

Introduction
Truancy continues to be a major problem in affecting most school districts in the U.S. Although truancy is hard to quantify, since a uniform definition of truancy is lacking and there is inconsistent reporting and tracking procedures across school districts, (National Center for School Engagement, 2006; US Department of Education, n.d.), it is estimated that thousands of youth are absent from school each day. For example, in 2003, the Monitoring the Future national survey of U.S. adolescents found high rates of student reports of skipping school one or more days in the previous 30 days among 8th graders (11%), 10th graders (16%), and 12th graders (35%)(Johnston, O’Malley, Bachman, & Schulenberg, 2004).
School districts vary in the quality of their collection and reporting of data on truancy. Los Angeles County and Colorado have been particularly diligent in their work in this area. Hence, we focus on more current data on truancy from these jurisdictions.
Recent statistics on truancy in Los Angeles County indicate high rates of unexcused absences, with the highest rates being found in urban high schools (Dropout Nation, 2010). Two hundred thousand Los Angeles County students were truant during the 2008-2009 school year, which represented 16 percent of all students attending schools in the county. Fifty-seven of L.A. County’s 88 school districts experienced truancy rates greater than 10 percent. Similarly, Colorado truancy data for 2010 to 2011 (Colorado Department of Education, 2011) indicated truancy rates (total student days unexcused absent/total days of possible attendance for all students) above ten percent for many schools, including several Denver area schools. Comparable statistics pointing to the high level of truancy problems can be found in other jurisdictions (Garry, 2001).
Truancy appears to be an early sign for a trajectory toward more negative behaviors (National Center for School Engagement, 2006). As Garry (2001) observed, truancy may be the beginning of a lifetime of problems among students who routinely skip school. Truancy has been shown to be associated with poor standardized test performance (Caldas, 1993; Lamdin, 1996), high school dropout (Bridgeland, Dilulio, & Morison, 2006), a stressed family life (Baker, Sigmon, & Nugent, 2001; Kearney & Silverman, 1995), and psychological and behavioral problems (Diebolt & Herlache, 1991; Egger, Costello, & Angold, 2003; Kearney & Silverman, 1995).
An additional issue is the relationship between substance use and truancy (Dembo et al., in press; Soldz, Huyser, & Dorsey, 2003). Recent national surveys and scientific studies consistently document that truant youth in the U.S. and in other counties are at high risk of involvement in drug use, particularly alcohol and marijuana. As might be expected, alcohol and marijuana use is higher among truant youth, compared to youth who attend school regularly. Analyzing longitudinal data on youth who grew up in socially disorganized neighborhoods in Denver, Colorado, Henry and Huizinga (2007) found truancy was a significant predictor of initiating the use of tobacco, alcohol, and marijuana. Hallfors et al.’s (2002) meta-analysis of school survey data found truancy was a strong marker for youth substance use. Henry and Thornberry (2010) obtained similar results in their analyses of data from the Rochester Youth Development Study. Their longitudinal, multivariate analyses documented robust contemporaneous and prospective relationships between truancy and substance use. Their findings highlight that truancy is not only “associated with an increased odds of initiation of substance use, but once an adolescent initiates substance use, truancy is also related to a substantial escalation of use” (Henry & Thornberry, 2010, p. 123). Using pooled data from the 1997 and 1998 National Household Surveys on Drug Abuse, Roebuck, French, & Dennis (2004) sought to determine the relationships between marijuana use and school attendance. Marijuana use was positively associated with school dropout and truancy in all the models they tested. Duarte and Escario (2005) found alcohol abuse and truancy to be related problems among the Spanish youth they studied. Similar results were obtained by Siziya, Muula, and Rudatsikira. (2007) in their study of Swaziland youth.
Recent research results have highlighted the importance of addressing marijuana use among youth. The Monitoring the Future 2012 survey of youth indicates marijuana remains the most widely used illicit drug. Following several years of reduced use from 2006 to 2008, marijuana use has increased. In 2010, significant increases in daily use of the drug were found among 8th grade, 10th grade, and 12th grade youth. There was a non-significant increase in use in 2011, followed by non-significant declines in daily use among 8th grade youth and a leveling of use among 12th grade youth. Relatedly, the perceived risk of using marijuana declined in all grades in 2012, suggesting a likely future increase in use of the drug (Johnston, O’Malley, Bachman, & Schulenberg, 2013). (These trends are in contrast to youth alcohol use, another widely used substance. Monitoring the Future data indicate a downward trend in alcohol use among 8th grade, 10th grade, and 12th grade youth in recent years, with a record decline in past month use among 8th graders [Johnston et al., 2013]).
Further, a recent report on the Dunedin Study, a prospective, longitudinal investigation of the association between marijuana use and neuropsychological impairment among a birth cohort of 1,037 individuals followed from birth in 1972/1973 through age 38 highlights the adverse effects of persistent use of the drug. Neuropsychological testing conducted at age 13, before initiation of use, and again at age 38 found decline across several domains of functioning, particularly executive functioning and processing speed. IQ was also affected by marijuana use. Study participants who never used marijuana experienced a slight increase in IQ. On the other hand, participants diagnosed as cannabis dependent or persistent users of marijuana at one or more of the study waves experienced an IQ decline of approximately 6 points. Cessation of marijuana use did not restore neuropsychological functioning among persistent users of the drug. The results highlight the importance of prevention and policy efforts to inform the public of the harmful effects of marijuana use in adolescence on later neuropsychological functioning, delaying the onset of cannabis use until adulthood, and fostering cessation of marijuana use, especially among youth beginning use of the drug in adolescence (Meier et al., 2012).
Truancy is often treated as a management and disciplinary problem (DeKalb, 1999; Diebolt & Herlache, 1991; Dougherty, 1999). Programs typically focus on identifying, locating, and transitioning truant youth back into their respective schools with sanctions and/or citations without much or any attention on identifying and referring services for the underlying psychosocial problems, including substance abuse (Dembo & Gulledge, 2009). Responding to truant youth with counseling or therapy provides an excellent opportunity to reduce the likelihood they will experience other negative outcomes, including future contact with the juvenile justice system.
Brief interventions are promising solutions for substance use treatment among truancy populations because they offer short-term treatment options that are easily transportable to various settings. Brief interventions can be as brief as a single, 15-minute discussion, but typically they range between 2 to 4 standard-length sessions (Breslin, Li, Sdao-Jarvie, Tupker, & Ittig-Deland, 2002).
The present study utilizes a brief intervention for substance abuse among youth developed by Winters and his associates (Winters, Fahnhorst, Botzet, Lee, & Lalone, 2012; Winters & Leitten, 2007) that integrates techniques from Motivational Interviewing (MI), Rational-Emotive Therapy (RET), and Problem-Solving Therapy (PST). MI is a client-centered counseling technique developed specifically for substance abuse intervention (Miller, 1983). The techniques of MI include increasing self-efficacy and increasing readiness for change (Miller & Rollnick, 1991). MI has demonstrated effectiveness with treating substance-abusing adolescents (e.g., D’Amico, Miles, Stern, & Meredith, 2008; Stein et al., 2011; Tait & Hulse, 2003). RET is a form of cognitive behavior therapy that focuses on correcting negative and self-defeating emotions that interfere with an individual’s abilities to achieve goals (Bernard & Joyce, 1984). While little research on RET, itself, has examined its effect on reducing substance use among adolescents, specifically, research has demonstrated RET has a significant impact on problem behaviors among youth (Gonzalez et al., 2004). PST recognizes that problem-solving skills are key to an individual’s ability to cope and focuses on applying general problem-solving and coping skills to various situations (D’Zurilla & Goldfried, 1971). PST has demonstrated promise for adolescent substance use relapse prevention (Bry, Conboy, & Bigsay, 1986; Fromme, Marlatt, Baer, & Kivalahan, 1994). By integrating techniques from MI, RET, and PST, the brief intervention encourages the development of adaptive beliefs and problem-solving skills to promote abstinence from substance use and prevent relapse among youth populations. This brief intervention has demonstrated effectiveness in reducing substance use among adolescents (Winters et al., 2012) in a school setting.
There is a critical need to evaluate the effect of intervention services on improving psychosocial outcomes, and reducing substance use, among truant youth. The purpose of the present study is to examine the effectiveness of an ongoing NIDA-funded Brief Intervention (BI) project in reducing substance use by truant youth in a southern urban region. Specifically, the BI project is a prospective, longitudinal, intervention study of substance-involved truant youth. The study’s design included random assignment of youth to assess the impact of two Brief Intervention strategies (BI-Youth and BI-Youth plus Parent) in comparison to Standard Truancy Services (control condition) on youth psychosocial functioning. Previous studies for this project have examined the diversity of the sample with regard to psychosocial problems (substance use, emotional, sexual, and behavioral issues) at baseline and over time. This is the first study from the BI project that examines the influence of BI treatment on future substance use. The present report describes the impact of BI services on the youths’ alcohol and marijuana use in an 18-month post-intervention follow-up period. Following a discussion of the method and our results, we consider their implications for intervention services.
