

Abstract
Balanced acupuncture, a single-acupoint balance therapy, regulates the balance of the cerebral center, and is characterized by exerting quick effects and a short treatment course. A total of 20 low-back and leg pain patients with lumbar disc herniation were treated with balanced acupuncture or body acupuncture. Central mechanisms of varied acupunctures were compared using resting-state functional MRI. Patients from both groups received functional MRI before and after acupuncture. Functional connectivity in brain regions that were strongly associated with the bilateral amygdala was analyzed utilizing AFNI software. Visual analogue scale scores were greater in the balanced acupuncture group compared with the body acupuncture group. Function of the endogenous pain regulation network was enhanced in patients in the balanced acupuncture group, but was not changed in the body acupuncture group. This result indicates that the analgesic effects of body acupuncture do not work through the central nervous system. These data suggest that balanced acupuncture exerts analgesic effects on low-back and leg pain patients with lumbar disc herniation by regulating the function of the endogenous pain regulation network.
Keywords: balanced acupuncture, body acupuncture, lumbar disc herniation, functional connectivity, amygdala, low-back and leg pain, pain, acupuncture, traditional Chinese medicine, neural regeneration
Research highlights
(1) Balanced acupuncture exerts analgesic effects in low-back and leg pain patients with lumbar disc herniation by regulating the function of the endogenous pain regulation network. The results of balanced acupuncture were better than those of body acupuncture. (2) The function of the endogenous pain regulation network was significantly enhanced in patients from the balanced acupuncture group. No overall changes in the function of the endogenous pain regulation network were detectable in the body acupuncture group. (3) The analgesic effects of body acupuncture do not work through the central nervous system. Thus, balanced acupuncture exerts effects rapidly, and the effects can last for a long period. However, the effects of body acupuncture occur more slowly.
Abbreviations
VAS, visual analogue scale
INTRODUCTION
Acupuncture analgesia is a common method for treatment of lumbar disc herniation. Balanced acupuncture and body acupuncture are frequently used in the clinic. Previous studies showed that body acupuncture at the Weizhong (BL40), Dachangshu (BL25), Ashi acupoint and Guanyuanshu (BL26) (The Urinary Bladder Channel of Foot-Taiyang) has a good analgesic effect by improving blood circulation and eliminating inflammatory edema[1,2]. Balanced acupuncture is a technique combining traditional medicine and modern medicine and a single-acupoint balance therapy, which can regulate the cerebral center, resulting in self-repair, self-integrity, and self-healing[3,4,5]. Balanced acupuncture is characterized by exerting quick effects and a short treatment course[5]. However, the present acupuncture scheme was selected mainly according to the physician's experience and lacked scientific criteria.
This study investigated the effects of balanced acupuncture versus body acupuncture on the endogenous pain regulation network in the brain of low-back and leg pain patients with lumbar disc herniation using resting-state functional MRI.
RESULTS
Quantitative analysis of subjects
A total of 20 low-back and leg pain patients with lumbar disc herniation were equally and randomly assigned to balanced acupuncture or body acupuncture groups. Patients from the balanced acupuncture and body acupuncture groups underwent balanced acupuncture and body acupuncture, respectively. They received resting-state functional MRI before and after acupuncture. A total of 20 patients were included in the final analysis, with no drop outs.
Baseline data of subjects and pain evaluation results
Baseline data of patients from the balanced acupuncture group are exhibited in Table 1.
Table 1.
Baseline data and visual analogue scale scores in patients from the balanced acupuncture group
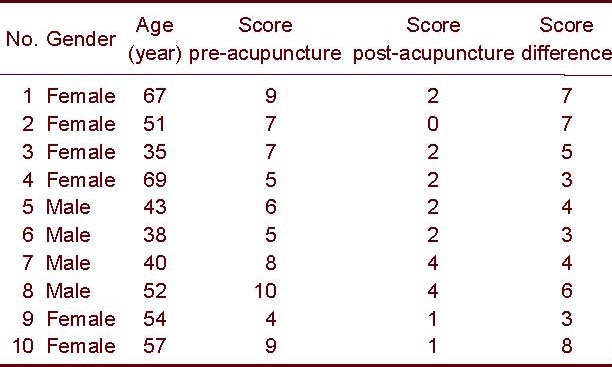
The mean visual analogue scale (VAS) score was 4.5 ± 1.65 at 10 minutes following balanced acupuncture. The VAS score was 0 in one patient, representing healing. VAS scores were less than 10 in nine patients, representing improvement.
