

Abstract
Objective
To investigate the safety of long-term subcutaneous (SC) abatacept treatment using integrated clinical trial data obtained in patients with rheumatoid arthritis refractory to traditional disease-modifying antirheumatic drugs.
Methods
Data from the double-blind and open-label phases of 5 clinical trials of SC abatacept were pooled. The overall and 6-month incidence rates were calculated as events per 100 patient-years of exposure.
Results
This analysis included 1,879 patients with 4,214.6 patient-years of exposure to SC abatacept. The mean ± SD length of exposure was 27.3 ± 9.1 months. The reported incidence rate of serious infections was 1.79 (95% confidence interval [95% CI] 1.42–2.24); the most frequent infections were pneumonia (incidence rate 0.36 [95% CI 0.22–0.59]), urinary tract infection (incidence rate 0.14 [95% CI 0.06–0.32]), and gastroenteritis (incidence rate 0.10 [95% CI 0.04–0.25]). Tuberculosis occurred rarely (incidence rate 0.09 [95% CI 0.04–0.25]). The reported incidence rate of malignancies was 1.32 (95% CI 1.01–1.72), and the most common was solid organ malignancy (incidence rate 0.69 [95% CI 0.48–0.99]). The incidence rate of autoimmune events was 1.37 (95% CI 1.06–1.78), and the most frequent events were psoriasis (incidence rate 0.33 [95% CI 0.20–0.56]) and Sjögren's syndrome (incidence rate 0.24 [95% CI 0.13–0.44]). The reported incidence rate of local injection site reactions was 1.72 (95% CI 1.36–2.17); these events occurred primarily during the first 6 months of treatment, and almost all were of mild or moderate intensity. The incidence rates of serious infections, malignancies, autoimmune events, and injection site reactions did not increase over time.
Conclusion
Long-term treatment with SC abatacept was associated with low incidence rates of serious infections, malignancies, and autoimmune events and was well tolerated, with infrequent injection site reactions. These findings are consistent with those related to treatment with intravenous abatacept. Long-term treatment with SC abatacept did not lead to new safety signals over time.
The use of biologic agents for the treatment of rheumatoid arthritis (RA) can increase the risk of adverse safety events such as infections, malignancy, and autoimmune events (1) and may be associated with an increased risk of immunogenicity (2) and a loss of efficacy (3,4). Subcutaneous (SC) administration of biologic agents may also cause injection site reactions (5). Furthermore, due to the chronic nature of RA and the increasing emphasis on earlier and more aggressive treatment, patients are likely to receive biologic therapy for extended periods of time (1,6). Therefore, physicians need treatments that not only provide a rapid positive response but also minimize long-term safety risks while maximizing long-term adherence to therapy (7).
Abatacept is a fully human, soluble, recombinant fusion protein that selectively modulates the CD80/CD86–CD28 costimulatory signal required for full T cell activation, resulting in decreased T cell proliferation and reduced production of proinflammatory cytokines (8). Treatment with intravenous (IV) abatacept has demonstrated consistent safety and favorable efficacy benefits in clinical trials in a range of different populations of patients with RA (9–16), and the benefits of IV abatacept are maintained with continued long-term treatment (17–19). These data are supported by real-world studies and long-term registry data, all of which reflect the balance of benefits and risks of treatment in clinical practice and demonstrate the sustained efficacy and safety of abatacept for the treatment of RA (20,21).
Integrated analyses of clinical trial data allow us to assess the long-term safety of biologic agents in combined large patient populations with exposure to the study drug. Periodic reassessment of safety data from such integrated analyses using incidence rates allows a standardized assessment of safety that can, over time, demonstrate any cumulative increased risk or new safety signals. Data reflecting up to 7 years of treatment have shown that IV abatacept is well tolerated, with stable incidence rates of serious infections, malignancy, and autoimmune events, and no new safety signals over time (22).
A formulation of abatacept that allows SC self-administration by the patient has been studied in 5 phase II and phase III trials (23–27). Integration of these trial data allows for a comprehensive evaluation of long-term safety and occurrence of adverse events (AEs) related to SC administration as well as a comparison with the established safety of IV abatacept. In the present study, we describe the results of an integrated safety analysis of long-term SC abatacept treatment, using combined data from 5 clinical trials in patients with RA with a total exposure of 4,214.6 patient-years.
PATIENTS AND METHODS
Data were derived from the double-blind and open-label phases of 5 clinical trials of SC abatacept in patients with active RA, as defined by the 1987 American College of Rheumatology revised criteria for the classification of RA (28) and the American College of Rheumatology 1991 revised criteria for the classification of global functional status in RA (29). One phase IIa randomized controlled trial, 2 phase IIIb randomized controlled trials, and 2 phase IIIb open-label studies were included (Table1) (23–27). The majority of patients had experienced an inadequate response to methotrexate (MTX). All studies were carried out in accordance with the Declaration of Helsinki and were consistent with International Conference on Harmonisation Good Clinical Practice guidelines. Data for patients treated with IV abatacept in a previously reported integrated safety analysis were used for a comparison of events (22).
Table 1.