Materials and Method
Design and Hypotheses
All study procedures were approved and monitored for ethics by the university Institutional Review Board (IRB). The baseline and follow-up interviews were conducted by trained research staff, following procedures approved by the IRB. As described in more detail by Dembo et al. (2011; 2012), the main place of recruitment into the BI project was the Truancy Intake Center (TIC) located at the Hillsborough County Juvenile Assessment Center. In addition, eligible participants were recruited from a community diversion program and referrals were accepted from any Hillsborough County School District (HCSD) social worker or guidance counselor who knew of eligible youth. At both locations, project enrollment proceeded as follows. A project staff member met with the youth and his/her parent/guardian, and provided an overview of the project and its services. Eligible participants were informed that project services were free, voluntary, and provided in-home. For interested participants, an in-home meeting was scheduled to discuss the project further, to answer any questions they had, complete the consent and assent processes, and to conduct separate baseline interviews with the youth and his/her parent/ guardian.
Following the completion of the consent and assent processes and baseline interviews, the youth and parent/guardian were randomly assigned to one of three project service conditions: (1) BI-Youth (BI-Y), (2) BI-Youth plus Parent (BI-YP), or (3) the Standard Truancy Services (STS). Data were also collected for four follow-up periods: the first three months after the intervention (referred to as 3-month follow-up period); the second three months, or months four through six after the intervention (referred to as 6-month follow-up period); months seven through twelve after the intervention (referred to as 12-month follow-up period); and months 13 through 18 after the intervention (referred to as 18-month follow-up period).
Two hypotheses guided this study. The first hypothesis was that truant youth receiving either of the intervention services (BI-Y or BI-YP) will have a lower rate of marijuana use during the 18-month post-intervention period, than youth receiving STS. The second hypothesis was that truant youth receiving BI-YP services will exhibit lower post-intervention marijuana use, than youth receiving BI-Y services. The hypothesized effect of BI-YP services is premised on epidemiological and clinical studies which indicate that parent monitoring and support, addressed in the BI-YP session, are linearly related to age of onset of illicit drug use, even when comorbidity is controlled (Chilcoat & Anthony, 1996), are associated with reduced risk for drug use (e.g., Clark, Kirisci, & Tarter, 1998; Gorman-Smith, Tolan, Loeber, & Henry, 1998), and contribute to positive outcomes for youth in recovery (Williams, Chang, & Addiction Centre Adolescent Research Group, 2000; Winters, 1999).
Participants
Eligible youths met the following criteria: (1) age 11 to 17, (2) no official record of delinquency or up to two misdemeanor arrests, (3) some indication of alcohol or other drug use, as determined, for example, by a screening instrument (Personal Experience Screening Questionnaire [PESQ, Winters, 1992]) or as reported by a HCSD social worker located at the TIC, and (4) lived within a 25-mile radius of the TIC. The total sample, from which the subsample of youths involved in the present study was drawn, consisted of 300 youths, who were enrolled and completed baseline interviews in the truancy intervention project between March 2, 2007 and June 22, 2012. Follow-up data at all time points, through 18-month follow-up, were available on n = 215 of these youths in regard to their marijuana use.
The characteristics of the subsample were quite similar to the full sample. Most youths in the study were male (65%), and averaged 14.81 years in age (SD = 1.34). Thirty-seven percent of the youths were Caucasian, 27% were African American, 26% were Hispanic, 1% were Asian, and 7% were from other, mainly multi-ethnic backgrounds.
Interventions
Brief interventions
The primary goal of the BI therapist sessions was to promote abstinence and prevent relapse among drug using adolescents. The BI incorporated elements of MI, RET and PST to develop adaptive beliefs and problem-solving skills. Drug involvement was viewed as learned behavior that develops within a context of personal, environmental, and social factors (Catalano, Hawkins, Wells, & Miller, 1991; Clark & Winters, 2002) that shape and define drug use attitudes and behaviors. Maladaptive beliefs and problem-solving skill deficits, developed over the course of an adolescent’s learning history and prior experience with drugs, were viewed as primary determinants of drug use. The goal of the BI therapy was to diminish factors contributing to drug use (e.g., maladaptive beliefs) and promote factors that protect against relapse (e.g., problem solving skills) (Winters et al., 2012; Winters & Leitten, 2007). As noted earlier, the BI presented here was adapted from previous work using brief intervention on drug-abusing youth (Winters & Leitten, 2001).
A BI counselor received training on the treatment manual adapted from previous brief interventions for drug-using youth (Winters & Leitten, 2001), and personal training from a skilled trainer on all intervention components. Then, the counselor provided BI services to several practice cases. The BI trainer reviewed these sessions with a focus on developing therapist adherence (aided by a rating checklist) and competence (e.g., perceived warmth and interest in the client, presentation clarity, ability to elicit client feedback). Following approval by the trainer, the counselor began to receive project families. With youth and parent/guardian permission, the BI sessions were tape recorded for ongoing fidelity/adherence assessment. Similar to other BI research, fidelity measures of the BI counselor monitored session content and exercises, and whether the counselor adhered to principles of motivational interviewing (i.e., establishing rapport; being a good listener, etc.).
Depending upon the treatment condition, participating families received 2-3 BI sessions. Youths randomly assigned to the BI-Youth (BI-Y) condition were administered two BI sessions, while no sessions were held with their parents/guardians. Youths randomly assigned to the BI-Youth plus Parent (BI-YP) condition were administered two BI sessions, and their parents/guardians were administered one BI session.
Each BI session lasted for 1-1/4 hours, and the sessions occurred about a week apart. The first BI session with the youth focused on discussing the youth’s substance use and related consequences, the level of willingness to change, the causes and benefits of change, and what goals for change the youth wanted to select and pursue. The youth was encouraged to pursue goals of drug abstinence or reduction in drug use. In the second session with the youth, the counselor reviewed the youth’s progress with the agreed upon goals, identified risk situations associated with difficulty in achieving goals, discussed strategies to overcome barriers toward goal achievement, reviewed where the youth was in the process of change, and negotiated either continuation or advancement of goals. Informed by an integrated behavioral and family therapy approach, the parent BI session addressed the youth’s substance use issues, parent attitudes and behaviors regarding this use, parent monitoring and supervision to promote progress towards their child’s intervention goals, and parent communication skills to enhance youth-parent connectedness.
Standard truancy services (STS)
In addition to the normal truancy services provided by the HCSD, STS youths/families received a referral service overlay of three weekly hour-long visits by a project staff member. Reflecting the concept of equipoise (Freedman, 1987), this referral assistance provided truant youth and their families in the control condition with an additional resource that is not routinely available to them, and also controlled for service exposure. On each contact occasion, the staff member carried a copy of a Hillsborough County government-developed agency and service resource guide. Developed over a period of several years, this resource guide contained hundreds of agency listings. The agency listing information included contact information such as a telephone number, e-mail/website address, and street address. Participants in the STS condition were provided with any agency listing information they felt they needed. In addition to a general inquiry on events since the last session, the staff member asked the youth and his/her parents/guardians: (1) if they used any services and (2) if there were any additional service needs–and, if so, provided an appropriate referral. The point of the STS condition was simply to provide publicly available contact information on local services available to the youth’s family. No form of counseling or therapy was offered in the STS condition.
Procedures
Each youth and parent/guardian was paid $15 for completing the in-home, baseline interview. The baseline interviews for parents/guardians averaged 30 minutes; the youth interviews averaged one hour. The 3-month follow-up interview was scheduled for 90 days from the date of the youth’s last participation in project services (i.e., the last intervention or Standard Truancy Services session). The 6-month follow-up interview date was scheduled for 90 days following completion of the 3-month follow-up interview; the 12-month follow-up interview was scheduled for 180 days after the completion date of the 6-month follow-up interview; and the 18-month follow-up interview was scheduled for 180 days after the completion date of the 12-month follow-up interview. On 16 occasions, when a follow-up interview was not performed near the scheduled time, a retrospective interview was performed at the same time as the following interview. For example, if a 6-month interview was not performed approximately three months after the 3-month interview, two interviews were performed approximately nine months after the 3-month interview. One was a retrospective 6-month interview, covering the period of three months after the 3-month interview. The other was the 12-month interview, from the end of the period covered in the retrospective 6-month interview until the time of the interview being conducted. Each youth and parent/guardian was paid $15.00 for each follow-up interview. Most youths were interviewed in their homes; at each follow-up time point, fewer than 3% of the youths were interviewed in a secure program setting, such as residential commitment programs, county jails, or a juvenile detention center.
