ampicillin and susceptible to daptomycin, linezolid and quinopristin-dalfopristin. We found vanA resistance gene in all of the swab samples by Xpert VanA/B test on Cepheid (Cepheid, USA) (Figure 1). PFGE band patterns are shown in Figure 2 and dendograms are shown in Figure 3. Dendogram profiles revealed two different strains, of which the majority of them (22/24) had the same clonal origin. The other two strains had the same clonal origin which were isolated from perianal swabs of two different patients. The common clonal origin was also isolated from rectal probes. The results are summarized in Table 1. Perianal swab culture positivity was evaluated as colonization but culture growth in two blood cultures, two urine cultures and one wound culture was evaluated as infection. These findings revealed the presence of an outbreak which began on Semptember 2013 and ended on December 2013. Infected patients were treated with linezolid. All of the patients survived the outbreak. The first outbreak patient was referred to our hospital from a different healthcare center.
Figure 1.
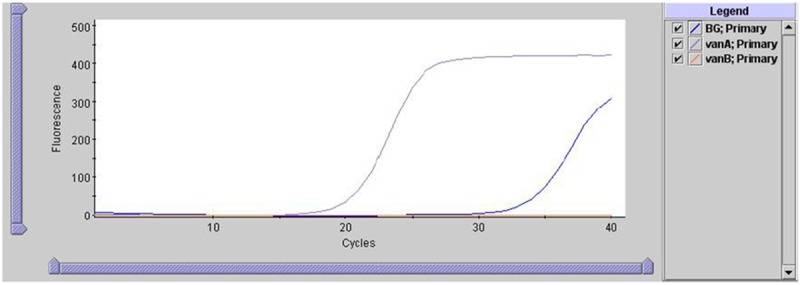
Determination of vanA resistance gene in all of the swab samples by Xpert VanA/B test on Cepheid (Cepheid, USA).
Figure 2.
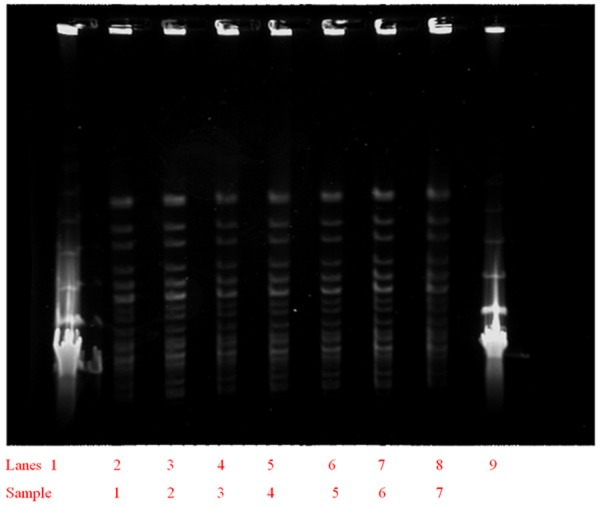
Strain relation according to PFGE (Lane 1and 9: Molecular marker) (PCR 20 bp Low Ladder, Sigma-Aldrich, USA).
Figure 3.