Trials of SC abatacept included in the safety analyses*
| Study (ref.) |
|||||
|---|---|---|---|---|---|
| Phase IIa dose-finding study (23) | ALLOW (25) | ACCOMPANY (27) | ACQUIRE (24) | ATTUNE (26) | |
| Cutoff date for data inclusion | July 2011 | July 2011 | July 2011 | July 2011 | July 2011 |
| ClinicalTrials.gov identifier | NCT00254293 | NCT00533897 | NCT00547521 | NCT00559585 | NCT00663702 |
| Patient population | Active RA, inadequate response (≥3 months) to MTX therapy plus ≥1 additional DMARD | Active RA, inadequate response (≥3 months) to MTX therapy | Active RA, inadequate response to ≥1 DMARD; patients treated with or without background MTX | Active RA, inadequate response (≥3 months) to MTX therapy | Active RA and either inadequate response to MTX therapy or inadequate response to anti-TNF therapy† |
| Abatacept dosage | Weight-tiered (75–200 mg) or fixed (125 mg) weekly dose | 125 mg/week following IV abatacept loading dose (∼10 mg/kg) | 125 mg/week, no IV abatacept loading dose | 125 mg/week following IV abatacept loading dose (∼10 mg/kg) | 125 mg/week; patients switched from long-term IV abatacept treatment |
| Short-term period | 12-week double-blind, placebo-controlled | Period I, 12-week open-label‡ | 4-month open-label, with or without MTX | 6-month double-blind, double-dummy with IV and SC abatacept | 12-month open-label, single-arm |
| Period II, 12-week double-blind, placebo-controlled Period III, 12-week open-label§ |
|||||
The open-label long-term extension period includes patients who switched from placebo to abatacept after the double-blind, placebo-controlled periods. The cumulative period (short-term plus long-term extension periods) includes patients who received subcutaneous (SC) abatacept at any time point. ALLOW = Evaluation of Abatacept Administered Subcutaneously in Adults with Active Rheumatoid Arthritis; ACCOMPANY = Abatacept in Subjects with Rheumatoid Arthritis Administered Plus or Minus Background MTX Subcutaneously; ACQUIRE = Abatacept Comparison of Sub[QU]cutaneous versus Intravenous in Inadequate Responders to MethotrexatE; ATTUNE = Abatacept in Subjects who Switch from Intravenous to Subcutaneous Therapy; RA = rheumatoid arthritis; MTX = methotrexate; DMARD = disease-modifying antirheumatic drug; anti-TNF = anti–tumor necrosis factor.
Patients in the Abatacept in Inadequate Responders to MTX (AIM) trial and the Abatacept Trial in the Treatment of Anti-TNF Inadequate Responders (ATTAIN) trial received ≥4 years of intravenous (IV) abatacept treatment.
Nonresponders could directly enter the long-term extension.
The long-term extension began after the end of period III.
All patients who received ≥1 dose of abatacept were evaluated for safety, including AEs, serious AEs (SAEs), and events of clinical interest (i.e., serious infections, malignancies, autoimmune events, and injection site reactions). The incidence rate of a safety event was calculated as the number of events per 100 patient-years of exposure, providing an estimate of the number of events that would occur if 100 patients were treated for 1 year. Exposure to SC abatacept was counted in days from the start of SC abatacept therapy until the first event or database locking (whichever occurred first); for patients who discontinued treatment prior to database locking, exposure was counted from the start of therapy until the first event or the end of treatment period plus 56 days (4 half-lives of abatacept in humans), whichever occurred first.
Incidence rates with 95% confidence intervals (95% CIs; Poisson distribution) were calculated overall and in 6-month intervals for the cumulative period (short-term plus long-term extension periods; includes patients who received SC abatacept at any time point). For 6-month incidence rate assessments, events were counted in the 6-month interval in which they occurred. Each patient contributed patient-years to a 6-month interval if they had been exposed to abatacept during that interval and had not experienced a particular AE prior to that interval.
Comparisons of safety events according to baseline body weight (<60 kg, 60–100 kg, and >100 kg) were conducted to ensure that the safety profile of SC abatacept, which is administered at a fixed dose rather than the weight-tiered dose of the IV formulation, was consistent regardless of patient weight. Safety events were also compared across different age groups (<65 years, ≥65 years, and ≥75 years) and according to sex. In addition, because the majority of patients in the SC abatacept clinical trial program had experienced an inadequate response to MTX, it was also of interest to assess the safety profile of the subgroup of patients who previously received or received and failed to respond to anti–tumor necrosis factor (anti-TNF) therapy at some point during their treatment history.
An electrochemiluminescence assay was used to assess immunogenicity during the trials included in this integrated analysis, based on the proportion of patients with a seropositive response, which was defined as an antibody titer of ≥10.
RESULTS
Patient disposition
The analysis included 1,879 patients. Among these patients, 1,576 (83.9%) were receiving treatment at the time of the analysis. The most common reasons for treatment discontinuation were lack of efficacy (n = 86 [4.6%]), AEs (n = 68 [3.6%]), or withdrawal of consent (n = 45 [2.4%]).
Exposure and overall safety
Overall, 4,214.6 patient-years of exposure to SC abatacept were included in this analysis. The mean ± SD length of exposure to SC abatacept was 27.3 ± 9.1 months (range 2–57 months, median 29.1 months). Most patients (95.3%) were receiving concomitant MTX at baseline. A total of 62.9% of patients were receiving corticosteroids at baseline (mean oral dose 4.1 mg).
The overall incidence rate of AEs in this integrated analysis was 136.13 (95% CI 129.71–142.87). The reported overall incidence rate of SAEs was 9.97 (95% CI 9.02–11.02). The SAEs most frequently reported were those affecting musculoskeletal and connective tissue (incidence rate 1.94 [95% CI 1.56–2.41]), and infections (incidence rate 1.79 [95% CI 1.42–2.24]). The most common serious musculoskeletal and connective tissue disorders were osteoarthritis (incidence rate 0.65 [95% CI 0.44–0.94]), RA (incidence rate 0.55 [95% CI 0.36–0.83]), back pain (incidence rate 0.14 [95% CI 0.06–0.32]), and arthritis (incidence rate 0.12 [95% CI 0.05–0.29]).