Completion of follow-up interviews depended on when youths entered the project: 3-month (n = 282), 6-month (n = 281), 12-month (n = 245), and 18-month (n = 215) follow-up interviews. Youths who began participation early in the project completed all four follow-up interviews, whereas youths who enrolled most recently were not yet due for any follow-up interview at the time of the present study. Overall completion rates of 94.0%, 93.7%, 92.1%, and 88.5% were achieved for the 3-month, 6-month, 12-month, and 18-month follow-up interviews, respectively. Of the completed follow-up interviews, 95.4% of the 3-month, 95.0% of the 6-month, 96.3% of the 12-month, and 99.1% of the 18-month interviews were completed within 60 days of the scheduled interview date.
Measures
Data Collection Instruments
The main data collection instruments were the Adolescent Diagnostic Interview (ADI, Winters & Henly, 1993), and the Adolescent Diagnostic Interview- Parent/Guardian (ADI-P, Winters & Stinchfield, 2003). Both the ADI and ADI-P were designed to be delivered within a highly structured and standardized format (e.g., most questions are yes/no) to capture DSM-IV criteria for substance use disorders and related areas of functioning. Item construction primarily involved advice from an expert panel and feedback from field testers. DSM guidelines and results from the statistical analysis provided the basis for scoring rules. Reliability and validity studies, involving over 1000 drug clinic adolescents for the ADI and about 200 parents/guardians for the ADI-P, provide a wide range of psychometric evidence pertaining to inter-rater agreement, test-retest reliability, convergent validity (with clinical diagnoses), self-report measures, and treatment referral recommendations (Winters & Henly, 1993; Winters & Stinchfield, 2003).
Sociodemographic measures
Our evaluation of the effectiveness of BI services on future substance use controlled for a number of socio-demographic measures. Several youth sociodemographic characteristics were used in this study: age (in number of years); gender; ethnicity; living situation; family annual income; and family experience of stressful/traumatic events. Table 1 shows the distributions of these sociodemographic characteristics.
Table 1.
Background Characteristics of the Youths at Baseline (n=300)
| Age: | |
| Mean | 14.80 |
| Standard Deviation | 1.30 |
| Gender: | |
| Male | 63.0% |
| Female | 37.0% |
| Ethnicity: | |
| Asian | 1.0% |
| African American | 25.7% |
| Hispanic | 28.7% |
| Native American | 0.3% |
| Caucasian | 37.3% |
| Other (Mixed race) | 7.0% |
| Who Youth Lives With | |
| Both birth mother and birth father | 16.7% |
| Birth mother alone | 33.3% |
| Birth mother with stepfather/boyfriend | 23.0% |
| Birth mother with relative or friend | 10.3% |
| Birth father alone | 2.7% |
| Birth father with stepmother or girlfriend | 4.3% |
| Birth father with relative or friend | <1% |
| Adoptive parent(s) | 2.7% |
| Grandparent(s) | 4.3% |
| Other relative(s) | 1.7% |
| Other | <1% |
| Family Annual Income Level (n = 297) | |
| Less than $5,000 | 5.1% |
| More than $5,000 up to $10,000 | 8.1% |
| More than$10,000 up to $25,000 | 26.3% |
| More than $25,000 up to $40,000 | 27.9% |
| More than $40,000 up to $75,000 | 22.9% |
| More than $75,000 | 9.8% |
| Family Experience of Stressful/Traumatic Events | |
| Unemployment of parent | 50.3% |
| Divorce of parents | 38.7% |
| Death of loved one | 57.7% |
| Serious illness | 31.0% |
| Victim of violent crime | 17.3% |
| Eviction from house or apartment | 17.0% |
| Legal problem resulting in jail time or detention | 26.4% |
| Accidental injury requiring hospitalization | 12.0% |
| Other stressful/traumatic event | 48.8% |
| Mean | 2.99 |
| Standard Deviation | 1.76 |
Information was obtained from the youth and parent/guardian interviews regarding who the youth was living with. As can be seen in Table 1, relatively few youth were living with both of their biological parents, birth father, or grandparents. On the other hand, a third of the youth in both the full sample and subsample were living with their mother alone. We created a variable reflecting youth residence with mother (1= living with mother alone) or in another living arrangement (0 = other living arrangement) for our analysis.
At their baseline interviews, parents/guardians were asked for information regarding their annual family income. Overall, the families in the project had modest annual incomes. Nearly 40% of the families had an annual income of $25,000 or less, 24% reported annual incomes between $40,000 and $75,000, and 10% indicated their annual incomes were greater than $75,000. The median annual family income was between $25,001 and $40,000.
Family Experience of Stressful/Traumatic Events
The youths’ parents/guardians were asked at baseline interview to indicate if the youth or their family ever experienced various stressful or traumatic events. Large percentages of subsample youth/families had these experiences, with unemployment of parent (48%), divorce of parents (38%), death of a loved one (59%), serious illness (32%), and a legal problem resulting in jail or detention (25%) being noteworthy. In addition, 46% of the parents/guardians reported other traumatic experiences (e.g., youth being placed in foster care, not having a relationship with father, fighting with brothers and sisters, losing the opportunity to obtain a driver’s license, separation from mother). Overall, an average of 2.99 stressful/traumatic events were reported (SD=1.76) (see Table 1).
Marijuana use
Marijuana use was measured through self-report questions on the ADI (Winters & Henly, 1993) and the results of urine tests (UA), both of which were administered at baseline interview and at each follow-up interview. The ADI questions probed the use of marijuana as: never, less than five times, or five or more times. Urine specimens using the Onsite CupKit® urine screen procedure were also collected to assess recent drug use. For marijuana (THC), urine test positive threshold levels were 50 ng/ml of urine. The surveillance windows were 5 days for moderate users of marijuana, 10 days for heavy users of marijuana, and 20 days for chronic users.
For each time point, we combined the self-reported marijuana use and marijuana urine test data into an overall measure of marijuana use involving six categories: (1) marijuana use denied and UA test for marijuana negative; (2) marijuana use denied and UA test data missing (due to reasons beyond the youth’s control [e.g., incarcerated]); (3) marijuana use denied and UA test data missing (not due to reasons beyond the youth’s control [e.g., participant refusal]); (4) UA test missing or negative for marijuana, but youth reported marijuana use one to four times; (5) UA test missing or negative, but youth reported marijuana use five or more times; (6) UA test positive for marijuana. The distributions of these polytomous data are presented in Table 2.
Table 2.
Youth Marijuana Use (Self-Report and Urine Test) Over Time
| Baseline (n = 300): | |
|
| |
| Denied use and urine test results negative | 7.0% |
| Denied use and urine test missing - reasons beyond control | 0.3% |
| Denied use and urine test missing - refusal | 0.3% |
| Reported use 1-4 times and urine test missing/negative | 17.0% |
| Reported use 5 or more times and urine test missing/negative | 29.3% |
| Urine test positive | 46.0% |
|
| |
|
At 3-month follow-up (n = 282):
| |
| Denied use and urine test results negative | 39.0% |
| Denied use and urine test missing - reasons beyond control | 3.9% |
| Denied use and urine test missing - refusal | 2.5% |
| Reported use 1-4 times and urine test missing/negative | 11.7% |
| Reported use 5 or more times and urine test missing/negative | 7.4% |
| Urine test positive | 35.5% |
|
| |
|
At 6-month follow-up (n = 281):
| |
| Denied use and urine test results negative | 31.0% |
| Denied use and urine test missing - reasons beyond control | 4.6% |
| Denied use and urine test missing - refusal | 2.1% |
| Reported use 1-4 times and urine test missing/negative | 10.3% |
| Reported use 5 or more times and urine test missing/negative | 8.2% |
| Urine test positive | 43.8% |
|
| |
|
At 12-month follow-up (n = 245):
| |
| Denied use and urine test results negative | 32.2% |
| Denied use and urine test missing - reasons beyond control | 4.1% |
| Denied use and urine test missing - refusal | 0.4% |
| Reported use 1-4 times and urine test missing/negative | 8.6% |
| Reported use 5 or more times and urine test missing/negative | 11.8% |
| Urine test positive | 42.9% |
|
| |
|
At 18-month follow-up (n = 215):
| |
| Denied use and urine test results negative | 30.2% |
| Denied use and urine test missing - reasons beyond control | 4.7% |
| Denied use and urine test missing - refusal | 1.4% |
| Reported use 1-4 times and urine test missing/negative | 8.8% |
| Reported use 5 or more times and urine test missing/negative | 5.6% |
| Urine test positive | 49.3% |
Time-at-risk
From official and interview records, we obtained information on placement in a secure facility, either treatment or incarceration, for youths with an 18-month follow-up interview. Four youths spent a sizable number of days in a secure facility during their 18 month follow-up period. Although three of the youths were in residential facility during the entire period, one residential facility permitted weekend passes after 30 to 45 days of treatment (contingent on negative UA test results). Since it is possible youth may have had access to marijuana during their time in a secure facility, these cases were also included in the analyses. (Exclusion of youths in a secure facility during the 18-month follow-up period did not change the results of the analyses reported in this study.)