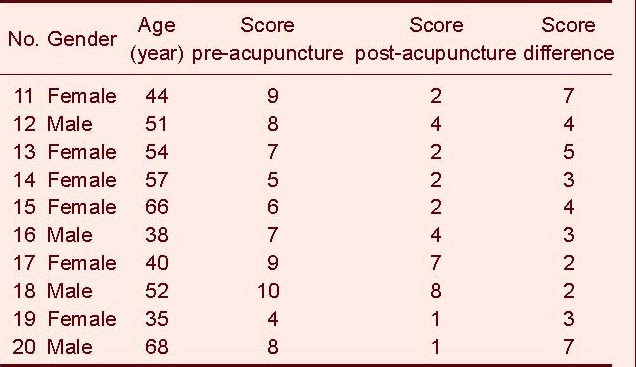
The mean VAS score was 4.0 ± 1.8 at 10 minutes following body acupuncture. VAS scores were less than 10 in 10 patients, representing improvement.
A one-sample t-test demonstrated that the mean VAS score was greater in the balanced acupuncture group than that in the body acupuncture group (P < 0.05).
Brain functional connectivity in low-back and leg pain patients with lumbar disc herniation following balanced acupuncture (Figure 1, Table 3)
Figure 1.
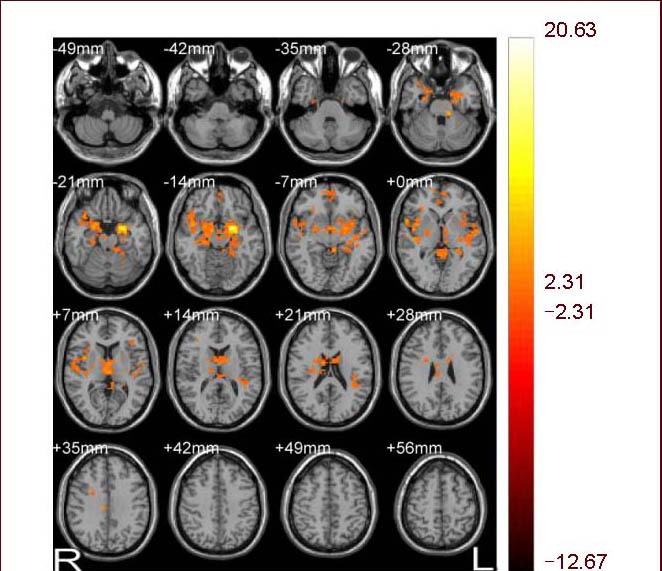
Image of brain functional connectivity in low-back and leg pain patients with lumbar disc herniation following balanced acupuncture. Bilateral amygdala served as a seed point. R: Right; L: left.
Table 3.
Changes in brain functional connectivity before and after balanced acupuncture using the amygdala as a seed point (Four temporal clusters)
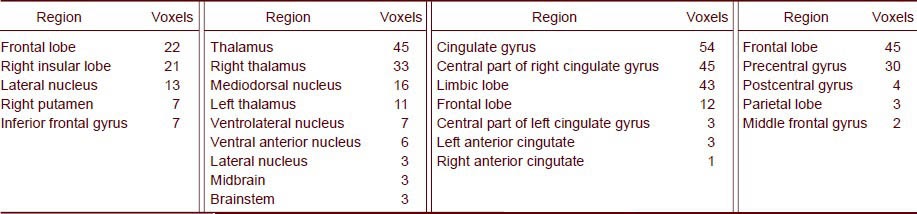
Table 2.
Baseline data and visual analogue scale scores in patients from the body acupuncture group
After balanced acupuncture, brain regions that were strongly associated with the bilateral amygdala (time correlation) in a resting state included the putamen, thalamus, superior temporal gyrus, insular lobe, brain stem, middle temporal gyrus, orbit of superior frontal gyrus, inferior frontal gyrus, cingulated gyrus, ventral anterior nucleus, ventrolateral nucleus, medial frontal gyrus and superior frontal gyrus (t = 4.97, P < 0.05; Figure 1, Table 3).