The overall cumulative incidence rates of other classes of events were as follows: 1.13 (95% CI 0.85–1.50) for cardiac disorders; 0.72 (95% CI 0.50–1.03) for gastrointestinal disorders; 0.64 (95% CI 0.44–0.94) for general disorders and administration site conditions; 0.62 (95% CI 0.42–0.91) for nervous system disorders; 0.62 (95% CI 0.42–0.91) for respiratory, thoracic, and mediastinal disorders; 0.40 (95% CI 0.25–0.65) for hepatobiliary disorders; 0.31 (95% CI 0.18–0.53) for renal and urinary disorders; 0.26 (95% CI 0.14–0.47) for vascular disorders; and 0.19 (95% CI 0.10–0.38) for blood and lymphatic system disorders. In total, the reported incidence rate of serious infections was 1.79 (95% CI 1.42–2.24). The most frequent serious infections (incidence rate ≥0.10) were pneumonia (incidence rate 0.36 [95% CI 0.22–0.59]), urinary tract infection (incidence rate 0.14 [95% CI 0.06–0.32]), and gastroenteritis (incidence rate 0.10 [95% CI 0.04–0.25]) (Table2).
Table 2.
Summary of safety events associated with SC and IV abatacept*
| SC abatacept |
IV abatacept |
|||
|---|---|---|---|---|
| Event | Patients with event | Incidence rate (95% CI) | Patients with event | Incidence rate (95% CI) |
| Deaths | 25 (1.3) | 0.59 (0.40–0.88) | 73 (1.8) | 0.60 (0.47–0.76) |
| Overall SAEs | 384 (20.4) | 9.97 (9.02–11.02) | 1,373 (33.1) | 14.61 (13.85–15.41) |
| Infections | 1,176 (62.6) | 50.52 (47.72–53.50) | 2,997 (72.3) | 75.65 (72.96–78.40) |
| Serious infections | ||||
| Total serious infections | 74 (3.9) | 1.79 (1.42–2.24) | 332 (0.8) | 2.87 (2.57–3.19) |
| Pneumonia | 15 (0.8) | 0.36 (0.22–0.59) | 55 (1.3) | 0.46 (0.34–0.59) |
| Urinary tract infection | 6 (0.3) | 0.14 (0.06–0.32) | 24 (0.6) | 0.20 (0.13–0.30) |
| Gastroenteritis | 4 (0.2) | 0.10 (0.04–0.25) | 14 (0.3) | 0.12 (0.06–0.19) |
| Tuberculosis | 4 (0.2) | 0.09 (0.04–0.25) | 8 (0.2) | 0.07 (0.03–0.13) |
| Bronchitis | 4 (0.2) | 0.09 (0.04–0.25) | NA | NA |
| Herpes zoster | 3 (0.2) | 0.07 (0–0.22) | 4 (0.1) | 0.03 (0.01–0.08) |
| Lobar pneumonia | 3 (0.2) | 0.07 (0.02–0.22) | 13 (0.3) | 0.11 (0.06–0.18) |
| Common malignancies† | ||||
| Total excluding NMSC | 30 (1.6) | 0.71 (0.50–1.02) | 88 (2.1) | 0.73 (0.58–0.89) |
| Solid organ (combined) | 29 (1.5) | 0.69 (0.48–0.99) | 72 (1.7) | 0.59 (0.46–0.75) |
| NMSC (combined) | 24 (1.3) | 0.57 (0.39–0.86) | 80 (1.9) | 0.67 (0.53–0.83) |
| Basal cell (combined) | 19 (1.0) | 0.45 (0.29–0.71) | 58 (1.4) | 0.48 (0.37–0.62) |
| Squamous cell (combined) | 9 (0.5) | 0.21 (0.11–0.41) | 32 (0.8) | 0.27 (0.18–0.37) |
| Breast (combined) | 7 (0.4) | 0.17 (0.08–0.35) | 14 (0.3) | 0.12 (0.06–0.19) |
| Lung (combined) | 5 (0.3) | 0.12 (0.05–0.29) | 18 (0.4) | 0.15 (0.09–0.23) |
| Endometrial/uterine (combined) | 3 (0.2) | 0.07 (0.02–0.22) | 4 (0.1) | 0.03 (0.01–0.08) |
| Melanoma (combined) | 3 (0.2) | 0.07 (0.02–0.22) | 4 (0.1) | 0.03 (0.01–0.08) |
| Common autoimmune events‡ | ||||
| Total autoimmune events | 57 (3.0) | 1.37 (1.06–1.78) | 232 (5.6) | 1.99 (1.74–2.26) |
| Psoriasis | 14 (0.7) | 0.33 (0.20–0.56) | 68 (1.6) | 0.57 (0.44–0.72) |
| Sjögren's syndrome | 10 (0.5) | 0.24 (0.13–0.44) | 23 (0.6) | 0.19 (0.12–0.29) |
| Erythema nodosum | 5 (0.3) | 0.12 (0.05–0.29) | 16 (0.4) | 0.13 (0.08–0.21) |
| Episcleritis | 5 (0.3) | 0.12 (0.05–0.29) | 15 (0.4) | 0.12 (0.7–0.20) |
The group receiving subcutaneous (SC) abatacept comprised 1,879 patients with 4,215 patient-years of followup; the group receiving intravenous (IV) abatacept comprised 4,149 patients with 12,132 patient-years of followup. Incidence rates are events per 100 patient-years and are normalized for exposure. Serious infections are a subset of serious adverse events (SAEs) and infections. Except where indicated otherwise, values are the number (%). 95% CI = 95% confidence interval; NA = not applicable; NMSC = nonmelanoma skin cancer.
