

Abstract
Background
Sedentary behaviors have been directly associated with all‐cause mortality. However, little is known about different types of sedentary behaviors in relation to overall mortality. Our objective was to assess the association between different sedentary behaviors and all‐cause mortality.
Methods and Results
In this prospective, dynamic cohort study (the SUN Project) 13 284 Spanish university graduates with a mean age of 37 years were followed‐up for a median of 8.2 years. Television, computer, and driving time were assessed at baseline. Poisson regression models were fitted to examine the association between each sedentary behavior and total mortality. All‐cause mortality incidence rate ratios (IRRs) per 2 hours per day were 1.40 (95% confidence interval (CI): 1.06 to 1.84) for television viewing, 0.96 (95% CI: 0.79 to 1.18) for computer use, and 1.14 (95% CI: 0.90 to 1.44) for driving, after adjustment for age, sex, smoking status, total energy intake, Mediterranean diet adherence, body mass index, and physical activity. The risk of mortality was twofold higher for participants reporting ≥3 h/day of television viewing than for those reporting <1 h/d (IRR: 2.04 [95% CI 1.16 to 3.57]).
Conclusions
Television viewing was directly associated with all‐cause mortality. However, computer use and time spent driving were not significantly associated with higher mortality. Further cohort studies and trials designed to assess whether reductions in television viewing are able to reduce mortality are warranted. The lack of association between computer use or time spent driving and mortality needs further confirmation.
Keywords: death, prospective cohort study, sedentary behavior, sedentary time, sitting time
Introduction
The benefits of a physically active lifestyle are well known.1–2 Epidemiologic research has traditionally focused on the effects of physical activity on morbidity and mortality.3 Early research conceptualized the absence of moderate‐to‐vigorous physical activities as a “sedentary lifestyle”. However, sedentary lifestyles deserve special and separate consideration because too much time spent sitting down is distinct from too little physical activity. In fact, high levels of sedentary behaviors can coexist with high levels of physical activity.4
Television viewing5 and sedentary time6 were found in 2 different meta‐analyses to be associated with an increased risk of diabetes, cardiovascular disease, and total mortality. Several studies reported that sitting time during leisure,7 total sitting time,8 or television viewing9 were associated with increased mortality, regardless of physical activity levels. Moreover, Matthews et al10 found that television viewing and overall sitting time were positively associated with all‐cause mortality after adjustment for physical activity.
Adults in the United States spend more than half of their waking hours in sedentary pursuits,11 such as television viewing, computer use, or driving.12 Altenburg et al13 found among Dutch adults (18 to 28 years) that television viewing, but not computer use, was directly associated with triglycerides levels and insulin concentrations. Pinto Pereira et al14 reported in British adults (44 to 45 years) that television viewing was adversely associated with biomarkers for cardiovascular disease. However, sitting time at work showed no association in women and only a weak association in men.
Several studies5–6,15 have addressed the association between television viewing (or total sedentary time) and mortality. However, few studies have assessed this association independently from physical activity levels. Thus, our objective was to assess the association between different types of sedentary behaviors (television viewing, computer use, and time driving) and all‐cause mortality in a prospective cohort study of Spanish university graduates.
Methods
Study Population
The design, methods, and objectives of the SUN Project (“Seguimiento Universidad de Navarra”, University of Navarra follow‐up) have been described previously.16 Briefly, the SUN Project is a multi‐purpose prospective cohort study designed to assess associations of diet or lifestyle with the incidence of several diseases and mortality. Information is collected through self‐administered questionnaires sent by mail every 2 years. The recruitment of participants, all of them university graduates, started in December 1999. The design is that of a dynamic cohort so the recruitment is permanently open.
Up to December 2012, the project had enrolled 21 593 participants. Among them, 20 572 completed the baseline questionnaire before March 2010 and were eligible for longitudinal analyses to warrant a minimum follow‐up time of 2 years. Participants who reported diabetes, cardiovascular disease, or cancer at baseline (n=1202), those with missing data for television viewing, computer use, or driving (n=4980), and participants lost to follow‐up (n=1106) were excluded from the present analyses. Thus, our final sample included 13 284 participants.
The study was approved by the Institutional Review Board of the University of Navarra. Voluntary response to the initial self‐administered questionnaire was considered to imply informed consent.
Sitting Time Assessment
The baseline questionnaire included items to assess television viewing, computer use or driving. Each of these 3 items was quantified in 12 categories (ranging from never to >9 h/d). These exposures were measured separately for weekdays and weekends. Time spent during weekdays was multiplied by 5 and the time spent during weekends by 2, and results were summed and divided by 7 to calculate the participants' total time per day. The validation study of this questionnaire found that the Spearman correlation coefficient between the energy expenditure estimated through the ratio sedentary lifestyle:physical activity in the questionnaire and that obtained by an objective method (triaxial accelerometer) was −0.578 (95% CI −0.754 to −0.325).17
Outcome Assessment
Our primary end point was death from any cause. If participants did not answer any of the 5 repeated mailings with the follow‐up questionnaires, they were contacted by e‐mail or telephone. Most deaths (>85%) were identified from reports by the next of kin, work associates, and postal authorities. The National Death Index was checked every 6 months to identify deceased cohort members. National Death Index is a responsibility of the National Institute of Statistics of the Spanish Government. It is a central index that collects information of any death registered in Spain. Taking into account all these sources of information, we considered that follow‐up ascertainment for the deceased participants was complete.