Analysis Strategy
We completed ordinal regression analyses to examine the relative predictive ability of the variables discussed in the methods section on marijuana use at 18-month follow-up. The regression analyses were run using Mplus version 7.0 (Muthén & Muthén, 1998-2012), a versatile, multivariate statistical modeling program that estimates a variety of models for continuous and categorical observed and latent variables. The analyses involved WLSMV estimation (a robust weighted least squares estimator using a diagonal weight matrix). Because the time of entry into the study determined the number of follow-up interviews each youth and parent/guardian received, the data that are missing are a consequence of the study design. Accordingly, the Mplus feature allowing for maximum likelihood estimation of missing values was used to treat the missing data (Muthen & Muthen, 1998-2012).
Given the time ordering of the marijuana use variables, an auto-regressive lag model was estimated. As a preliminary analysis step, we first estimated the basic model depicted in Figure 1.
Figure 1.
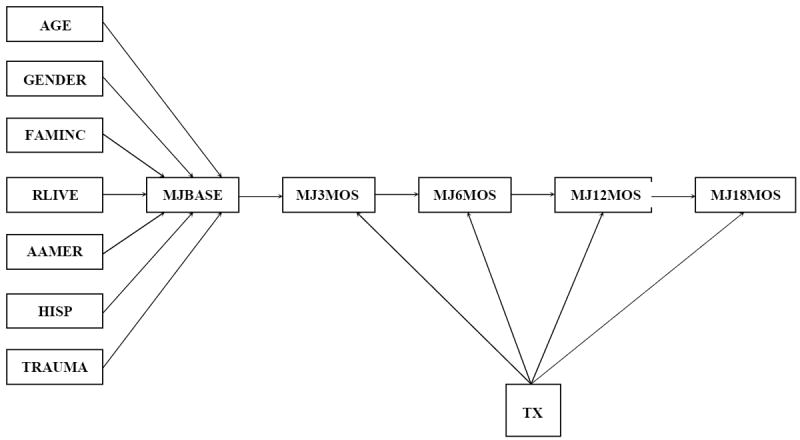
The Basic Auto-Regressive Lag Model
As Figure 1 shows, the covariates of age, gender, family income level, who youth lives with, being African American, Hispanic, and family stress/trauma experiences are specified to influence baseline marijuana use. Each of the following marijuana use time points is regressed its preceding time point of use of the drug. Finally, an overall STS vs BI [BI-Y+BI-YP] intervention effect is specified on marijuana use as 3 month, 6 month, 12 month, and 18 month follow-up.
Estimation of this model resulted in a poor fit to the data (chi-square= 60.60, df=36, p=0.0063). Inspection of the modification indices indicated model fit could be improved by including covariates at a number of time points. Hence, the basic autoregressive model was refined to incorporate these covariate effects. The revised model that was tested is shown in Figure 2.
Figure 2.

The Revised Auto-Regressive Lag Model
Note: Displayed model was used to compare STS vs BI (BI-Y+BI-YP) and BI-Y vs BI-YP. The model comparing STS vs BI-Y included a direct effect from GENDER to MJ18MOS. The model comparing STS vs BI-YP included direct effects from GENDER and AAMER to MJ18MOS.
Four autoregressive lag models were estimated: Model 1: an overall intervention effect (BI-Y + BI-YP = 1, versus STS = 0); Model 2: comparison of the BI-Y vs STS conditions; Model 3 comparison of the BI-YP vs STS conditions, and Model 4: comparison of the BI-YP vs BI-Y conditions. For these analyses, the directional hypotheses were considered significant at the .05 level by a one-tailed test.
Results
Intervention Group Comparison of Demographic, Alcohol Use, and Marijuana Use Variables
We compared the STS, BI-Y, and BI-YP groups in regard to their baseline background characteristics, and marijuana use. No significant differences were found for each of these variables. (These results have been omitted due to space concerns. A copy is available from the senior author upon request.)
Assessment of Model 1: (BI-Y + BI-YP = 1, versus STS = 0)
Table 3 displays the results of our estimation Model 1. The model fit to the data was quite good (chi-square=34.90, df=37, p=0.57, RMSEA=0.000; CFI=1.000 TLI=1.005). Findings indicate a significant positive effect of age on baseline marijuana use (estimate=0.174) and 6 month follow-up use of the drug (estimate=0.308). There are also significant autoregressive effects of marijuaua use at successive time points (18 month use on 12 month use [estimate=0.558]; 12 month use on 6 month use [estimate=0.838]; 6 month use on 3 month use [estimate=0.861]; and 3 month use on baseline use [estimate=0.727]). Importantly, a significant over all BI intervention effect is found for 18 month follow-up marijuana use (estimate= -0.490). Truant youth receiving BI services are less likely to be involved in marijuana use, than youth receiving STS services. Together, the predictor variables explain 48% of the variance in 18-month follow-up marijuana use. The estimated intervention effect size on marijuana use at 18 month follow-up is, following Muthèn & Asparouhov (2002) -0.509 (moderate). The thresholds refer to a point on the assumed underlying continuous scale for marijuana use at each time point (Joreskog & Sorbom, 1993).
Table 3.
Auto-Regressive Lag Model Estimation Results
| Variables | Model 1: STS vs. BI-Y + BI-YP | Model 2: STS vs. BI-Y | ||||
|---|---|---|---|---|---|---|
| Estimate | S.E. | Est./S.E. | Estimate | S.E. | Est./S.E. | |
| 18-Month Follow-Up Marijuana Use ON | ||||||
| 12-Month Follow-Up Marijuana Use | 0.558*** | 0.095 | 5.848 | 0.547*** | 0.115 | 4.742 |
| Gender (1 = Female) | -0.849* | 0.413 | -2.054 | |||
| Intervention (1 = Intervention Condition[s]) | -0.490+ | 0.277 | -1.767 | -0.841** | 0.323 | -2.599 |
| 12-Month Follow-Up Marijuana Use ON | ||||||
| 6-Month Follow-Up Marijuana Use | 0.838*** | 0.107 | 7.838 | 0.821*** | 0.131 | 6.261 |
| Intervention | -0.041 | 0.277 | -0.148 | -0.074 | 0.323 | -0.229 |
| 6-Month Follow-Up Marijuana Use ON | ||||||
| 3-Month Follow-Up Marijuana Use | 0.861*** | 0.110 | 7.839 | 0.855*** | 0.131 | 6.508 |
| Age | 0.308*** | 0.070 | 4.386 | 0.317*** | 0.086 | 3.669 |
| Intervention | 0.053 | 0.233 | 0.229 | 0.101 | 0.260 | 0.388 |
| 3-Month Follow-Up Marijuana Use ON | ||||||
| Baseline Marijuana Use | 0.727*** | 0.106 | 6.880 | 0.624*** | 0.120 | 5.209 |
| Intervention | 0.180 | 0.229 | 0.786 | 0.003 | 0.255 | 0.010 |
| Gender × Intervention | -0.488 | 0.411 | -1.190 | -0.009 | 0.446 | -0.020 |
| Age | 0.039 | 0.071 | 0.557 | 0.033 | 0.085 | 0.381 |
| Baseline Marijuana Use ON | ||||||
| Age | 0.174*** | 0.051 | 3.433 | 0.147* | 0.061 | 2.407 |
| Gender | -0.069 | 0.269 | -0.255 | -0.055 | 0.266 | -0.205 |
| Family Income Level | 0.017 | 0.066 | 0.261 | -0.010 | 0.082 | -0.120 |
| Who Youth Lives With (1=Mother Only) | 0.189 | 0.163 | 1.161 | 0.305 | 0.212 | 1.437 |
| African-American (1 = African-American) | 0.213 | 0.194 | 1.097 | 0.101 | 0.242 | 0.416 |
| Hispanic (1 = Hispanic) | -0.090 | 0.181 | -0.500 | 0.106 | 0.224 | 0.474 |
| Family Experience of Stress/Trauma | -0.006 | 0.043 | -0.135 | -0.007 | 0.052 | -0.143 |
Note. Two-tailed p-values:
p < .05;
p < .01;
p < .001.
Significant at p<.05 for a one-tailed test.