Defined as incidence rates of >0.06 per 100 patient-years in patients receiving SC abatacept.
Defined as incidence rates of >0.1 per 100 patient-years in patients receiving SC abatacept.
The incidence rate of opportunistic infections was 0.31 (95% CI 0.18–0.53); opportunistic infections included herpes zoster (incidence rate 1.33 [95% CI 1.02–1.73]). Herpes zoster infections that were SAEs occurred at an incidence rate of 0.07 (95% CI 0–0.22). Tuberculosis (TB) occurred at an incidence rate of 0.09 (95% CI 0.04–0.25). A total of 4 cases of TB were reported (30): 2 cases of pulmonary TB (reported on day 317 of treatment in a patient with normal chest radiography findings and a negative tuberculin purified protein derivative [PPD] test result at baseline and on day 791 of treatment in a patient for whom no baseline information was available); 1 case of peritoneal TB (reported on day 537 of treatment in a patient with a history of childhood TB and for whom no baseline information was available); and 1 case of TB infection with no disease (reported on day 349 of treatment in a patient with normal chest radiography findings and negative PPD test result at baseline). Three of the patients were from South America, and the other patient was from Asia; all events resulted in treatment discontinuation. During the cumulative period, the incidence rates of TB at 6-month intervals did not increase with increasing exposure over time (incidence rates 0.11 [95% CI 0.02–0.78], 0.12 [95% CI 0.02–0.83], 0.12 [95% CI 0.02–0.87], 0.00 [95% CI 0.00–0.00], and 0.18 [95% CI 0.02–1.26] at months 0–6, 6–12, 12–18, 18–24, and 24–30, respectively).
The reported incidence rate of total malignancies was 1.32 (95% CI 1.01–1.72), and the incidence rate of total malignancies excluding nonmelanoma skin cancer (NMSC) was 0.71 (95% CI 0.50–1.02). The most frequent malignancies (incidence rate ≥0.2) were NMSC (incidence rate 0.57 [95% CI 0.39–0.86]), basal cell combined (incidence rate 0.45 [95% CI 0.29–0.71]), and squamous cell combined (incidence rate 0.21 [95% CI 0.11–0.41]) (Table2). A single case of B cell lymphoma was reported (incidence rate 0.02 [95% CI 0.00–0.17]). During the cumulative period, 27 patients had malignancies that resulted in discontinuation of the study drug. The incidence rates of malignancies at 6-month intervals did not increase with increasing exposure over time.
During the cumulative period, the reported incidence rate of autoimmune events was 1.37 (95% CI 1.06–1.78). The most frequent autoimmune events reported were psoriasis (incidence rate 0.33 [95% CI 0.20–0.56]), Sjögren's syndrome (incidence rate 0.24 [95% CI 0.13–0.44]), erythema nodosum, and episcleritis (incidence rate for both 0.12 [95% CI 0.05–0.29]) (Table2). The incidence rates of psoriasis at 6-month intervals remained stable with increasing exposure over time (incidence rates 0.33 [95% CI 0.11–1.02], 0.12 [95% CI 0.02–0.83], 0.49 [95% CI 0.18–1.31], and 0.79 [95% CI 0.35–1.75] during months 0–6, 6–12, 12–18, and 18–24, respectively)
Most prespecified autoimmune events were of mild-to-moderate intensity; 4 autoimmune events were considered severe (multiple sclerosis [MS], psoriasis, Crohn's disease, and vasculitis). The case of MS occurred on day 516 of abatacept treatment in a 44-year-old Caucasian female. The event was considered by the investigator to be possibly related to the study drug and led to discontinuation in that patient. Severe psoriasis was reported in 1 patient on day 839 of treatment and was considered to be an exacerbation of a mild event occurring on day 700; however, the event was considered to be unrelated to the study drug, and the patient continued to receive treatment. The case of Crohn's disease occurred on day 752 of treatment, was considered to be unrelated to the study drug, and did not result in discontinuation. The case of severe vasculitis (not otherwise specified) occurred on day 253 of treatment, was considered to be unrelated to the study drug, and did not lead to interruption or discontinuation of treatment with the study drug; the patient was treated with prednisone 20 mg/day, and the event was ongoing at the time of database locking. One event was considered to be very severe: rapid onset of vasculitis (again, not otherwise specified) that occurred on treatment day 574 in a patient with no history of vasculitis. Although the event was considered unlikely to be related to the study drug, it did lead to study drug discontinuation; the patient was treated with high dosages of corticosteroids (60 mg/day), and the event was ongoing at the time of database locking.
Deaths occurred at an incidence rate of 0.59 (95% CI 0.40–0.88). Of 7 deaths classified as certainly, probably, or possibly related to treatment, 4 were due to infections (including 2 cases of pneumonia [combined with pulmonary TB in 1 patient], 1 gastrointestinal infection, and 1 case of staphylococcal sepsis), 1 death was caused by peritoneal neoplasm, 1 was due to a combination of wound infection and malignant lung neoplasm, and 1 was attributable to multiorgan failure. An additional 18 deaths were considered unlikely to be related or unrelated to treatment; these deaths were most frequently due to cardiovascular events (n = 7).