Assessment of Covariates
The baseline questionnaire inquired information about medical history, lifestyle, sociodemographic factors, and anthropometric measurements. Physical activity was ascertained at baseline through a 17‐item questionnaire.17 Time spent in each activity in hours per week was multiplied by its typical energy expenditure, expressed in metabolic equivalent tasks (METs), then summed over all activities to yield a METs‐h/wk score for each participant.18 This score correlated with energy expenditure measured by a triaxial accelerometer in a validation study (Spearman correlation coefficient 0.507 (95% CI 0.232 to 0.707).17 Regarding smoking habits, participants were classified as nonsmokers, quitters, or current smokers. Dietary habits at baseline were assessed using a 136‐item semiquantitative food‐frequency questionnaire previously validated in Spain.19 Adherence to the Mediterranean dietary pattern was appraised combining 9 items (fruits and nuts, vegetables, fish, legumes, cereals, dairy products, meat, and meat products, alcohol, and the ratio monounsaturated fatty acids/saturated fatty acids).20 Self‐reported weight and height, and body mass index (BMI) calculated from them, were previously validated in a subsample of this cohort.21
Statistical Analysis
We summarized continuous variables by their mean and standard deviation (SD), and categorical variables using percentages. To estimate incidence rate ratios (IRRs) and their 95% confidence intervals (CI), across increasing categories of sitting time (or other sedentary activities) and mortality, we fitted Poisson regression models with robust standard errors. For all analyses, we considered participants with the lowest exposure time at baseline as the reference category. We conducted tests of linear trend across increasing categories of sedentary activities by assigning medians for the time spent in each activity within each category and treating this variable as a continuous one. Poisson regression models were also fitted to examine the association between each type of sedentary behavior as a continuous variable and total mortality. As a sensitivity analysis we repeated these models using Cox proportional hazards regression.
We fitted a crude univariable model, an age‐ and sex‐adjusted model and a multivariable model adjusted also for, smoking, total energy intake (kcal/d), Mediterranean diet adherence, baseline BMI (kg/m2) and leisure‐time physical activity (METs‐h/wk). To assess correlations of continuous variables we calculated Pearson correlation coefficients. Deaths occurring over time were described using Nelson‐Aalen survival curves. We used inverse probability weighting to adjust the Nelson‐Aalen curves for potential confounders.
All P values were 2 tailed, and significance was set at P<0.05.
Results
During a median of 8.2 years of follow‐up we registered 97 deaths from all causes in this young and healthy cohort (the expected number of deaths would be 128 in a sample of the general Spanish population with the same size, sex, and age distribution). Table 1 shows descriptive statistics according to the average number of daily hours of television viewing, computer use and time spent driving. Of the 13 284 participants, 61.6% were women. Mean age was 37 years. Participants spent at baseline a mean (SD) of 1.6 (1.3) h/d watching television, 2.1 (2.1) h/d using computers and 0.9 (1.2) h/d driving. The correlation coefficient between the time spent in television viewing and using a computer was 0.07 (95% CI: 0.05 to 0.08); it was 0.20 (95% CI: 0.18 to 0.21) between television viewing and driving; and it was 0.12 (95% CI: 0.10 to 0.14) between using a computer and driving. Correlations between physical activity and television viewing, using a computer and driving were −0.04 (95% CI: −0.06 to −0.03), 0.003 (95% CI: −0.01 to 0.02) and 0.01 (95% CI: −0.01 to 0.03), respectively.
Table 1.