Brain functional connectivity in low-back and leg pain patients with lumbar disc herniation following body acupuncture
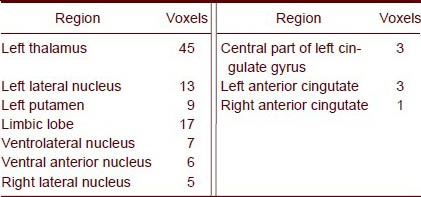
After body acupuncture, brain regions strongly associated with the bilateral amygdala (time correlation) in a resting state included the left thalamus, left putamen, ventrolateral nucleus, limbic lobe and cingulated gyrus (t = 4.81, P < 0.05; Figure 2, Table 4).
Figure 2.
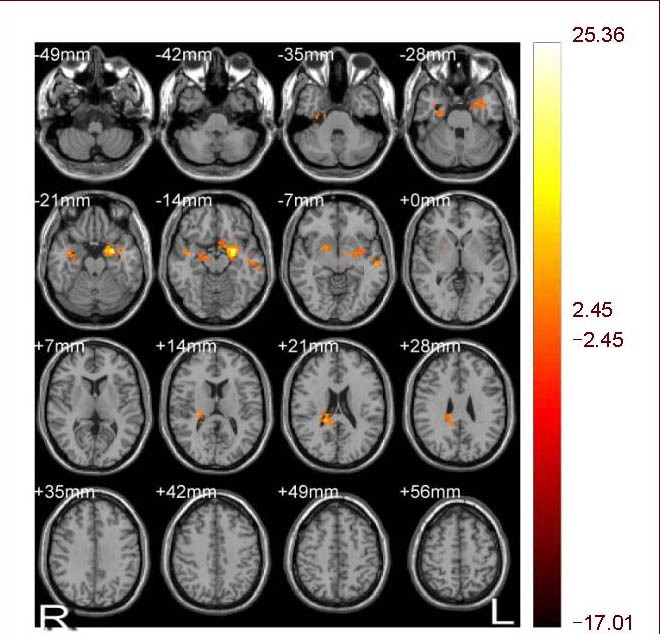
Image of brain functional connectivity in low-back and leg pain patients with lumbar disc herniation following body acupuncture. Bilateral amygdala served as a seed point. R: Right; L: left.
Table 4.
Changes in brain functional connectivity before and after body acupuncture using the amygdala as a seed point (Two temporal clusters)
DISCUSSION
Concept of default mode network and clinical application of brain function analysis at resting state
Raichle et al[6] found that blood oxygen level-dependent signal has a high time correlation in the medial prefrontal lobe, anterior cingulated gyrus, posterior cingulated gyrus and inferior parietal lobule, and proposed a concept of a default-mode network. The resting-state brain functional network of Alzheimer's disease, epilepsy and Parkinson's disease differs from healthy persons[7,8,9]. The analysis of resting-state brain functional networks is significant for changes in complicated functions following acupuncture.
Liu et al[10] confirmed that acupuncture at the Zusanli (ST36) acupoint and non-acupoint could enhance the functional connectivity of different brain regions, which contained the somatosensory area, motor area and visceral nerve center, suggesting that acupuncture exerts effects on organs and the whole body by the networks in the brain. Resting-state functional MRI can be used to analyze the connectivity of neural networks of various brain regions following acupuncture and to compare the central mechanisms of different types of acupuncture.
Resting-state brain functional connectivity after acupuncture
The amygdala, an important structure of the limbic system, contains many nuclear groups of different sizes, of which some nuclear groups are strongly associated with the coding and modulation of pain. Results from this study revealed that following balanced acupuncture, the brain regions that had a strong time correlation with the bilateral amygdala were composed of the putamen, thalamus, superior temporal gyrus, insular lobe, brain stem, middle temporal gyrus, orbit of superior frontal gyrus, inferior frontal gyrus, cingulated gyrus, ventral anterior nucleus, ventrolateral nucleus, medial frontal gyrus and superior frontal gyrus. The frequency of the low-frequency oscillation signal in these brain regions is associated with the amygdala in a resting state. That is, the resting-state brain has a functional network that correlates with pain regulation and this function is strengthened by balanced acupuncture. The enhancement of functional connectivity in these brain regions suggests that the periaqueductal gray, ventral tegmental area, compact part of the substantia nigra, peripeduncular nucleus and the tegmentum accept amygdala afference.