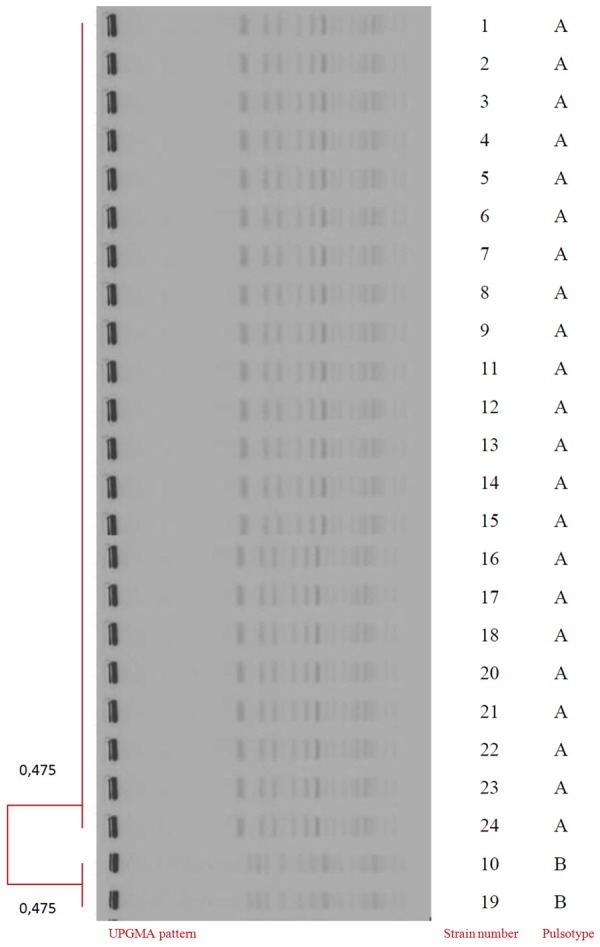
UPGMA patterns of strains; strain numbers and pulsotypes.
Table 1.
Specimen type, number and pulsotype according to patients
| Patient/Probe No | Sample No | Specimen | Pulsotype |
|---|---|---|---|
| 1 | 1 | PAS | A |
| 2 | 2 | PAS | A |
| 3 | 3 | PAS | A |
| 4 | 4 | PAS | A |
| 4 | 5 | Blood culture | A |
| 5 | 6 | PAS | A |
| 6 | 7 | PAS | A |
| 7 | 8 | PAS | A |
| 7 | 9 | Blood culture | A |
| 8 | 10 | PAS | B |
| 9 | 11 | PAS | A |
| 10 | 12 | PAS | A |
| 10 | 13 | Urine | A |
| 11 | 14 | PAS | A |
| 12 | 15 | Urine | A |
| 13 | 16 | PAS | A |
| 14 | 17 | Wound | A |
| 15 | 18 | PAS | A |
| 16 | 19 | PAS | B |
| 17 | 20 | PAS | A |
| Probe 1 | 21 | Swab | A |
| Probe 2 | 22 | Swab | A |
| Probe 2 | 23 | Swab | A |
| Probe 3 | 24 | Swab | A |
PAS, Perianal swab; A: Pulsotype of common isolate, B: Pulsotype of other isolates.
Discussion
This study revealed a close relationship between VRE colonization and VRE symptomatic infections; similar pulsotypes were identified in patients both asymptomatic and clinically manifested VRE. Five patients were infected after colonization. These findings reveal that infection control policies should include active surveillence which should monitor both VRE colonization and VRE infection [11,12].
Typing of bacterial strains is important in the suspicion of an outbreak and proving the nosocomial spread of infections. Phenotypic and genotypic methods can be used for strain typing, but now molecular methods are being used generally [10,13,14]. PFGE, rep-PCR and RFLP methods are the common methods for molecular typing. PFGE is more discriminative than rep-PCR in defining clonal relation. Though PFGE turnaround time is longer than rep-PCR, PFGE costs less than rep-PCR [15]. In this study we used PFGE to fingerprint DNA of VRE. DNA was digested by SmaI restriction enzyme and divided into 10 to 20 pieces differing from 10 to 800 kilobase pairs which was electrophoresed by iso-electric focusing [13,14,16].
Infection control precautions could not be implemented until the time passed during isolation, identification and reporting of the first strain, which resulted in spread of VRE to other neonates and led to an outbreak. As the first strain was imported from a diffent center, strict infection control precautins could be implemented for a time, as there was not a VRE colonization in our NICU. The probes which were shown to be colonized with the same VRE strain played an important role in the outbreak besides the hands of the health care staff. Though all the strains were phenotypically showed concordant, PFGE revealed genetical discrepancy between the strains. It was thought that, phenotypical methods are not able to determine genetical discrepancies. That’s why many laboratories are increasingly using molecular techniques, as they offer higher sensitivity and faster turnaround time than traditional culture methods [17,18].