Baseline Characteristics of Participants According to Television Viewing, Computer Use and Driving at Baseline: Figures are Means and Standard Deviations (SD) Unless Otherwise Stated, The SUN Project 1999–2010
| Television | Computer | Driving | ||||
|---|---|---|---|---|---|---|
| <1 h/d | ≥3 h/d | <1 h/d | ≥3 h/d | 0 h/d | ≥2 h/d | |
| N | 4539 | 1631 | 5902 | 3959 | 1908 | 1277 |
| Age, y | 37.1 (11.0) | 35.8 (12.1) | 37.2 (11.9) | 35.5 (9.6) | 32.1 (11.7) | 36.4 (10.7) |
| Female, % | 61.6 | 67.0 | 71.0 | 54.7 | 82.3 | 53.5 |
| BMI, kg/m2 | 23.1 (3.3) | 23.6 (3.6) | 23.1 (3.5) | 23.5 (3.5) | 22.2 (3.2) | 24.0 (3.6) |
| Physical activity, METs‐h/wk | 22.0 (23.8) | 19.1 (21.7) | 20.6 (22.2) | 20.5 (22.3) | 20.0 (22.3) | 21.9 (25.5) |
| Total energy intake, kcal/d | 2543 (890) | 2611 (1129) | 2555 (957) | 2545 (919) | 2635 (1018) | 2634 (923) |
| Mediterranean diet (0 to 9 score) | 4.2 (1.8) | 4.1 (1.7) | 4.3 (1.8) | 4.1 (1.8) | 4.2 (1.8) | 4.2 (1.8) |
| Smoking | ||||||
| Never, % | 52.8 | 45.9 | 48.3 | 50.3 | 56.8 | 46.8 |
| Current, % | 20.0 | 27.7 | 23.8 | 24.0 | 24.8 | 26.4 |
| Television viewing, h/d | 0.5 (0.2) | 4.1 (1.5) | 1.6 (1.2) | 1.7 (1.5) | 1.8 (1.5) | 2.2 (2.1) |
| Computer use, h/d | 2.0 (2.1) | 2.3 (2.3) | 0.3 (0.3) | 5.0 (1.3) | 2.0 (2.3) | 2.6 (2.5) |
| Car driving, h/d | 0.8 (1.2) | 1.3 (2.0) | 0.8 (1.1) | 1.1 (1.5) | 0 (0) | 3.7 (2.2) |
BMI indicates body mass index; MET, metabolic equivalent task.
Television viewing time was positively associated with all‐cause mortality after adjustment for age, sex, smoking, total energy intake, Mediterranean diet adherence, BMI, computer use, and time spent driving (Figure 1). Participants reporting ≥3 h/d of television viewing had a twofold higher risk of mortality than those reporting <1 h/d (IRR 2.04; 95% CI: 1.16 to 3.57) (Table 2). When television viewing was analyzed as a continuous variable, the IRR per each additional 2 h/d of television watching was 1.40 (95% CI: 1.06 to 1.84). The time spent using a computer or driving were not significantly associated with mortality (Table 2). When the time spent using a computer and driving were analyzed as continuous variables, the IRRs per each additional 2 h/d were 0.96 (95% CI: 0.79 to 1.18) and 1.14 (95% CI: 0.90 to 1.44), respectively. A higher amount of total sedentary behaviors (the sum of television viewing, computer use, and driving) was directly associated with total mortality after multivariable adjustment (Table 3). When total sedentary behavior was analyzed as a continuous variable, the IRR per each additional 2 h/d of exposure was 1.17 (95% CI: 1.03 to 1.33)]. There were no significant interactions between television viewing (continuous) and sex, baseline body mass index, or physical activity. (Figure 2).
Figure 1.
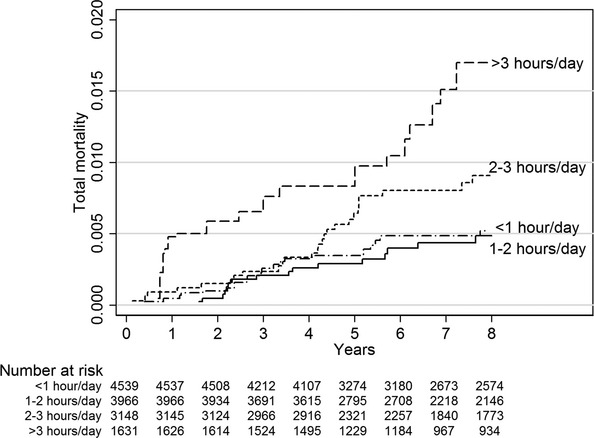
Nelson‐Aalen estimates of total mortality according to categories of baseline television viewing. Adjusted for age (continuous), sex, smoking history (never, current, quit), total energy intake (continuous), Mediterranean diet adherence (continuous), baseline body mass index (continuous), physical activity (quartiles), computer use (continuous), time driving (continuous), using inverse probability weighting.
Table 2.