The external relation of the amygdala to the temporal lobe cortex and olfactory system is via projections to the hypothalamus and brainstem[11]. In this study, the functional connectivity was enhanced in the thalamus and brainstem of patients undergoing balanced acupuncture, suggesting that there was a functional connectivity between the amygdala, thalamus and brainstem. The enhancement of functional connectivity in the ventral anterior nucleus and ventrolateral nucleus suggests the enhanced functions in the periaqueductal gray, ventral tegmental area, compact part of the substantia nigra, peripeduncular nucleus and tegmentum. In addition, the amygdaloid complex is widely connected to many new cortical areas. The afference of the amygdaloid complex was from the frontal lobe, cingulum, insular cortex and temporal lobe cortex, whereas the efference of the amygdaloid complex is extensively involved in new cortices. In the present study, the functional connectivity was also enhanced in the hippocampal gyrus, superior temporal gyrus, insular lobe, middle temporal gyrus, orbit of superior frontal gyrus, inferior frontal gyrus, cingulated gyrus, medial frontal gyrus and superior frontal gyrus, which was consistent with a previous study[11], suggesting that this pain regulation-related functional network pathway exists and its function is fortified. Taken together, the central mechanism of balanced acupuncture exerts analgesia effects not through a single brain region, but through a complex network related to the amygdala. The periaqueductal gray, hypothalamus, somatosensory cortex I and II areas, motor cortex, caudate nucleus and limbic system are important pain regulation centers. In particular, the hypothalamic-limbic system is an important region involved in balanced acupuncture for analgesia. Balanced acupuncture activates the nerve-endocrine-immune system by changing the excitability of the nervous system, inhibiting inflammation, easing pain, balancing the nerve-endocrine-immune system, adjusting physiological functions, and achieving analgesic effects. Ma et al[12] reported that blood plasma β-endorphin contents significantly decreased at 7 days and blood plasma adrenocorticotropic hormone contents were significantly lower at 14 days after balanced acupuncture compared with the control group. These results indicated that balanced acupuncture could relieve pain. Balanced acupuncture probably controlled physical stress by affecting the secretion and metabolism of the central nervous system. In the present study, the function of the endogenous pain regulation network was obviously increased following balanced acupuncture, which was identical to results from previously published studies[12,13]. Results from this study revealed that brain regions that are strongly associated with the bilateral amygdala included the left thalamus, left putamen, ventrolateral nucleus, limbic lobe and cingulated gyrus in the body acupuncture group. Function of the endogenous pain regulation network was not changed after body acupuncture. This result indicates that the analgesic effect of body acupuncture does not work through the central nervous system. Yan et al[14] showed that the mechanism of body acupuncture for rat neuropathic pain was probably associated with the decreased release of excitatory amino acid neurotransmitters and the increased release of inhibitory amino acid neurotransmitters.
The amygdala is an important component of the endogenous pain regulation pathway. There are abundant fiber connections in the endogenous pain regulation pathway. Balanced acupuncture exerts analgesic effects by regulating the network function, whereas the analgesic effect of body acupuncture does not work through the central nervous system. Thus, balanced acupuncture exerts effects rapidly, and the effects can last for a long period. However, body acupuncture exerts effects more slowly.
SUBJECTS AND METHODS
Design
Quasi-experimental study.
Time and setting
Experiments were performed at the Department of Image, Guangdong Provincial Hospital of Traditional Chinese Medicine, China from March to September 2009.
Subjects
A total of 20 low-back and leg pain patients with lumbar disc herniation were recruited at the Department of Orthopedics, Department of Rehabilitation, Traditional Therapy Center, Guangdong Provincial Hospital of Traditional Chinese Medicine, China from March to September 2009.
Diagnostic criteria
Patients with lumbar disc herniation were diagnosed using CT or MRI, with the presence of ruptured annulus fibrosus and compressed soft tissues, resulting in low-back and leg pain.
Inclusion criteria
(1) History of lumbar trauma and acute episode of chronic lumbar muscle strain, onset or episode < 1 month; (2) right handedness; (3) 30–70 years old; (4) VAS pain score > 4; (5) radiating pain from the lumbar to the buttocks and lower limb; abdominal pressure (cough, sneeze) increases pain; and (6) straight-leg raising test and pick-up test showed positive reaction; knee and Achilles tendon reflex weakens or disappears.
Exclusion criteria
(1) Women in pregnancy or lactation; (2) presence of severe cardio-cerebrovascular, liver, kidney, hematopoietic system diseases; (3) patients experiencing neurosis and psychosis; (4) patients with calcification in protrusion, lateral recess stenosis, spinal stenosis, pyriformis syndrome, sciatica of the trunk, tumors, tuberculosis, fracture and spondylolisthesis of lumbar vertebra; (5) taking analgesics; (6) diagnosed as having lumbar disc herniation, without clinical symptoms; and (7) noncompliance.