Multiple approaches were used to curtail the outbreak. As per usual all VRE infected or colonized patients were subjected to control precautions, enhanced infection control and prevention measures were undertaken including the use of personel protective equipment, strategies to increase adherence to hand hygiene recommendations, no more new patient was imported to the neonatal unit and none of the patients were exported from neonatal unit to other clinics during outbreak, education about infection control precautions was given to all workers and rectal probes were treated by disinfectants for a longer duration and higher concentration [17,19,20]. After the treatment of the last outbreak patient and no more VRE growth in culture plates, it was thought that the outbreak was terminated.
Implementation of molecular methods have an important role in the management and analysis of outbreaks. PFGE, which may be used in outbreaks has a high correlation with epidemiological data and can be used as the gold standard molecular method. PFGE usage is restricted because of the facts that; PFGE is labor intensive, needs authorized personnel and it needs an expensive device.
During an outbreak, determining the genetic relation between outbreak strains which can be done in the microbiology laboratory as an infection control precaution is necessary. Molecular microbiologic analysis of outbreak strains may prove the epidemiologic and evolution of outbreak strains.
Disclosure of conflict of interest
None.
References
- 1.Cetinkaya Y, Falk P, Mayhall CG. Vancomycin-resistant Enterococci . Clin Microbiol Rev. 2000;13:686–707. doi: 10.1128/cmr.13.4.686-707.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Deshpande VR, Karmarkar MG, Mehta PR. Prevalance of multi-drug resistant Enterococci in a tertiary care hospital in Mumbai, India. J Infect Dev Ctries. 2013;7:155–158. doi: 10.3855/jidc.3018. [DOI] [PubMed] [Google Scholar]
- 3.Gilmore MS, Lebreton F, van Schaik W. Genomic transition of Enterococci from gut commensals to leading causes of multidrug-resistant hospital infection in the antibiotic era. Curr Opin Microbiol. 2013;16:10–16. doi: 10.1016/j.mib.2013.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sood S, Malhotra M, Das BK, Kapil A. Enterococcal infections & antimicrobial resistance. Indian J Med Res. 2008;128:111–121. [PubMed] [Google Scholar]
- 5.Resende M, Caierao J, Prates JG, Narvaez GA, Dias CAG, d’Azevedo PA. Emergence of vanA vancomycin-resistant Enterococcus faecium in a hospital in Posto Alegre, South Brazil. J Infect Dev Ctries. 2014;8:160–167. doi: 10.3855/jidc.4126. [DOI] [PubMed] [Google Scholar]
- 6.Kaki R, Yu Y, O’Neill C, Lee C, Mertz D. Vancomycin-resistant Enterococcus (VRE) transmission and risk factors in contacts of VRE carriers. Infect Control Hosp Eoidemiol. 2014;35:876–879. doi: 10.1086/676864. [DOI] [PubMed] [Google Scholar]
- 7.Takei Y, Yokoyama K, Katano H, Tsukiji M, Ezaki T. Molecular epidemiological analysis of methicillin-resistant Staphylococci in a neonatal intensive care unit. Biocontrol Sci. 2010;15:129–138. doi: 10.4265/bio.15.129. [DOI] [PubMed] [Google Scholar]
- 8.Grisold AJ, Zarfel G, Strenger V, Feierl G, Leitner E, Masoud L, Hoenigl M, Raggam RB, Dosch V, Marth M. Use of automated repetitive-sequence-based PCR for rapid laboratory confirmation of nosocomial outbreaks. J Infect. 2010;60:44–51. doi: 10.1016/j.jinf.2009.10.045. [DOI] [PubMed] [Google Scholar]