Association Between Time Spent in Television Viewing, Computer Use and Driving and Total Mortality, The SUN Project 1999–2010
| Television Viewing | <1 h/d | 1 to 2 h/d | 2 to 3 h/d | ≥3 h/d | P Trend |
|---|---|---|---|---|---|
| N | 4539 | 3966 | 3148 | 1631 | |
| Unadjusted cumulative incidence of deaths, % | 0.57 | 0.55 | 0.86 | 1.35 | |
| Age‐, sex‐ adjusted | 1 (Ref.) | 1.02 (0.58 to 1.77) | 1.47 (0.86 to 2.48) | 2.31 (1.34 to 4.00) | 0.002 |
| Multivariable‐adjusted* | 1 (Ref.) | 1.01 (0.57 to 1.78) | 1.36 (0.80 to 2.30) | 2.01 (1.16 to 3.50) | 0.011 |
| Multivariable‐adjusted* | 1 (Ref.) | 1.05 (0.59 to 1.87) | 1.44 (0.85 to 2.43) | 2.04 (1.16 to 3.57) | 0.008 |
| Computer Use | <1 h/d | 1 to 2 h/d | 2 to 3 h/d | ≥3 h/d | P Trend |
|---|---|---|---|---|---|
| N | 5902 | 1696 | 1727 | 3959 | |
| Unadjusted cumulative incidence of deaths, % | 0.83 | 0.88 | 0.52 | 0.73 | |
| Age‐, sex‐ adjusted | 1 (Ref.) | 1.11 (0.62 to 1.98) | 0.69 (0.34 to 1.41) | 1.10 (0.68 to 1.78) | 0.94 |
| Multivariable‐adjusted* | 1 (Ref.) | 1.13 (0.63 to 2.00) | 0.72 (0.35 to 1.47) | 1.12 (0.68 to 1.82) | 0.97 |
| Multivariable‐adjusted* | 1 (Ref.) | 1.13 (0.64 to 2.02) | 0.73 (0.36 to 1.48) | 1.05 (0.64 to 1.72) | 0.92 |
| Time Driving | 0 h/d | 0 to 1 h/d | 1 to 2 h/d | ≥2 h/d | P Trend |
|---|---|---|---|---|---|
| N | 1908 | 7467 | 2632 | 1277 | |
| Unadjusted cumulative incidence of deaths, % | 0.79 | 0.60 | 0.87 | 1.10 | |
| Age‐, sex‐ adjusted | 1 (Ref.) | 0.50 (0.27 to 0.92) | 0.70 (0.35 to 1.42) | 0.94 (0.44 to 1.98) | 0.20 |
| Multivariable‐adjusted* | 1 (Ref.) | 0.56 (0.31 to 1.04) | 0.79 (0.39 to 1.58) | 1.02 (0.48 to 2.15) | 0.19 |
| Multivariable‐adjusted* | 1 (Ref.) | 0.61 (0.33 to 1.12) | 0.83 (0.41 to 1.70) | 0.93 (0.43 to 2.01) | 0.39 |
Values are incidence rate ratios; 95% confidence intervals in parenthesis.
Adjusted for age (continuous), sex, smoking history (never, current, quit), total energy intake (continuous), Mediterranean diet adherence (continuous).
Adjusted for age (continuous), sex, smoking history (never, current, quit), total energy intake, Mediterranean diet adherence (continuous), baseline body mass index (continuous), physical activity (quartiles), computer use (continuous) and driving (continuous).
Adjusted for age (continuous), sex, smoking history (never, current, quit), total energy intake, Mediterranean diet adherence (continuous), baseline body mass index (continuous), physical activity (quartiles), television viewing (continuous) and driving (continuous).
Adjusted for age (continuous), sex, smoking history (never, current, quit), total energy intake (continuous), Mediterranean diet adherence (continuous), baseline body mass index (continuous), physical activity (quartiles), television viewing (continuous) and computer use (continuous).
Table 3.
Association Between Total Time Sitting Down (Television Viewing+Computer Use+Driving) and Total Mortality, The SUN Project 1999–2010
| Time Sitting | <2 h/d | 2 to 4 h/d | 4 to 6 h/d | ≥6 h/d | P Trend |
|---|---|---|---|---|---|
| N | 2347 | 4185 | 3066 | 3686 | |
| Unadjusted cumulative incidence of deaths, % | 0.47 | 0.69 | 0.98 | 0.73 | |
| Age‐, sex‐ adjusted | 1 (Ref.) | 1.44 (0.74 to 2.81) | 2.16 (1.11 to 4.21) | 2.18 (1.11 to 4.28) | 0.009 |
| Multivariable‐adjusted* | 1 (Ref.) | 1.45 (0.75 to 2.82) | 2.04 (1.05 to 3.96) | 2.06 (1.05 to 4.07) | 0.023 |
| Multivariable‐adjusted* | 1 (Ref.) | 1.50 (0.77 to 2.91) | 2.13 (1.09 to 4.14) | 2.11 (1.07 to 4.15) | 0.021 |
Values are incidence rate ratios; 95% confidence intervals in parenthesis.
Adjusted for age (continuous), sex, smoking history (never, current, quit), total energy intake (continuous), Mediterranean diet adherence (continuous).
Adjusted for age (continuous), sex, smoking history (never, current, quit), total energy intake (continuous), Mediterranean diet adherence (continuous), baseline body mass index (continuous), physical activity (quartiles).
Figure 2.
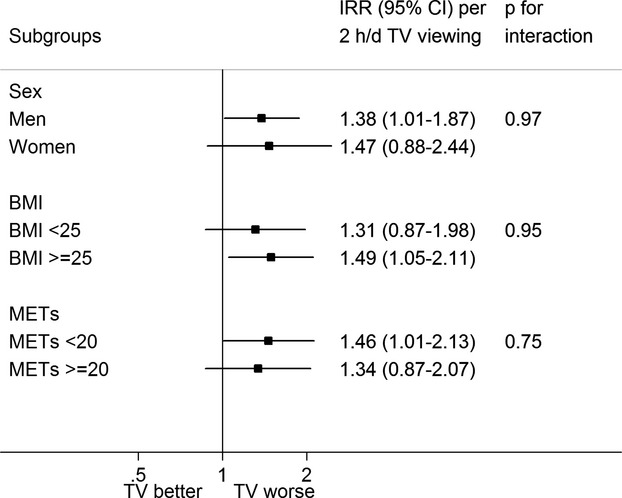
Results of subgroup analyses of television viewing and mortality. Adjusted incidence risk ratios per 2 hours of TV (television) viewing per day for mortality within specific subgroups. Squares denote incidence risk ratios; horizontal lines represent 95% confidence intervals. Incidence risk ratios were adjusted for age (continuous), sex, smoking history (never, current, quit), total energy intake (continuous), Mediterranean diet adherence (continuous), baseline body mass index (continuous), physical activity (continuous), computer use (continuous), time driving (continuous). BMI indicates body mass index; IRR, incidence risk ratio; MET, metabolic equivalent task; TV, television.