Assessment of Model 2: (BI-Y = 1, versus STS = 0)
Table 3 also displays the results of our estimation Model 2. The model fit to the data was quite good (chi-square=32.89, df=36, p=0.62, RMSEA=0.000; CFI=1.000 TLI=1.013). Findings indicate a significant positive effect of age on baseline marijuana use (estimate=0.147) and 6 month follow-up use of the drug (estimate=0.317). There are also significant autoregressive effects of marijuana use at successive time points (18 month use on 12 month use [estimate=0.547]; 12 month use on 6 month use [estimate=0.821]; 6 month use on 3 month use [estimate=0.855]; and 3 month use on baseline use [estimate=0.624]). Gender is significantly and negatively related to marijuana use at 18 month follow-up, indicating girls are less likely to be involved with this drug at that time point, than boys. Importantly, again a significant intervention effect is found for 18 month follow-up marijuana use (estimate= -0.841), indicating youths receiving BI-Y services are less likely to be involved in marijuana use than STS youths. Together, the predictor variables explain 53% of the variance in 18-month follow-up marijuana use. The estimated intervention effect size on marijuana use at 18 month follow-up is, following Muthèn & Asparouhov (2002), -0.941 (large).
Assessment of Model 3: (BI-YP= 1, versus STS = 0)
The results of our estimation of Model 3, comparing BI-YP and STS youth, are also shown in Table 3. The model fit to the data was very good (chi-square=34.58, df=35, p=0.49, RMSEA=0.000; CFI=1.000 TLI=1.001). Findings indicate a significant positive effect of age on baseline marijuana use (estimate=0.207) and 6 month follow-up use of the drug (estimate=0.317). Youth who live with their mothers only are significantly more likely to be involved in marijuana use at baseline, than youth living in other family arrangements (estimate=0.440). There are also significant autoregressive effects of marijuana use at successive time points (18 month use on 12 month use [estimate=0.704]; 12 month use on 6 month use [estimate=0.816]; 6 month use on 3 month use [estimate=0.996]; and 3 month use on baseline use [estimate=0.739]). Gender is significantly and negatively related to marijuana use at 18 month follow-up, indicating girls are less likely to be involved with this drug at that time point, than boys. African American youth are significantly more likely to be involved in marijuana use at 18 month follow-up, than non-African American youth. (There is some suggestion in the data, not reported in Table 3, that Hispanic youth are less involved in marijuana use at 3 month follow-up, than other youth in the study.) There are no significant direct intervention effects on marijuana use at any time point. However, reflecting a significant gender × intervention group interaction, girls who received BI-YP services were significantly less likely to be involved in marijuana use at 3 month follow-up, than boys (estimate=-0.980; a large effect size of -1.065 [Muthèn & Asparouhov, 2002]). Together, the predictor variables explain 70% of the variance in 18-month follow-up marijuana use. Comparing the results from the BI-Y vs STS and BI-YP vs STS analyses in Table 3, it is clear that BI-Y is the intervention condition influencing youth reductions in marijuana use at 18 month follow-up.
Assessment of Model 4: (BI-YP = 1, versus BI-Y = 0)
The results of our estimation of Model 4, comparing BI-YP and BI-Y youth, are also shown in Table 3. The model fit to the data was very good (chi-square=31.03, df=37, p=0.74, RMSEA=0.000; CFI=1 .000 TLI=1.020).
The Model 4 results shown in Table 3, comparing youth in the BI-Y vs BI-YP conditions, indicate age is significantly and positively related to baseline and 6 month follow-up marijuana use (estimates, =0.173 and 0.298, respectively). However, a significant gender × intervention group interaction effect was again found for 3 month follow-up marijuana use, with girls who received BI-YP services being less involved in marijuana use at 3 month follow-up, than boys (estimate=-1.095); a large effect size of -1.153 [Muthèn & Asparouhov, 2002]). Significant autoregressive marijuana use effects at successive time point are also found. Importantly, and in a lack of support for our second hypothesis, youth receiving BI-YP services were significantly more likely to be involved in marijuana use at 18 month follow-up, than youth receiving BI-Y services. Together, the predictor variables explain 45% of the variance in 18-month follow-up marijuana use. The estimated intervention effect size on marijuana use at 18 month follow-up is, following Muthen & Asparouhov (2002), 0.852 (large). We shall have more to say about this result in the discussion section.
There was a possible assessment validity problem for 13 follow-up interview cases completed by a former staff member. These assessments occurred during the first two years of the project and involved several assessments at each follow-up. The analyses reported in the present paper were re-computed with the thirteen cases suspected of having validity issues excluded. The results were unaffected by excluding these cases.
Discussion
The purpose of the present study was to examine the effects of the BI intervention (BI-Y + BI-YP) in reducing marijuana use at 18 month follow-up (Hypothesis 1) among a sample of truant youth. In addition, we examined the differential effects of BI-Y and BI-YP in reducing the truant youth’s marijuana use (Hypothesis 2), specifically, that truant youth receiving BI-YP services would exhibit lower post-intervention marijuana use, than youth receiving BI-Y services.
The results of our study provided support of the Hypothesis 1, but no support for Hypothesis 2. Overall, truant youth receiving BI services, experienced a significant reduction in marijuana use at 18 month follow-up (one-tailed test). Relatedly, truant youth receiving BI-Y services were significantly less likely to be involved in marijuana use at 18 month follow-up, than truant youth receiving STS. The effect sizes were in an appreciable range, Model 1(-0.509) and Model 2 (-0.941).
Given these effect sizes, it is also important to note that the cost of providing BI services is modest. We estimate a full-time brief interventionist can provide BI-Y services to approximately 70 youth per year, at a cost of about $500 per intervention service (assuming a $35,000 annual salary). It is important to note that a paraprofessional can be trained to deliver BI services. This is a relatively small cost, given the long term consequences discussed above, related to involvement in marijuana use—including potential justice system costs to affected youth, their families and society.
The overall Brief Intervention effect (BI-Y + BI-YP), specifically BI-Y services, on 18 month follow-up marijuana use may point to a delayed impact of the intervention, although more study is needed on this issue. This finding is consistent with other studies (e.g., Prado et al., 2007; Wolchik et al., 2002) that have found delayed effects of preventive interventions delivered in early adolescence. Our results are consistent with these cited studies in suggesting that the “effects of preventive interventions may only become apparent over a year post intervention. Such sleeper effects may be a function of developmental increases in base rates of the target behaviors”(Prado et al., 2007:923).
BI-YP services were not found to be effective in reducing the truant youth’s marijuana use, when compared to STS or BI-Y services. In fact, BI-YP youth experienced an increase in marijuana use, when compared to BI-Y youth (Model 4, effect size =0.852). There are several possible reasons for this result. First, it is likely that the parent/guardian session, focusing on monitoring and supervision issues, might have opened up several communication and relationship issues that could not be addressed during this one meeting. Several more parent/guardian sessions may have been needed to complete BI-YP services with the family. Relatedly, it may be important to include the youth in one or more of the parent/guardian sessions, in order to enhance communication skills and relations between parents and youth. In addition to increased monitoring and supervision, other important parenting skills introduced in the single BI parent session included development of family rules about substance use and practicing consistent discipline (Winters & Leitten, 2001). It is plausible that parents’ exercise of these principles within an already difficult and strained relationship with their child (and in the absence of additional BI sessions to foster communication and trust) may have contributed to the increased use of marijuana in this group. Additionally, when youth in this group emotionally process that parents are involved in the BI, they may misperceive their marijuana use to now be “out in the open,” and that parents have been made aware of their use. It is possible that an increase in marijuana use may occur because youth in this group may have mistakenly come to the realization that it is no longer necessary to hide this behavior.
Our finding that BI-YP was not associated with better outcomes than BI-Y with respect to marijuana use at long-term outcome (18-months) is relevant to consider in light of findings observed when this intervention was applied to moderate-to-mild drug abusing youth recruited from schools (Winters et al., 2012; in press). In those studies, at 6-month follow-up the BI-YP group was associated with superior outcome to the BI-Y (Winters et al., 2012), but at 12-months there were differences between the groups (Winters et al., in press). A significant mediating factor linked to the superior BI-YP effect at short-term outcome was greater utilization of community services following the intervention (Winters et al., 2012), a variable that may have exerted little or no effect at longer term outcome (Winters et al., in press). For the present study, we may have observed the same problem, that is, the BI-YP condition did not produce long-term counseling experiences for the youth and thus did yield better outcome.
As discussed earlier in this paper, rates of UA marijuana positives were sizable at each time point. Overall, marijuana positive rates were 46% at baseline, 36% at 3-month follow-up, 44% at 6-month follow-up, 43% at 12-month follow-up, and 49% at 18 month follow-up. These data highlight that marijuana use is a very significant issue among the truant youths we studied. Our results indicate Brief Intervention services may be effective in reducing their involvement with this substance 18 months post-intervention. This low cost, limited duration service holds promise of being of benefit to marijuana involved, truant youth in other jurisdictions.