The reported incidence rate of prespecified local injection site reactions was 1.72 (95% CI 1.36–2.17); these reactions occurred predominantly during the first 6 months of treatment. All except 1 reaction were of mild-to-moderate intensity. The most commonly reported injection site reactions (incidence rate ≥0.10) were erythema, pain, pruritus, hematoma (incidence rate 0.33 [95% CI 0.2–0.6] for all), reaction (incidence rate 0.24 [95% CI 0.13–0.44]), swelling (incidence rate 0.12 [95% CI 0.05–0.29]), rash (incidence rate 0.10 [95% CI 0.04–0.25]), and papule (incidence rate 0.10 [95% CI 0.04–0.25]). Injection site reactions led to discontinuation of the study drug in 2 patients (1 due to erythema and mild pruritus at the injection site and 1 due to a severe injection site reaction).
Clinical laboratory abnormalities during the cumulative period
Abatacept was not associated with any clinically significant abnormalities of laboratory values. Low leukocyte counts were reported in 35 patients (1.9%), and low platelet counts were reported in 4 patients (0.2%). Mean leukocyte and platelet counts were stable throughout the cumulative period. Elevations in alanine transaminase (ALT) and aspartate transaminase (AST) levels were reported in 46 patients (2.4%) and 26 patients (1.4%), respectively. An elevation in the serum creatinine level was reported in 122 patients (6.5%). Mean blood chemistry values for ALT, AST, and creatinine were similar throughout the cumulative period.
Immunogenicity
During the cumulative period, 8.2% of all patients in the 4 combined phase III studies (143 of 1,749) had a positive response to testing for immunogenicity at some point while receiving treatment (based on electrochemiluminescence data), and 9.2% of patients (161 of 1,758) had positive test results at some point during the treatment and/or posttreatment periods. Abatacept-induced seropositivity was generally not persistent; only 1.4% of patients (24 of 1,723) were seropositive at ≥2 consecutive visits. In addition, in most patients, antibody titers were low: only 3 patients with abatacept-induced immunogenicity had titers of >100 while receiving SC abatacept (a positive response was defined as a titer of ≥10).
As reported for the individual trials (23,25,27,31), immunogenicity with SC abatacept did not appear to have any impact on safety in this pooled safety analysis. During the cumulative period, 25 (15.5%) of 161 patients with abatacept-induced immunogenicity experienced an SAE, 5 of which were classified by the investigator as possibly related to the study drug (exacerbation of acute diverticulitis, basal cell carcinoma, Ludwig's angina, respiratory tract infection, and dyspnea); however, investigators were unaware of immunogenicity status when classifying relatedness. Of the 25 seropositive patients who reported SAEs, 19 remained in the study. For 14 of these 19 patients, the seropositive samples were detected after the occurrence of the SAE. In the 5 patients in whom the seropositive samples were obtained during treatment and in whom these samples were detected prior to the occurrence of the SAE, no association between the event and the presence of the anti-abatacept antibodies could be established post hoc; the events were either unrelated to or not typically associated with immunogenicity (e.g., limb injury due to a fall, hip replacement surgery) and/or showed no temporal relationship with the presence of antibodies.
AEs in patients with abatacept-induced immunogenicity led to discontinuation in 8 patients (5.0%); 3 (1.9%) of these discontinuations were attributable to SAEs. In the 3 patients who discontinued due to SAEs, the events were not temporally associated with immunogenicity and/or were not classified as being related to study drug. During the cumulative period, 5 (3.1%) of 161 patients with abatacept-induced immunogenicity experienced an autoimmune event, including 2 cases of psoriasis and 1 case each of dermatomyositis, ulcerative colitis, and vasculitis. All autoimmune events were of mild-to-moderate intensity, and none led to discontinuation of the study drug. One case of psoriasis that occurred on day 753 was classified as possibly being related to the study drug; no other events were classified as being related. Three patients (1.9%) had prespecified local injection site reactions with concurrent abatacept-induced immunogenicity during the cumulative period. In these patients, injection site reactions were mild and did not appear to be related to immunogenicity (no temporal relationship/event related to the presence of anti-abatacept antibodies).
Safety over time
The incidence rates of SAEs at 6-month intervals were low and did not increase with increased abatacept exposure. The incidence rates of SAEs during each 6-month interval were 9.25 (95% CI 7.46–11.48) during the first 6 months and 10.40 (95% CI 7.88–13.72) during months 24–30. Similarly, incidence rates of serious infections (Figure 1), malignancies, and autoimmune events (Figure 2) remained relatively stable over time with increasing exposure, as evidenced by overlapping 95% CIs at all time points (32). The incidence rates of overall infections decreased over time, from an incidence rate of 74.67 (95% CI 68.76–81.08) at 6 months to an incidence rate of 31.12 (95% CI 25.63–37.78) at month 24 (Figure 1); the 95% CIs did not overlap. The incidence of injection site reactions also decreased, from an incidence rate of 5.59 at 6 months (50 patients were affected during months 0–6) to an incidence rate of 0.0 at month 24 (no injection site reactions were reported) (Figure 3); again, the 95% CIs did not overlap.
Figure 1.