During 8.2 years of follow‐up, 19 deaths occurred due to cardiovascular disease, 46 occurred due to cancer, and 32 deceases were noncardiovascular/noncancer deaths. The IRRs for each additional 2 h/d of television viewing were 1.44 (95% CI: 0.87 to 2.41) for cardiovascular mortality, 1.21 (95% CI: 0.73 to 2.00) for cancer mortality and 1.55 (95% CI: 0.96 to 2.53) for noncardiovascular/noncancer mortality, after adjusting for age, sex, smoking, total energy intake, Mediterranean diet adherence, BMI, computer use, and time spent driving.
To check for reverse causality, we repeated the analyses after excluding deaths occurring in the first 3 years of follow‐up (35 deaths excluded). The multivariable‐adjusted IRRs for all‐cause mortality across categories of television viewing were 1.16 (95% CI: 0.56 to 2.39), 1.75 (95% CI: 0.91 to 3.35), and 2.38 (95% CI: 1.19 to 4.74) for 1 to 2 h/d, 2 to 3 h/d, and ≥3 h/d, respectively, with <1 h/d as the reference category (P for linear trend=0.006). When television viewing was introduced as a continuous variable the multivariable‐adjusted IRR per each additional 2 h/d was 1.48 (95% CI: 1.08 to 2.02).
Finally, as a sensitivity analyses we repeated the analysis further adjusting for snacking and consumption of sugar‐sweetened beverages. The all‐cause mortality IRRs for television viewing were of 1.09 (95% CI: 0.61 to 1.95), 1.45 (95% CI: 0.84 to 2.50), and 2.19 (95% CI: 1.23 to 3.91) for 1 to 2 h/d, 2 to 3 h/d and ≥3 h/d, respectively, with <1 h/d as the reference category (P for linear trend=0.006). When television viewing was introduced as a continuous variable the IRR per each additional 2 h/d of exposure was 1.46 (95% CI: 1.10 to 1.93).
Discussion
In this prospective cohort study we assessed different types of sedentary behaviors and found that television viewing and total sitting time were associated with higher risks of all‐cause mortality after adjusting for physical activity and other potential confounders. These 2 associations showed a direct monotonic dose‐response linear trend with mortality. We did not find any association between computer use or time spent driving and all‐cause mortality.
Because television viewing is likely to be associated with snacking and consumption of sugar‐sweetened beverages,22 a possible explanation for the association that we have found could be a difference in energy intake during television viewing. However, the associations between television viewing and mortality were adjusted for total caloric intake and hardly changed after adjustment for snacking and consumption of sugar‐sweetened beverages. A second alternative non‐causal explanation for our results might be reverse causation, because patients with a chronic disease may continue watching television but stop using computers or driving. However, there are several reasons to think that reverse causation is not a major confounder in this cohort. First, this is a young and basically healthy cohort. Besides, participants with baseline diabetes, cardiovascular disease or cancer were excluded from all the analyses. Finally, when deaths occurring in the first 3 years of follow‐up (deaths that were more likely to be related to a latent disease at baseline) were excluded, the results did not significantly change. A third possible explanation for the differences in mortality found between television viewing and computer use is that computer use has increased in Spain during the last years,23 and for this reason baseline questionnaires may not reflect the total “average” exposure. This change in computer use may have produced a misclassification of exposure. Though possible, it is however very unlikely that such a misclassification may explain the present results. Furthermore, television viewing hardly has changed in Spain during the years when the follow‐up of this cohort took place.23 A fourth explanation for these results could be a difference in energy expenditure. Among the 3 activities that we assessed, energy expenditure during driving may be higher than during computer use or television viewing.18 But also using the computer may lead to a higher energy expenditure than television viewing, because computer use may require some muscle activity. In this way our results are consistent with those reporting that low‐intensity non‐exercise activities are inversely associated with mortality24–25 and beneficially associated with cardiometabolic risk markers.26 Finally, although we adjusted for a wide array of covariates, residual confounding might also be a possible explanation for our results, as it can be always the case in observational studies. However, a randomized trial probably will be never conducted to assess this association, due to problems of ethics and feasibility.