- 9.Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Testing, 22nd Informational Supplement, M100-S22. Wayne, Pennsylvania, U S A: 2012. [Google Scholar]
- 10.Tenover FC, Arbeit RD, Goering RV, Mickelsen PA, Murray BE, Persing DH, Swaminathan B. Interpreting chromosomal DNA restriction patterns produced by pulsed field gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol. 1995;33:2233–2239. doi: 10.1128/jcm.33.9.2233-2239.1995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Morris JG Jr, Shay DK, Hebden JN, McCarter RJ Jr, Perdue BE, Jarwis W. Enterococci resistant to multiple antimicrobial agents, including vancomycin: establishment of endemicity in a University Medical Center. Ann Intern Med. 1995;123:250–259. doi: 10.7326/0003-4819-123-4-199508150-00002. [DOI] [PubMed] [Google Scholar]
- 12.Lee SC, Wu MS, Shih HJ, Huang SH, Chiou MJ, See LC, Siu LK. Identification of vancomycin-resistant Enterococci clones and inter-hospital spread during an outbreak in Taiwan. BMC Infect Dis. 2013;13:163. doi: 10.1186/1471-2334-13-163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cantor CR, Smith CL, Mathew M. Pulsed-field gel electrophoresis of very large DNA molecules. Ann Rev Biophys Chem. 1988;17:287–304. doi: 10.1146/annurev.bb.17.060188.001443. [DOI] [PubMed] [Google Scholar]
- 14.Ostojic M. Epidemiologic genotyping of methicillin-resistant Staphylococcus aureus (MRSA) by pulsed field gel electrophoresis (PFGE) Bosn J Basic Med Sci. 2008;8:259–265. doi: 10.17305/bjbms.2008.2930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chuang YC, Wang JT, Chen ML, Chen YC. Comparison of an automated repetitive sequence based PCR microbial typing system with pulsed-field gel electrophoresis for molecular typing of vancomycin-resistant Enterococcus faecium . J Clin Microbiol. 2010;48:2897–2901. doi: 10.1128/JCM.00136-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Grisold AJ, Zarfel G, Strenger V, Feierl G, Leitner E, Masoud L, Hoenigl M, Raggam RB, Dosch V, Marth E. Use of automated repetitive-sequence-based PCR for rapid laboratory confirmation of nosocomial outbreaks. J Infect. 2010;60:44–51. doi: 10.1016/j.jinf.2009.10.045. [DOI] [PubMed] [Google Scholar]
- 17.Szakacs TA, Kalan L, McConnel MJ, Eshaghi A, Shahinas D, McGeer A, Wright GD, Low DE, Patel SN. Outbreak of Vancomycin-susceptible Enterococcus faecium containig the wild type VanA gene. J Clin Microbiol. 2014;52:1682–1686. doi: 10.1128/JCM.03563-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kee SE, Park CW, Lee JE, Kwon YJ, Pyo HJ, Kim WJ, Cheong HJ. Healthcare-associated risk factors ov vancomycin-resistant Enterococci colonization among outpatients undergoing hemodialysis. Jpn J Infect Dis. 2012;65:57–60. [PubMed] [Google Scholar]
- 19.Escaut L, Bouam S, Frank-Soltysiak M, Rudant E, Saliba F, Kassis N, Presiozi P, Vittecoq D. Eradication of an outbreak of vancomycin-resistant Enterococcus (VRE): the cost of a failure in the systematic screening. Antimicrob Resist Infect Control. 2013;2:18. doi: 10.1186/2047-2994-2-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Iosifidis E, Evdoridou I, Agakidou E, Chochliouruou E, Protonotariou E, Karakoula K, Stathis I, Sofianou D, Drossou-Agakidou V, Pournaras S, Roilides E. Vancomycin-resistant Enterococcus outbreak in a neonatal intensive care unit: epidemiology, molecular analysis and risk factors. Am J Infect Control. 2013;41:857–61. doi: 10.1016/j.ajic.2013.02.005. [DOI] [PubMed] [Google Scholar]