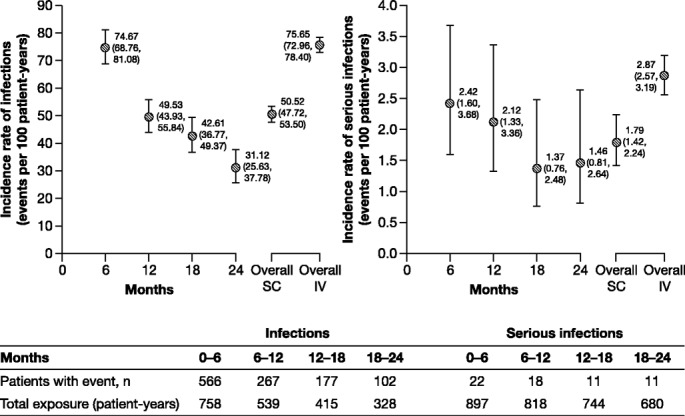
Infections and serious infections in 1,879 patients treated with subcutaneous (SC) abatacept and 4,149 patients previously treated with intravenous (IV) abatacept. Top, Incidence rates (95% confidence intervals) at 6-month intervals in patients treated with SC abatacept, and overall incidence rates in patients treated with SC abatacept and those treated with IV abatacept. Bottom, Numbers of patients with infections and serious infections and total patient-years of exposure at 6-month intervals. Serious infections are a subset of serious adverse events and infections.
Figure 2.
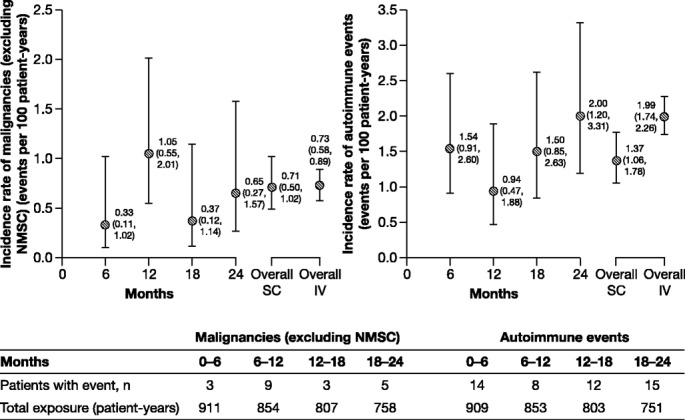
Malignancies (excluding nonmelanoma skin cancer [NMSC]) and autoimmune events in 1,879 patients treated with subcutaneous (SC) abatacept and 4,149 patients previously treated with intravenous (IV) abatacept. Top, Incidence rates (95% confidence intervals) at 6-month intervals in patients treated with SC abatacept, and overall incidence rates in patients treated with SC abatacept and those treated with IV abatacept. Bottom, Numbers of patients with malignancies and autoimmune events and total patient-years of exposure at 6-month intervals. Autoimmune events are prespecified (Medical Dictionary for Regulatory Activities preferred terms).
Figure 3.
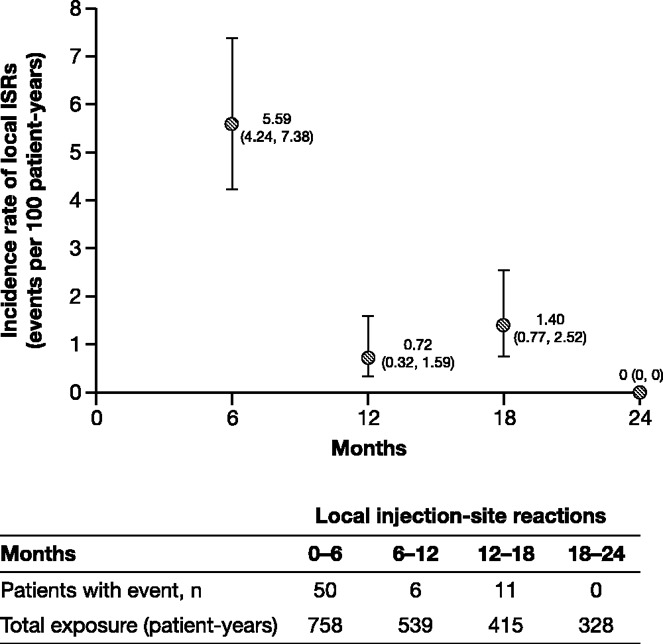
Injection site reactions (ISRs) in 1,879 patients treated with subcutaneous abatacept. Top, Incidence rates (95% confidence intervals) at 6-month intervals. Bottom, Numbers of patients with injection site reactions and total patient-years of exposure at 6-month intervals. Injection site reactions are prespecified (Medical Dictionary for Regulatory Activities preferred terms).
Comparison of safety across patient subgroups
At baseline, ∼24% of patients (n = 450) had a body weight of <60 kg; 67% (n = 1,264) weighed 60–100 kg, and 9% (n = 162) weighed >100 kg. Within these respective weight groups, the mean ± SD durations of exposure to SC abatacept were 27.4 ± 8.4 months, 27.5 ± 8.9 months, and 25.4 ± 12.1 months. During the cumulative period, lower incidence rates (per 100 patient-years) of AEs, SAEs, and AEs that led to discontinuation were observed in the lower-weight groups (<60 kg and 60–100 kg) compared with the higher-weight group (>100 kg) (for AEs, incidence rates 120.68 [95% CI 109.17–133.41] and 133.52 [95% CI 125.88–141.61] versus 250.09 [95% CI 213.22–293.34]; for SAEs, incidence rates 8.91 [95% CI 7.20–11.04] and 9.50 [95% CI 8.39–10.76] versus 17.55 [95% CI 13.34–23.09]; for AEs leading to discontinuation, incidence rates 2.38 [95% CI 1.59–3.54] and 2.21 [95% CI 1.73–2.84] versus 3.88 [95% CI 2.25–6.67]).