The different associations with mortality found for television viewing, computer use or driving may be explained by differential effects of these activities on cardiometabolic risk factors. A recent study conducted among Dutch adults13 reported that television viewing, but not computer use, was associated with detrimental changes in biomarkers. Another study27 conducted in an Asian population reported that television screen time, but not computer use or reading time, was associated with worse cardio‐metabolic biomarkers. Hu et al28 reported among US women (30 to 55 years) that sitting at work or away from home or while driving, and especially television viewing, were significantly associated with increased risk of obesity and type 2 diabetes. Other time spent sitting at home (eg, reading, meal times, at desk) was significantly associated with increased risk of type 2 diabetes, but not with obesity. Matthews et al10 found among US adults (50 to 71 years) that television viewing had a stronger association with mortality than overall sitting time. However, the association between different sedentary behaviors and all‐cause mortality was not assessed in these previous studies.
Our findings confirm the association between television viewing and mortality found in a meta‐analysis5 of 3 prospective studies9,29–30 with a pooled relative risk of 1.13 (95% CI: 1.07 to 1.18) per 2 additional h/d of television viewing. Another meta‐analysis, of 8 studies, addressed the association between sedentary time and death,6 observing a pooled HR of 1.49 (95% CI: 1.14 to 2.03) for the highest versus the lowest exposure. The 3 studies included in the first meta‐analysis were also included in the second one. With a single exception8 (mean age 42 years), all studies included in these meta‐analyses had older participants (age>50 years). Thus, a novelty of our findings is to support also a direct association between television viewing and mortality in a relatively young cohort. There are fewer studies about computer use; 2 recent studies29,31 assessed the combined effect of television viewing and computer use on mortality. Only 1 of them29 reported a significant direct association. Warren et al32 found that men riding in a car had higher rates of cardiovascular mortality, although these results were not comparable with ours because driving a car expends more energy than riding in a car.18 The classic and well‐known study of Morris et al33–34 reported that London bus drivers were more likely than bus conductors to develop coronary heart disease, however in this case drivers were more sedentary than conductors and exposure to driving was longer than in our cohort.
Since our analyses were adjusted for leisure‐time physical activity, our findings suggest that not only the promotion of physical activity but also the reduction in sedentary activities (especially television viewing) is a priority for the prevention of premature mortality. Other authors have also reported that prolonged sitting is a risk factor for all‐cause mortality, independently of physical activity.7–10,30,35 In this cohort, the correlation between physical activity and television viewing was minimal (r=−0.04) and there was no correlation between physical activity and computer use or time spent driving. This very weak correlation found between television viewing and physical activity is consistent with previous studies.7,9,28 The metabolic pathways linking prolonged sitting times with clinical disease are unclear. Studies conducted in animal models have demonstrated a reduction in lipoprotein lipase activity.36–37 There is evidence of increases in C‐reactive protein,29 and altered carbohydrate metabolism in humans associated with sedentary lifestyles.37
A strength of our study is the detailed assessment of specific sedentary behaviors.38 Other strengths include its prospective design and the ability to carefully evaluate reverse causality and to adjust for several potential confounders. Besides, our cohort has a high retention rate. The main limitation is the use of self‐reported information on exposure. All participants are university graduates and this fact contributes to a higher quality of their self‐reported information. Furthermore, our questionnaire of physical activity and sedentary lifestyle had been previously validated.17 Also, other measurements, including the food‐frequency questionnaire, weight, and BMI, had been previously validated.19,21 However, a limitation of our study is the low number of observed deaths. The observed mortality rate is lower than the mortality rate expected in the Spanish general population. According to data from Spanish Institute of Statistic39 we would have expected approximately 128 deaths in a sample of this size from the general Spanish population with this same distribution by sex and age. However, the higher educational level and the healthy worker effect may account for the lower mortality actually observed in the SUN cohort. Due to the low number of deaths, Poisson regressions were fitted. As a sensitivity analysis we also calculated a Cox regression and results hardly changed, the adjusted hazard ratio per 2 additional h/d of television viewing was 1.41 (95% CI 1.07 to 1.85).
In conclusion, consistently with previous studies, television viewing was associated with all‐cause mortality in our cohort. These results support the need for further observational studies and randomized trials specifically designed to assess the impact of interventions aimed to reduce television viewing on total mortality. Further studies are needed to confirm the effect of computer use and driving on mortality, and to determine the exact biological mechanisms explaining these associations.
Sources of Funding
This work was supported by Spanish Government grants (PI10/02658, PI10/02293, PI13/00615, RD06/0045, G03/140, and 87/2010), the Navarra Regional Government (45/2011, 27/2012) and the University of Navarra.
Disclosures
None.
Acknowledgments
We are indebted to the participants of the SUN Study for their continued cooperation and participation. We thank other members of the SUN Group: Alonso A, Barrio López MT, Benito Corchón S, Beunza JJ, Carlos Chillerón S, Carmona L, Cervantes S, de Irala Estévez J, de la Fuente Arrillaga C, de la Rosa PA, Delgado Rodríguez M, Donat Vargas CL, Fernández Montero A, Galbete Ciáurriz C, García López M, Goñi Ochandorena E, Guillén Grima F, Hernández A, Lahortiga F, Llorca J, López del Burgo C, Marí Sanchís A, Martí del Moral A, Martín Calvo N, Martínez JA, Pimenta AM, Ruiz‐Canela M, Ruiz Zambrana A, Sánchez Adán D, Sánchez‐Villegas A, Sayón Orea C, Toledo Atucha J, Vázquez Ruiz Z, Zazpe García I.