Thus, 20 patients comprising 8 males and 12 females, with an average age of 50 ± 12 years were included. Protocols and risk were informed to subjects in accordance with Administrative Regulations on Medical Institution, issued by State Council of the People's Republic of China[15].
Methods
Balanced acupuncture method
All acupuncture sessions were conducted using a No. 30 sterile silver needle (1.5 cun; Huanqiu Medical Equipment, Suzhou, China) by a senior physician from the Department of Acupuncture and Moxibustion, Guangdong Provincial Hospital of Traditional Chinese Medicine, China. The Lumbago acupoint localized at the central point of the forehead was selected. The Lumbago acupoint, named as the position function, is supplied by the medial arterial venous branches and the supratrochlear nerve of the trigeminal nerve. A cross was made on the forehead, with the central point of the cross indicating the Lumbago acupoint.
Operation technique: lifting-inserting method was used. The needle was withdrawn when the patient felt the needling sensation. Unilateral low back pain received horizontal needling, no lifting or inserting. Pain was not controlled in severe low back pain patients. However, the needle could be maintained under no fainting condition during acupuncture. Needling sensation: mainly sour, numb, and swell up. Horizontal needling was done only once, without frequency, needle retaining time or interval time. The lifting-inserting method did not have a special depth, but took patients’ needling sensation as a standard.
Body acupuncture method
Acupoint selection: Weizhong (the midpoint of popliteal transverse line, between biceps femoris tendon and semitendinosus tendon), Dachangshu (lumbar part, below spinous process of the fourth lumbar vertebra, 1.5 cun from the midline), Ahshi acupoint (tender point) and Guanyuanshu (lumbar part, below spinous process of the fifth lumbar vertebra, 1.5 cun from the midline). Operation technique: All acupunctures were conducted using a No. 30 sterile silver needle (1.5 cun; Huanqiu Medical Equipment) by a senior physician from the Department of Acupuncture and Moxibustion, Guangdong Provincial Hospital of Traditional Chinese Medicine, China. The needle was held for about 20 minutes when the patient felt the needling sensation (insensible feeling or swelling). The needle was twisted once every 5–10 minutes, using mild reinforcing-reducing method. For patients with dull needling sensation, the manipulation could be slightly strong (with greater power).
MRI and parameter setting
Subjects’ heads were evaluated utilizing an Avanto 1.5T functional MRI (Siemens, Germany) before acupuncture and 10 minutes following the first acupuncture session. The scanning sequence was identical before and after acupuncture. During MRI, the patients were conscious, resting in a horizontal position, with eyes closed and normal respiration. Rubber ear plugs were applied to decrease noise. The head was fixed, and initiative and passive exercise was reduced to the utmost extent. A typical head coil was used for head fixation.
Functional imaging used an echo plane sequence. The parameters were as follows: repetition time/echo time/flip angle = 3 560 ms/50 ms/90°, visual field 230 mm, matrix 64 × 128, resolution 3.59 mm × 1.80 mm, sweep time of 3 seconds, with an interval of 5 seconds; axial view. The acquisition direction was parallel to the link of anterior and posterior parts of the corpus callosum, including the whole brain from telencephalon to cerebellum, 3 mm thickness, 36 slices. Anatomical images were collected at the same level as the functional images using a fast spin-echo sequence, T1-weighted images, repetition time/echo time/flip angle = 500 ms/11 matrix 192 × 192.
Data processing
The data were analyzed using Analysis of Functional NeuroImages software (Milwaukee, WI, USA). A time curve was estimated by convolution utilizing a Hamming bandpass filter. Low-frequency oscillation signals were obtained at a frequency of 0.015–0.100 Hz. Functional connectivity used the bilateral amygdala as the seed point. Cross correlation of seed point voxel i and brain voxel j was calculated, and the region related to time course of seed region was found to indicate the functional connectivity between the target region and the seed region. Using Fisher transformation, the cross correlation was transformed into a normal distribution Z:CCij ->Zij. The absolute value of the Z value was obtained, and then connectivity of this voxel Zi was calculated.