During the cumulative period, the mean ± SD durations of exposure to SC abatacept according to age group were 27.5 ± 9.7, 26.1 ± 11.3, and 25.2 ± 13.9 months in patients aged <65 years (n = 1,609), ≥65 years (n = 270), and ≥75 years (n = 46), respectively. Among younger patients, the incidence rates (per 100 patient-years) of AEs, SAEs, and discontinuations due to AEs were lower than those among older patients (in patients aged <65 years, incidence rates 129.81 [95% CI 123.19–136.80], 8.30 [95% CI 7.39–9.34], and 1.79 [95% CI 1.44–2.29], respectively; in patients aged ≥65 years, incidence rates 188.21 [95% CI 166.10–213.26], 21.74 [95% CI 17.94–26.34], and 6.28 [95% CI 4.53–8.70], respectively; in patients aged ≥75 years, incidence rates 214.30 [95% CI 156.58–293.31], 32.79 [95% CI 21.79–49.34], and 9.52 [95% CI 4.96–18.31], respectively).
The mean ± SD durations of exposure to SC abatacept according to sex were 27.3 ± 9.2 months in female patients (n = 1,546) and 27.5 ± 8.7 months in male patients (n = 333). The incidence rate (per 100 patient-years) of SAEs in female patients (8.85 [95% CI 7.73–10.13]) was decreased compared with that in male patients (13.49 [95% CI 10.98–16.59]), while the incidence rate (per 100 patient-years) of AEs and AEs leading to discontinuation were lower in male patients (120.69 [95% CI 107.52–135.46] and 2.13 [95% CI 1.31–3.48], respectively) than in female patients (139.93 [95% CI 132.68–147.58] and 9.24 [95% CI 8.24–10.35], respectively).
Safety during the cumulative period was also evaluated in a subgroup of patients who had previously received anti-TNF treatment. This subgroup comprised 218 patients with a mean ± SD length of exposure to SC abatacept of 26.1 ± 11.6 months. The reported incidence rates (per 100 patient-years) of AEs, SAEs, and AEs leading to discontinuation in this subgroup were 211.52 (95% CI 183.69–43.57), 14.35 (95% CI 11.12–18.52), and 2.80 (95% CI 1.63–4.82), respectively.
Comparative safety of SC and IV abatacept
The incidence rates of overall safety events among patients receiving SC abatacept were compared with those from a previously reported integrated analysis of 4,149 patients treated with IV abatacept, representing up to 7 years of continued exposure (22) (Table2, Figure 1, and Figure 2).
DISCUSSION
In this integrated analysis of clinical trial safety data representing >4,200 patient-years of exposure (mean exposure 27.3 months), long-term treatment with SC abatacept was well tolerated, and no new safety signals were identified. Local injection site reactions were generally mild or moderate and infrequent, and most occurred within the first 6 months of exposure. SC abatacept was not associated with significant increases in the number of infections, malignancies, or autoimmune events over time. This represents the largest analysis of this kind with SC abatacept to date and complements a similar analysis with the IV formulation (22).
Findings from the current analysis suggest that the risk of serious infections with SC abatacept treatment is not increased over time, consistent with previously published observations. Independent meta-analyses have suggested that the risk of serious infections during abatacept treatment (odds ratio 1.35 [95% CI 0.78–2.32] versus placebo) is not significantly increased, and that opportunistic infections are rare with abatacept (33).
Patient subgroup analyses revealed that lower baseline weight (≤100 kg) and younger age (<65 years) were associated with a decreased risk of safety events that was likely attributable to less obesity- and age-related comorbidity compared with patients who were in the higher-weight group or were older. Female patients had a lower incidence rate of SAEs compared with male patients, but male patients demonstrated a lower incidence of AEs and discontinuation due to AEs. SC abatacept was well tolerated in the group that had received anti-TNF treatment during the cumulative period, although the evaluation is limited due to the small sample size (n = 218). No new safety signals were identified compared with the established IV experience (22).
Immunogenicity was transient, with low antibody titers, and did not persist or increase during continued treatment with SC abatacept. Overall rates of immunogenicity were higher in this pooled analysis compared with those in the previously published double-blind or short-term open-label periods of the individual SC abatacept studies (23–27), which generally used the less sensitive enzyme-linked immunosorbent assay instead of the electrochemiluminescence assay used for the long-term extensions of these studies. The general safety profile in patients who experienced immunogenicity, in terms of the frequency of SAEs and discontinuations due to safety events, was comparable with that in the overall patient population treated with SC abatacept, suggesting that immunogenicity had no impact on safety following long-term SC abatacept treatment. The results of individual clinical trials suggest that immunogenicity does not have a significant impact on the efficacy of SC abatacept (23–27). Several phase II and III trials (23,27,31,34) demonstrated that treatment with IV abatacept was also associated with transient immunogenicity and low antibody titers, and that immunogenicity had no apparent impact on safety.
Overall, data for the cumulative population treated with IV abatacept support a similar safety profile for SC and IV abatacept, including AEs of particular interest, such as malignancies (incidence rates 0.71 and 0.73, respectively) and autoimmune events (incidence rates 1.37 and 1.99, respectively), based on results of a previously reported integrated analysis of 4,149 patients treated with IV abatacept with up to 7 years of continued exposure (22). A slightly lower rate of serious infections was observed in the population treated with SC abatacept compared with the population treated with IV abatacept (1.79 versus 2.87); this lower rate may be associated with differences in baseline characteristics of the 2 populations. For example, the mean disease duration at baseline was lower in patients who received SC abatacept compared with that in patients who received IV abatacept (7.8 years and 10.1 years, respectively). These findings are also supported by results from the long-term extension phases of several randomized clinical trials (17,18,35), which showed that IV abatacept was well tolerated, with low incidence rates of malignancies, serious infections, and autoimmune events, with no new safety signals over time (22).