We appreciate the youths may use drugs other than marijuana. Youths were also asked about their use of other drugs, including amphetamines, barbiturates, cocaine, opioids, hallucinogens, PCP, Club Drugs (e.g., Ecstasy), and inhalants. Relatively few youths reported using any of these drugs at any time point. Urine test results confirmed the very low, recent use of amphetamines, cocaine, and opiates (Appendix A). Appendix A also indicates that less than 10 percent of the youths reported 5 or more times use of one or more of any of the listed drugs. Barbiturates, followed by hallucinogens and cocaine, were the most frequently reported other drugs. Due to low frequencies of reported use of other drugs, and low UA positive rates for amphetamines, cocaine and opioids, these drugs were not in included in our analyses. As well, we found significant validity problems in the youths’ reported use of alcohol. Analysis showed that, at each time point, over 90% of youth found to be UA positive for marijuana but denied use of the drug, also denied the use of alcohol (Dembo et al., 2013--accepted with minor revisions).
There were several limitations to this study. First, there were limitations due to the nature of the sample, which consisted of truant youth picked up by law enforcement or placed in a diversion program. Hence, the results of the study may not generalize to truant youth who do not have such agency contact/involvement. Second, the truant youth were living in one geographical area. It would be important for future studies to evaluate the impact of Brief Intervention services among truant youth in other geographical areas.
We appreciate there are other domains of youth outcome that are important to examine, such as improvements in psychosocial functioning and school attendance. These will be the subject of other project studies. The results of this study provide promising indication that successful BI services, particular BI-Y services, may reduce the youths’ marijuana use, 18-months post intervention services, even after controlling for their background factors and previous marijuana use.
Supplementary Material
Table 3.
| Variables | Model 1: STS vs. BI-Y + BI-YP | Model 2: STS vs. BI-Y | ||||
|---|---|---|---|---|---|---|
| Estimate | S.E. | Est./S.E. | Estimate | S.E. | Est./S.E. | |
|
| ||||||
| Baseline Marijuana Use$1 | 1.161 | 0.745 | 1.559 | 0.438 | 0.878 | 0.499 |
| Baseline Marijuana Use$2 | 1.937** | 0.758 | 2.554 | 1.277 | 0.890 | 1.434 |
| Baseline Marijuana Use$3 | 2.745*** | 0.767 | 3.581 | 2.159* | 0.900 | 2.398 |
| 3-Month Follow-Up Marijuana Use$1 | 2.418* | 1.159 | 2.087 | 1.915 | 1.376 | 1.392 |
| 3-Month Follow-Up Marijuana Use$2 | 2.797* | 1.165 | 2.401 | 2.320 | 1.384 | 1.677 |
| 3-Month Follow-Up Marijuana Use$3 | 3.050** | 1.165 | 2.618 | 2.545 | 1.384 | 1.839 |
| 6-Month Follow-Up Marijuana Use$1 | 6.242*** | 1.321 | 4.725 | 5.831*** | 1.570 | 3.715 |
| 6-Month Follow-Up Marijuana Use$2 | 6.674*** | 1.324 | 5.040 | 6.353*** | 1.576 | 4.031 |
| 6-Month Follow-Up Marijuana Use$3 | 7.012*** | 1.324 | 5.296 | 6.602*** | 1.574 | 4.195 |
| 12-Month Follow-Up Marijuana Use$1 | 5.059** | 1.596 | 3.170 | 5.394** | 1.843 | 2.926 |
| 12-Month Follow-Up Marijuana Use$2 | 5.434*** | 1.604 | 3.387 | 5.867** | 1.855 | 3.163 |
| 12-Month Follow-Up Marijuana Use$3 | 5.941*** | 1.619 | 3.670 | 6.303*** | 1.871 | 3.370 |
| 18-Month Follow-Up Marijuana Use$1 | 2.974* | 1.417 | 2.099 | 2.436 | 1.720 | 1.416 |
| 18-Month Follow-Up Marijuana Use$2 | 3.321* | 1.424 | 2.333 | 2.754 | 1.729 | 1.592 |
| 18-Month Follow-Up Marijuana Use$3 | 3.536* | 1.428 | 2.476 | 3.011 | 1.734 | 1.736 |
| R2 | Model 1 | Model 2 | ||
| Estimate | Scale Factors | Estimate | Scale Factors | |
|
| ||||
| Baseline | 0.073 | 1.000 | 0.060 | 1.000 |
| 3-Month Follow-Up Marijuana Use | 0.389 | 0.809 | 0.299 | 0.848 |
| 6-Month Follow-Up Marijuana Use | 0.604 | 0.685 | 0.569 | 0.704 |
| 12-Month Follow-Up Marijuana Use | 0.639 | 0.633 | 0.610 | 0.651 |
| 18-Month Follow-Up Marijuana Use | 0.478 | 0.750 | 0.531 | 0.766 |
Note. Two-tailed p-values:
p < .05;
p < .01;
p < .001
Table 3.
| Variables | Model 3: STS vs. BI-YP | Model 4: BI-Y vs. BI-YP | ||||
|---|---|---|---|---|---|---|
| Estimate | S.E. | Est./S.E. | Estimate | S.E. | Est./S.E. | |
|
| ||||||
| 18-Month Follow-Up Marijuana Use ON | ||||||
| 12-Month Follow-Up Marijuana Use | 0.704*** | 0.153 | 4.609 | 0.482*** | 0.097 | 4.964 |
| Gender (1 = female) | -1.064* | 0.505 | -2.106 | |||
| African-American (1 = African-American) | 0.830++ | 0.424 | 1.959 | |||
| Intervention (1 = Intervention Condition[s]) | 0.012 | 0.390 | 0.032 | 0.790* | 0.323 | 2.448 |
| 12-Month Follow-Up Marijuana Use ON | ||||||
| 6-Month Follow-Up Marijuana Use | 0.816*** | 0.150 | 5.449 | 0.858*** | 0.119 | 7.214 |
| Intervention | 0.054 | 0.330 | 0.163 | 0.195 | 0.315 | 0.618 |
| 6-Month Follow-Up Marijuana Use ON | ||||||
| 3-Month Follow-Up Marijuana Use | 0.996*** | 0.164 | 6.065 | 0.762*** | 0.116 | 6.559 |
| Age | 0.319** | 0.102 | 3.139 | 0.298*** | 0.080 | 3.744 |
| Intervention | -0.030 | 0.349 | -0.085 | -0.050 | 0.278 | -0.178 |
| 3-Month Follow-Up Marijuana Use ON | ||||||
| Baseline Marijuana Use | 0.739*** | 0.126 | 5.877 | 0.755*** | 0.127 | 5.957 |
| Intervention | 0.307 | 0.296 | 1.038 | 0.417 | 0.275 | 1.515 |
| Gender × Intervention | -0.980* | 0.492 | -1.989 | -1.095* | 0.492 | -2.229 |
| Age | 0.111 | 0.095 | 1.170 | -0.026 | 0.085 | -0.303 |
| Baseline Marijuana Use ON | ||||||
| Age | 0.207*** | 0.065 | 3.181 | 0.173** | 0.063 | 2.748 |
| Gender | 0.050 | 0.265 | 0.189 | 0.080 | 0.251 | 0.319 |
| Family Income Level | 0.007 | 0.085 | 0.081 | 0.081 | 0.081 | 1.002 |
| Who Youth Lives With (1= Mother Only) | 0.440* | 0.203 | 2.166 | -0.114 | 0.193 | -0.590 |
| African-American (1 = African-American) | 0.126 | 0.240 | 0.526 | 0.404 | 0.233 | 1.732 |
| Hispanic (1 = Hispanic) | -0.427 | 0.226 | -1.889 | 0.146 | 0.223 | 0.654 |
| Family Experience of Stress/Trauma | 0.009 | 0.056 | 0.156 | -0.020 | 0.054 | -0.362 |
Note. Two-tailed p-values:
p < .05;
p < .01;
p < .001.
p=.05 for a two-tailed test.