References
- 1.World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva, Switzerland: Who Press; 2009. [Google Scholar]
- 2.Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report 2008. Washington, DC: US Dept of Health and Human Services; 2008. [DOI] [PubMed] [Google Scholar]
- 3.Dietz WH. The role of lifestyle in health: the epidemiology and consequences of inactivity. Proc Nutr Soc. 1996; 55:829-840. [DOI] [PubMed] [Google Scholar]
- 4.Owen N, Healy GN, Matthews CE, Dunstan DW. Too much sitting: the population health science of sedentary behavior. Exerc Sport Sci Rev. 2010; 38:105-113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Grontved A, Hu FB. Television viewing and risk of type 2 diabetes, cardiovascular disease, and all‐cause mortality: a meta‐analysis. JAMA. 2011; 305:2448-2455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wilmot EG, Edwardson CL, Achana FA, Davies MJ, Gorely T, Gray LJ, Khunti K, Yates T, Biddle SJ. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: systematic review and meta‐analysis. Diabetologia. 2012; 55:2895-2905. [DOI] [PubMed] [Google Scholar]
- 7.Patel AV, Bernstein L, Deka A, Feigelson HS, Campbell PT, Gapstur SM, Colditz GA, Thun MJ. Leisure time spent sitting in relation to total mortality in a prospective cohort of us adults. Am J Epidemiol. 2010; 172:419-429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Katzmarzyk PT, Church TS, Craig CL, Bouchard C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med Sci Sports Exerc. 2009; 41:998-1005. [DOI] [PubMed] [Google Scholar]
- 9.Dunstan DW, Barr EL, Healy GN, Salmon J, Shaw JE, Balkau B, Magliano DJ, Cameron AJ, Zimmet PZ, Owen N. Television viewing time and mortality: the Australian diabetes, obesity and lifestyle study (AusDiab). Circulation. 2010; 121:384-391. [DOI] [PubMed] [Google Scholar]
- 10.Matthews CE, George SM, Moore SC, Bowles HR, Blair A, Park Y, Troiano RP, Hollenbeck A, Schatzkin A. Amount of time spent in sedentary behaviors and cause‐specific mortality in us adults. Am J Clin Nutr. 2012; 95:437-445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Matthews CE, Chen KY, Freedson PS, Buchowski MS, Beech BM, Pate RR, Troiano RP. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am J Epidemiol. 2008; 167:875-881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Owen N, Sparling PB, Healy GN, Dunstan DW, Matthews CE. Sedentary behavior: emerging evidence for a new health risk. Mayo Clin Proc. 2010; 85:1138-1141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Altenburg TM, de Kroon ML, Renders CM, Hirasing R, Chinapaw MJ. TV time but not computer time is associated with cardiometabolic risk in Dutch young adults. PLoS One. 2013; 8:e57749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pinto Pereira SM, Ki M, Power C. Sedentary behaviour and biomarkers for cardiovascular disease and diabetes in mid‐life: the role of television‐viewing and sitting at work. PLoS One. 2012; 7:e31132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ford ES, Caspersen CJ. Sedentary behaviour and cardiovascular disease: a review of prospective studies. Int J Epidemiol. 2012; 41:1338-1353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Segui‐Gomez M, de la Fuente C, Vazquez Z, de Irala J, Martinez‐Gonzalez MA. Cohort profile: the ‘seguimiento universidad de navarra’ (SUN) study. Int J Epidemiol. 2006; 35:1417-1422. [DOI] [PubMed] [Google Scholar]
- 17.Martinez‐Gonzalez MA, Lopez‐Fontana C, Varo JJ, Sanchez‐Villegas A, Martinez JA. Validation of the spanish version of the physical activity questionnaire used in the nurses' health study and the health professionals' follow‐up study. Public Health Nutr. 2005; 8:920-927. [DOI] [PubMed] [Google Scholar]
- 18.Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, O'Brien WL, Bassett DR, Jr, Schmitz KH, Emplaincourt PO, Jacobs DR, Jr, Leon AS. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000; 32:S498-S504. [DOI] [PubMed] [Google Scholar]
- 19.Martin‐Moreno JM, Boyle P, Gorgojo L, Maisonneuve P, Fernandez‐Rodriguez JC, Salvini S, Willett WC. Development and validation of a food frequency questionnaire in spain. Int J Epidemiol. 1993; 22:512-519. [DOI] [PubMed] [Google Scholar]
- 20.Trichopoulou A, Costacou T, Bamia C, Trichopoulos D. Adherence to a mediterranean diet and survival in a greek population. N Engl J Med. 2003; 348:2599-2608. [DOI] [PubMed] [Google Scholar]
- 21.Bes‐Rastrollo M, Pérez Valdivieso JR, Sánchez‐Villegas A, Alonso A, Martínez‐Gónzalez MA. Validación del peso e índice de masa corporal auto‐declarados de los participantes de una cohorte de graduados universitarios [Validation of the self‐reported weight and body mass index of the participants in a cohort of university graduates]. Rev Esp Obes. 2005; 3:352-358. [Google Scholar]
- 22.Cleland VJ, Schmidt MD, Dwyer T, Venn AJ. Television viewing and abdominal obesity in young adults: is the association mediated by food and beverage consumption during viewing time or reduced leisure‐time physical activity? Am J Clin Nutr. 2008; 87:1148-1155. [DOI] [PubMed] [Google Scholar]
- 23.Instituto Nacional de Estadistica. Encuesta de empleo del tiempo 2009–2010 [Time Use Survey 2009–2010] Available at: http://www.ine.es/prensa/np606.pdf. Accessed March 24, 2014.