Assessment for curative effects
Pain was evaluated using a VAS 10 minutes after acupuncture in each group. Curative effects were assessed in accordance with the Criteria of Diagnosis and Therapeutic Effect of TCM Diseases. Curing: low back and leg pain disappeared; VAS score of 0; angle of straight-leg raising > 70°; did their previous work. Improvement: low back and leg pain lessened; VAS score of < 10; the lumbar function was improved. Ineffective: No improvement and VAS score of ≥10.
Statistical analysis
A single Z value was substituted in one-sample t-test using Analysis of Functional NeuroImages software. According to AlphaSim results, the cluster threshold was set as 243 mm3. After space correction, an intragroup threshold of P < 0.05 was produced.
Footnotes
Funding: This project was funded by the Scientific Research Innovation Program regarding Traditional Chinese Medicine of Guangzhou University of Chinese Medicine (Central mechanism of balanced acupuncture for lumbar disc herniation using functional MRI), No. 09CX068.
Conflicts of interest: None declared.
Ethical approval: This study was approved by the Ethics Committee, Guangdong Provincial Hospital of Traditional Chinese Medicine, China.
(Edited by Yin JZ, Yang LP/Qiu Y/Wang L)
REFERENCES
- [1].Ouyang BS. Short acupuncture and electroacupuncture for treatment of lumbar disc herniation hemorheology change observed. Zhongguo Zhen Jiu. 1999;1(12):723. [Google Scholar]
- [2].Guan ZH, Xu J, Tan BH. Hot needle instrument in the treatment of lumbar disc herniation mechanism. Zhenjiu Liuchuang Zazhi. 1998;14(5):28. [Google Scholar]
- [3].Zhao DL. Shanghai: Science and Technology Literature Press; 1996. Spinal Surgery. [Google Scholar]
- [4].Luo Y, Chen XY. The current situation of therapeutics for prolapse of lumbar intervertebral disc by traditional Chinese medicine and western medicine. Xiandai Zhongxiyi Jiehe Zazhi. 2009;18(9):1054–1055. [Google Scholar]
- [5].Wang WY. Beijing: Beijing Science and Technology Press; 1998. Chinese Balance Acupuncture. [Google Scholar]
- [6].Raichle ME, MacLeod AM, Snyder AZ, et al. A default mode of brain function. Proc Natl Acad Sci U S A. 2001;98(2):676–682. doi: 10.1073/pnas.98.2.676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Zhang ZQ, Lu GM, Tan QF. Development of functional MRI in locating epileptogenic focus. Zhongguo Yixue Yingxiang Jishu. 2006;22(12):1915–1918. [Google Scholar]
- [8].Chen ZL, Lu GM, Zhang ZQ, et al. Disturbances of default mode in focal epilepsy: a functional connectivity MRI study. Zhongguo Yixue Yingxiang Jishu. 2008;24(12):1916–1919. [Google Scholar]
- [9].Liu X, Liu B, Luo XD, et al. Magnetic resonance imaging of functional connectivity in Parkinson disease in the resting brain. Zhongguo Fangshexue Zazhi. 2009;43(3):253–260. [Google Scholar]
- [10].Liu B, Liu X, Chen J, et al. Study on the effects of acupuncture at acupoint and non-acupoint on functional connectivity of different brain regions with functional magnetic resonance imaging. Zhongguo Zhenjiu. 2009;29(12):981–986. [PubMed] [Google Scholar]
- [11].Elsevier: Churchill Livingstone; 2004. Susan Standring. Gray's Anatomy. [Google Scholar]
- [12].Ma WS, Zhang YM, Yuan H, et al. Effects of balance-acupuncture stimulation of “back pain” and “hip pain” points on plasma β-endorphin and ACTH contents in rats with lumbar disc herniation. Zhen Ci Yan Jiu. 2011;36(5):357–360. [PubMed] [Google Scholar]
- [13].Sun ZR, Wang S, Li XJ, et al. Benign Regulation of acupuncture on β- endorphin of rats with experimental sciatic nerve compressed. Zhongguo Zhongyiyao Keji. 2004;11(2) [Google Scholar]
- [14].Yan LP, Wu XT, Yin ZY, et al. Effect of electroacupuncture on the levels of amino acid neurotransmitters in the spinal cord in rats with chronic constrictive injury. Zhen Ci Yan Jiu. 2011;36(5):45–48. [PubMed] [Google Scholar]
- [15].State Council of the People's Republic of China. Administrative Regulations on Medical Institution. 1994 Sep 01; [Google Scholar]