Table 3.
| Variables | Model 3: STS vs. BI-YP | Model 4: BI-Y vs. BI-YP | ||||
|---|---|---|---|---|---|---|
| Estimate | S.E. | Est./S.E. | Estimate | S.E. | Est./S.E. | |
|
| ||||||
| Baseline Marijuana Use$1 | 1.790 | 0.952 | 1.881 | 1.361 | 0.903 | 1.507 |
| Baseline Marijuana Use$2 | 2.605** | 0.980 | 2.658 | 2.090* | 0.913 | 2.288 |
| Baseline Marijuana Use$3 | 3.374*** | 0.995 | 3.391 | 2.893** | 0.918 | 3.150 |
| 3-Month Follow-Up Marijuana Use$1 | 3.785* | 1.492 | 2.536 | 1.688 | 1.416 | 1.192 |
| 3-Month Follow-Up Marijuana Use$2 | 4.092** | 1.499 | 2.730 | 2.121 | 1.421 | 1.493 |
| 3-Month Follow-Up Marijuana Use$3 | 4.317** | 1.501 | 2.876 | 2.436 | 1.418 | 1.719 |
| 6-Month Follow-Up Marijuana Use$1 | 7.955*** | 1.870 | 4.254 | 5.530*** | 1.496 | 3.697 |
| 6-Month Follow-Up Marijuana Use$2 | 8.332*** | 1.872 | 4.450 | 5.942*** | 1.500 | 3.961 |
| 6-Month Follow-Up Marijuana Use$3 | 8.647*** | 1.882 | 4.595 | 6.405*** | 1.497 | 4.278 |
| 12-Month Follow-Up Marijuana Use$1 | 5.628** | 2.189 | 2.571 | 4.677* | 1.867 | 2.504 |
| 12-Month Follow-Up Marijuana Use$2 | 5.862** | 2.195 | 2.670 | 5.100** | 1.878 | 2.715 |
| 12-Month Follow-Up Marijuana Use$3 | 6.416** | 2.226 | 2.882 | 5.665** | 1.896 | 2.988 |
| 18-Month Follow-Up Marijuana Use$1 | 5.733* | 2.249 | 2.549 | 2.500 | 1.443 | 1.732 |
| 18-Month Follow-Up Marijuana Use$2 | 6.169** | 2.277 | 2.709 | 2.851* | 1.454 | 1.961 |
| 18-Month Follow-Up Marijuana Use$3 | 6.390** | 2.298 | 2.780 | 3.052* | 1.457 | 2.095 |
| R2 | Model 3 | Model 4 | ||
| Estimate | Scale Factors | Estimate | Scale Factors | |
|
| ||||
| Baseline | 0.146 | 1.000 | 0.085 | 1.000 |
| 3-Month Follow-Up Marijuana Use | 0.453 | 0.804 | 0.425 | 0.798 |
| 6-Month Follow-Up Marijuana Use | 0.695 | 0.628 | 0.553 | 0.723 |
| 12-Month Follow-Up Marijuana Use | 0.686 | 0.610 | 0.624 | 0.645 |
| 18-Month Follow-Up Marijuana Use | 0.695 | 0.655 | 0.449 | 0.801 |
Note. One-tailed p-values:
p < .05;
p < .01;
p < .001.
Acknowledgments
The research reported in this article was funded by National Institute on Drug Abuse (NIDA) Grant No. DA021561. We are grateful for NIDA’s support. We are also grateful for the collaboration and support of our work by the Tampa Police Department, the Hillsborough County Sheriff’s Office, the Hillsborough County Public Schools, the Agency for Community Treatment Services, and 13th Judicial Circuit, Juvenile Diversion Program. We also appreciate Ms. Kimberly Barrett’s assistance on this project between 2009 and 2011.
Contributor Information
Richard Dembo, University of South Florida, Department of Criminology, Tampa, FL 33620, Phone: (813) 931-3345, Fax: (813) 354-0740, rdembo@usf.edu
Rhissa Briones Robinson, Department of Criminology, University of South Florida, Tampa, FL 33620
James Schmeidler, Mt. Sinai School of Medicine, New York, NY 10029
Jennifer Wareham, Department of Criminal Justice, Wayne State University, Detroit, MI 48202
Rocío Ungaro, Department of Criminology, University of South Florida, Tampa, FL 33620.
Ken C. Winters, Department of Psychiatry, University of Minnesota, Minneapolis, MN 55454
Lora Karas, 13th Judicial Circuit, Tampa, FL 33602
Werner Wothke, American Councils for International Education, Washington, DC 20036
Steven Belenko, Department of Criminal Justice, Temple University, Philadelphia, PA 19122
References
- Baker ML, Sigmon JN, Nugent ME. Juvenile Justice Bulletin. Washington DC: U.S. Department of Justice, Office of Juvenile Justice Delinquency Prevention; 2001. Truancy reduction: Keeping students in school. [Google Scholar]
- Bernard ME, Joyce MR. Rational emotive therapy with children and adolescents: Theory, treatment strategies, preventative methods. New York: John Wiley; 1984. [Google Scholar]
- Breslin C, Li S, Sdao-Jarvie K, Tupker E, Ittig-Deland V. Brief treatment for young substance abusers: A pilot study in an addiction treatment setting. Psychology of Addictive Behaviors. 2002;16:10–16. [PubMed] [Google Scholar]
- Bridgeland J, Dilulio JJ, Jr, Morison KB. The silent epidemic: Perspectives of high school dropouts. The Bill & Melinda Gates Foundation; Seattle, WA: 2006. A report by Civic Enterprises in association with Peter D. Hart Research Associates for the Bill & Melinda Gates Foundation. [Google Scholar]
- Bry BH, Conboy C, Bigsay K. Decreasing adolescent drug use and school failure: Long-term effects of targeted family problem-solving training. Child & Family Behavior Therapy. 1986;8:43–59. [Google Scholar]
- Caldas SJ. Reexamination of input and process factor effects on public school achievement. Journal of Educational Research. 1993 Mar-Apr;86:206–214. [Google Scholar]
- Catalano RF, Hawkins JD, Wells EA, Miller J. Evaluation of effectiveness of adolescent drug abuse treatment, assessment of risks for relapse, and promising approaches for relapse prevention. The International Journal of Addictions. 1991;25:1085–1140. doi: 10.3109/10826089109081039. [DOI] [PubMed] [Google Scholar]
- Chilcoat HD, Anthony JC. Impact of parent monitoring on initiation of drug use through late childhood. Journal of the American Academy of Child and Adolescent Psychiatry. 1996;35:91–100. doi: 10.1097/00004583-199601000-00017. [DOI] [PubMed] [Google Scholar]
- Clark DB, Kirisci L, Tarter RE. Adolescent versus adult onset and development of substance use disorders in males. Drug and Alcohol Dependence. 1998;49:115–121. doi: 10.1016/s0376-8716(97)00154-3. [DOI] [PubMed] [Google Scholar]
- Clark DB, Winters KC. Measuring risks and outcomes in substance use disorders prevention research. Journal of Consulting and Clinical Psychology. 2002;70:1207–1223. doi: 10.1037//0022-006x.70.6.1207. [DOI] [PubMed] [Google Scholar]
- Colorado Department of Education. School by School Truancy Rates School Year: 2010-2011. 2011 Retrieved December, 2011 from http://www.cde.state.co.us/cdereval/truancystatistics.htm.