- 24.Matthews CE, Jurj AL, Shu XO, Li HL, Yang G, Li Q, Gao YT, Zheng W. Influence of exercise, walking, cycling, and overall nonexercise physical activity on mortality in chinese women. Am J Epidemiol. 2007; 165:1343-1350. [DOI] [PubMed] [Google Scholar]
- 25.Manini TM, Everhart JE, Patel KV, Schoeller DA, Colbert LH, Visser M, Tylavsky F, Bauer DC, Goodpaster BH, Harris TB. Daily activity energy expenditure and mortality among older adults. JAMA. 2006; 296:171-179. [DOI] [PubMed] [Google Scholar]
- 26.Healy GN, Dunstan DW, Salmon J, Cerin E, Shaw JE, Zimmet PZ, Owen N. Objectively measured light‐intensity physical activity is independently associated with 2‐h plasma glucose. Diabetes Care. 2007; 30:1384-1389. [DOI] [PubMed] [Google Scholar]
- 27.Nang EE, Salim A, Wu Y, Tai ES, Lee J, Van Dam RM. Television screen time, but not computer use and reading time, is associated with cardio‐metabolic biomarkers in a multiethnic asian population: a cross‐sectional study. Int J Behav Nutr Phys Act. 2013; 10:70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hu FB, Li TY, Colditz GA, Willett WC, Manson JE. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. JAMA. 2003; 289:1785-1791. [DOI] [PubMed] [Google Scholar]
- 29.Stamatakis E, Hamer M, Dunstan DW. Screen‐based entertainment time, all‐cause mortality, and cardiovascular events: population‐based study with ongoing mortality and hospital events follow‐up. J Am Coll Cardiol. 2011; 57:292-299. [DOI] [PubMed] [Google Scholar]
- 30.Wijndaele K, Brage S, Besson H, Khaw KT, Sharp SJ, Luben R, Wareham NJ, Ekelund U. Television viewing time independently predicts all‐cause and cardiovascular mortality: the epic norfolk study. Int J Epidemiol. 2011; 40:150-159. [DOI] [PubMed] [Google Scholar]
- 31.Ford ES. Combined television viewing and computer use and mortality from all‐causes and diseases of the circulatory system among adults in the United States. BMC Public Health. 2012; 12:70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Warren TY, Barry V, Hooker SP, Sui X, Church TS, Blair SN. Sedentary behaviors increase risk of cardiovascular disease mortality in men. Med Sci Sports Exerc. 2010; 42:879-885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Morris JN, Heady JA, Raffle PA, Roberts CG, Parks JW. Coronary heart‐disease and physical activity of work. Lancet. 1953; 265:1053-1057. [DOI] [PubMed] [Google Scholar]
- 34.Morris JN, Heady JA, Raffle PA, Roberts CG, Parks JW. Coronary heart‐disease and physical activity of work. Lancet. 1953; 265:1111-1120. [DOI] [PubMed] [Google Scholar]
- 35.van der Ploeg HP, Chey T, Korda RJ, Banks E, Bauman A. Sitting time and all‐cause mortality risk in 222 497 australian adults. Arch Intern Med. 2012; 172:494-500. [DOI] [PubMed] [Google Scholar]
- 36.Zderic TW, Hamilton MT. Physical inactivity amplifies the sensitivity of skeletal muscle to the lipid‐induced downregulation of lipoprotein lipase activity. J Appl Physiol. 2006; 100:249-257. [DOI] [PubMed] [Google Scholar]
- 37.Tremblay MS, Colley RC, Saunders TJ, Healy GN, Owen N. Physiological and health implications of a sedentary lifestyle. Appl Physiol Nutr Metab. 2010; 35:725-740. [DOI] [PubMed] [Google Scholar]
- 38.Dong L, Block G, Mandel S. Activities contributing to total energy expenditure in the United States: results from the NHAPS study. Int J Behav Nutr Phys Act. 2004; 1:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Instituto Nacional de Estadistica. Tablas de mortalidad de la población de España 1991–2012 [Mortality Tables of Spanish Population 1991–2012] Available at: http://www.ine.es/inebmenu/mnu_dinamicapob.htm. Accessed March 24, 2014.