- D’Amico EJ, Miles JNV, Stern SA, Meredith LS. Brief motivational interviewing for teens at risk of substance use consequences: A randomized pilot study in a primary care clinic. Journal of Substance Abuse Treatment. 2008;35:53–61. doi: 10.1016/j.jsat.2007.08.008. [DOI] [PubMed] [Google Scholar]
- DeKalb J. Student truancy (ERIC Digest No 125) Eugene, OR: ERIC Clearinghouse on Educational Management; 1999. [Google Scholar]
- Dembo R, Briones Robinson R, Ungaro RA, Gulledge LM, Karas LM, Winters KC, Belenko S, Greenbaum PE. Emotional psychological and related problems among truant youths: An exploratory latent class analysis. Journal of Emotional and Behavioral Disorders. 2012;20:157–168. doi: 10.1177/1063426610396221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dembo R, Briones Robinson R, Barrett KL, Winters KC, Schmeidler J, Ungaro R, Karas LM, Belenko S, Gulledge LM. Mental health, substance use, and delinquency among truant youths in a brief intervention project: A longitudinal study. Journal of Emotional and Behavioral Disorders. doi: 10.1177/1063426611421006. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dembo R, Briones Robinson R, Barrett KL, Winters KC, Ungaro R, Karas L, Belenko S, Wareham J. The validity of truant youths’ marijuana use and its impact on alcohol use and sexual risk taking. Journal of Child and Adolescent Substance Abuse. doi: 10.1080/1067828X.2013.844089. under review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dembo R, Gulledge L. Truancy intervention programs: Challenges and innovations to implementation. Criminal Justice Policy Review. 2009;20:437–456. doi: 10.1177/0887403408327923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dembo R, Gulledge L, Briones Robinson R, Winters KC. Enrolling and engaging high-risk youths and families in community-based, brief intervention services. Journal of Child & Adolescent Substance Abuse. 2011;20:330–350. doi: 10.1080/1067828X.2011.598837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diebolt A, Herlache L. The school psychologist as a consultant in truancy prevention; Paper presented at the annual meeting of the National Association of School Psychologists; Dallas, Texas. 1991. [Google Scholar]
- Dougherty JW. Attending to attendance. Fastback 450, Bloomington, IN: Phi Delta Kappa Education Foundation; 1999. [Google Scholar]
- Dropout Nation. America’s truancy problem: L A County example. 2010 Retrieved March 14, 2012 from http://dropoutnation.net/
- Duarte R, Escario JJ. Alcohol use and truancy among Spanish adolescents: A count-data approach. Economics of Educational Review. 2005;25:179–187. [Google Scholar]
- D’Zurilla TJ, Goldfried MR. Problem-solving and behavior modification. Journal of Abnormal Psychology. 1971;78:107–126. doi: 10.1037/h0031360. [DOI] [PubMed] [Google Scholar]
- Egger HL, Costello EJ, Angold A. School refusal and psychiatric disorders: A community study. Journal of the American Academy of Child & Adolescent Psychiatry. 2003;42:797–807. doi: 10.1097/01.CHI.0000046865.56865.79. [DOI] [PubMed] [Google Scholar]
- Freedman B. Equipoise and the ethics of clinical research. New England Journal of Medicine. 1987;317:141–145. doi: 10.1056/NEJM198707163170304. [DOI] [PubMed] [Google Scholar]
- Fromme K, Marlatt GA, Baer JS, Kivlahan DR. The Alcohol Skills Training Program: A group intervention for young adult drinkers. Journal of Substance Abuse Treatment. 1994;11:143–154. doi: 10.1016/0740-5472(94)90032-9. [DOI] [PubMed] [Google Scholar]
- Garry EM. Juvenile Justice Bulletin. Vol. 76. Washington DC: U.S. Department of Justice, Office of Juvenile Justice Delinquency Prevention; 2001. Truancy, first step in a lifetime of problems. [Google Scholar]
- Gonzalez JE, Nelson JR, Gutkin TB, Saunders A, Galloway A, Shwery CS. Rational Emotive Therapy with children and adolescents: A meta-analysis. Journal of Emotional and Behavioral Disorders. 2004;12:222–235. [Google Scholar]
- Gorman-Smith D, Tolan PH, Loeber R, Henry D. Relation of family problems to patterns of delinquent involvement among urban youth. Journal of Abnormal Child Psychology. 1998;26:319–333. doi: 10.1023/a:1021995621302. [DOI] [PubMed] [Google Scholar]
- Hallfors D, Vevea JL, Iritani B, Cho H, Khatapoush S, Saxe L. Truancy, grade point average, and sexual activity: A meta-analysis of risk indicators for youth substance use. Journal of School Health. 2002;72:205–211. doi: 10.1111/j.1746-1561.2002.tb06548.x. [DOI] [PubMed] [Google Scholar]
- Henry KL, Huizinga DH. Truancy’s effect on the onset of drug use among urban adolescents placed at risk. Journal of Adolescent Health. 2007;40:358.e9–358.e17. doi: 10.1016/j.jadohealth.2006.11.138. [DOI] [PubMed] [Google Scholar]
- Henry KL, Thornberry TP. Truancy and escalation of substance use during adolescence. Journal of Studies on Alcohol and Drugs. 2010;71:115–124. doi: 10.15288/jsad.2010.71.115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the future national results on adolescent drug use: Overview of key findings, 2003. Ann Arbor, MI: Institute for Social Research, University of Michigan; 2004. [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the future national results on adolescent drug use: Overview of key findings, 2012. Ann Arbor, MI: Institute for Social Research, University of Michigan; 2013. [Google Scholar]
- Joreskog KG, Sorbom D. LISREL 8: Structural equation modeling with the SIMPLIS command language. Chicago: Scientific Software International; 1993. [Google Scholar]
- Kearney CA, Silverman WK. Family environment of youngsters with school refusal behavior: A synopsis with implications for assessment and treatment. American Journal of Family Therapy. 1995;23:59–72. [Google Scholar]
- Lamdin DJ. Evidence of student attendance as an independent variable in education production functions. Journal of Educational Research. 1996 Jan-Feb;89:155–162. [Google Scholar]
- Meier MH, Caspi A, Ambler A, Harrington H, Houts R, Keefe RSE, McDonald K, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proceedings of the National Academy of Sciences. 2012;109(40) doi: 10.1073/pnas.1206820109. PNAS Early Edition report. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller WR. Motivational Interviewing with problem drinkers. Behavioural Psychotherapy. 1983;11:147–172. [Google Scholar]
- Miller WR, Rollnick S. Motivational Interviewing: Preparing people to change addictive behavior. New York: Guilford Press; 1991. [Google Scholar]
- Muthén BO, Asparouhov T. Latent variable analysis with categorical outcomes: Multiple-Group and Growth Modeling in Mplus. Los Angeles, CA: Muthén & Muthén; 2002. Mplus Web Notes: No. 4. [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide, version 7. Los Angeles, CA: Muthén & Muthén; 1998-2012. [Google Scholar]
- National Center for School Engagement. Quantifying school engagement: Research report. Denver, CO: National Center for School Engagement; 2006. [Google Scholar]
- Prado G, Pantin H, Briones E, Schwartz SJ, Feaster D, Huang S, Sullivan S, Tapia MI, Sabillon E, Lopez B, Szapocznik José. A randomized controlled trial of a parent-centered intervention in preventing substance use and HIV risk behaviors in Hispanic adolescents. Journal of Consulting and Clinical Psychology. 2007;75(6):914–926. doi: 10.1037/0022-006X.75.6.914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roebuck MC, French MT, Dennis ML. Adolescent marijuana use and school attendance. Economics of Education Review. 2004;23:133–141. [Google Scholar]
- Siziya S, Muula AS, Rudatsikira E. Prevalence and correlates of truancy among adolescents in Swaziland: Findings from the global school-based health survey. Child and Adolescent Psychiatry and Mental Health. 2007;1:15–22. doi: 10.1186/1753-2000-1-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soldz S, Huyser DJ, Dorsey E. The cigar as a drug delivery device: Youth use of blunts. Addiction. 2003;98:1379–1386. doi: 10.1046/j.1360-0443.2003.00492.x. [DOI] [PubMed] [Google Scholar]
- Stein LAR, Clair M, Lebeau R, Colby SM, Barnett NP, Golembeske C, Monti PM. Motivational interviewing to reduce substance-related consequences: Effects for incarcerated adolescents with depressed mood. Drug and Alcohol Dependence. 2011;118:475–478. doi: 10.1016/j.drugalcdep.2011.03.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tait RJ, Hulse GK. A systematic review of the effectiveness of brief interventions with substance using adolescents by type of drug. Drug and Alcohol Review. 2003;22:337–346. doi: 10.1080/0959523031000154481. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Education. (n.d.) The Challenge Newsletter. no. 2. Vol. 15. Washington, D.C.: Office of Safe and Drug-Free Schools; Truancy numbers hard to count. [Google Scholar]
- Williams RJ, Chang SY Addiction Centre Adolescent Research Group. A comprehensive and comparative review of adolescent substance abuse treatment outcome. Clinical Psychology, Science, and Practice. 2000;7:138–166. [Google Scholar]
- Winters KC. Development of an adolescent alcohol and other drug abuse screening scale: Personal Experience Screening Questionnaire. Addictive Behaviors. 1992;17:479–490. doi: 10.1016/0306-4603(92)90008-j. [DOI] [PubMed] [Google Scholar]
- Winters KC. Treatment of adolescents with substance use disorders. Treatment Improvement Protocol (TIP) Series 32. 1999 http://www.athealth.com/practitioner/ceduc/health_tip32b.html.
- Winters KC, Fahnhorst T, Botzet A, Lee S, Lalone B. Brief intervention for drug abusing adolescents in a school setting: Outcomes and mediating factors. Journal of Substance Abuse Treatment. 2012;42:279–288. doi: 10.1016/j.jsat.2011.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winters KC, Henly GA. Adolescent diagnostic interview schedule and manual. Los Angeles: Western Psychological Services; 1993. [Google Scholar]
- Winters KC, Lee S, Botzet A, Fahnhorst T, Nicholson A. One-year outcomes of a brief intervention for drug abusing adolescents. Psychology of Addictive Behaviors. doi: 10.1037/a0035041. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winters KC, Leitten W. Brief intervention manual. Minneapolis: University of Minnesota; 2001. [Google Scholar]
- Winters KC, Leitten W. Brief intervention for drug-abusing adolescents in a school setting. Psychology of Addictive Behaviors. 2007;21:249–254. doi: 10.1037/0893-164X.21.2.249. [DOI] [PubMed] [Google Scholar]
- Winters KC, Stinchfield RD. Adolescent Diagnostic Interview-Parent. Minneapolis, MN: University of Minnesota; 2003. [Google Scholar]
- Wolchik SA, Sandler IN, Millsap RE, Plummer BA, Greene SM, Anderson ER, Dawson-McClure Spring R, Hipke K, Haine R. Six-year follow-up of preventive interventions for children of divorce: Randomized controlled trial. Journal of American Medical Association. 2002;288(15):1874–1881. doi: 10.1001/jama.288.15.1874. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.