Most patients in this integrated analysis had experienced an inadequate response to MTX; however, the ATTUNE (Abatacept in Subjects Who Switch from Intravenous to Subcutaneous Therapy) study included patients in whom prior anti-TNF therapy had failed and who had been receiving long-term treatment (≥4 years) with IV abatacept (26). Overall, safety data for patients treated in the ATTUNE study (n = 123; mean SC abatacept exposure 15.4 months) were consistent with those in the integrated SC abatacept analysis. However, any differences that do exist in the incidence of safety events in the ATTUNE study versus the integrated safety analysis may be related to factors such as longer exposure to abatacept and lower baseline disease activity (based on the Disease Activity Score in 28 joints using the C-reactive protein level [36] and the Health Assessment Questionnaire disability index [37] scores) and fewer tender and swollen joints compared with other abatacept trials.
Only patients who remained in the long-term extensions of these studies were evaluated, which should be noted as a limitation, because events that occurred long after discontinuation will not be captured. However, events that occurred up to 56 days after discontinuation were included in the analysis, a time frame that exceeds the half-life of abatacept at study termination and should therefore capture any event that occurs while abatacept remains in the body. Further observations of the safety of SC abatacept over longer treatment intervals are warranted to confirm that, similar to IV abatacept, no additional, unexpected safety signals will emerge over the long term.
The integrated safety analyses of SC abatacept demonstrate that treatment with the SC formulation is associated with low incidence rates of serious infections, malignancies, and autoimmune events, consistent with observations associated with IV abatacept. Administration of abatacept via the SC route was well tolerated, with low rates of injection site reactions and transient immunogenicity. The safety profile was consistent over time; the frequency of the events of interest did not increase, and there was no occurrence of unexpected/new safety signals with continued exposure. These data support the long-term use of SC abatacept for the treatment of RA.
AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. Dr. Alten had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study conception and design.Alten, Kaine, Keystone, Delaet, Genovese.
Acquisition of data.Alten, Kaine, Keystone, Nash, Delaet, Genovese.
Analysis and interpretation of data.Alten, Kaine, Keystone, Nash, Delaet, Genovese.
ROLE OF THE STUDY SPONSOR
Bristol-Myers Squibb funded the study and reviewed and approved the manuscript prior to submission. The authors had ultimate control over the decision to publish and the final version of the manuscript submitted for publication. Professional medical writing and editorial assistance were provided by Caudex Medical and were funded by Bristol-Myers Squibb.
Acknowledgments
Medical writing and editorial assistance were funded by Bristol-Myers Squibb and were provided by Eve Guichard, BSc (Hons), for Caudex Medical.
REFERENCES
- 1.Goekoop-Ruiterman YP, de Vries-Bouwstra JK, Allaart CF, van Zeben D, Kerstens PJ, Hazes JM. Clinical and radiographic outcomes of four different treatment strategies in patients with early rheumatoid arthritis (the BeSt study): a randomized, controlled trial. Arthritis Rheum. 2005;52:3381–90. doi: 10.1002/art.21405. , et al. [DOI] [PubMed] [Google Scholar]
- 2.Dore RK, Mathews S, Schechtman J, Surbeck W, Mandel D, Patel A. The immunogenicity, safety, and efficacy of etanercept liquid administered once weekly in patients with rheumatoid arthritis. Clin Exp Rheumatol. 2007;25:40–6. , et al. [PubMed] [Google Scholar]
- 3.Bartelds GM, Krieckaert CL, Nurmohamed MT, van Schouwenburg PA, Lems WF, Twisk JW. Development of antidrug antibodies against adalimumab and association with disease activity and treatment failure during long-term follow-up. JAMA. 2011;305:1460–8. doi: 10.1001/jama.2011.406. , et al. [DOI] [PubMed] [Google Scholar]
- 4.Radstake TR, Svenson M, Eijsbouts AM, van den Hoogen FH, Enevold C, van Riel PL. Formation of antibodies against infliximab and adalimumab strongly correlates with functional drug levels and clinical responses in rheumatoid arthritis. Ann Rheum Dis. 2009;68:1739–45. doi: 10.1136/ard.2008.092833. , et al. [DOI] [PubMed] [Google Scholar]
- 5.Curtis JR, Hobar C, Hansbrough K. Injection-site burning and stinging in patients with rheumatoid arthritis using injectable biologics. Curr Med Res Opin. 2011;27:71–8. doi: 10.1185/03007995.2010.534959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Combe B. Early rheumatoid arthritis: strategies for prevention and management. Best Pract Res Clin Rheumatol. 2007;21:27–42. doi: 10.1016/j.berh.2006.08.011. [DOI] [PubMed] [Google Scholar]
- 7.Singh JA, Furst DE, Bharat A, Curtis JR, Kavanaugh AF, Kremer JM. 2012 update of the 2008 American College of Rheumatology recommendations for the use of disease-modifying antirheumatic drugs and biologic agents in the treatment of rheumatoid arthritis. Arthritis Care Res (Hoboken) 2012;64:625–39. doi: 10.1002/acr.21641. , et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yamada A, Salama A, Sayegh M. The role of novel T cell costimulatory pathways in autoimmunity and transplantation. J Am Soc Nephrol. 2002;13:559–75. doi: 10.1681/ASN.V132559. [DOI] [PubMed] [Google Scholar]
- 9.Buch MH, Boyle DL, Rosengren S, Saleem B, Reece RJ, Rhodes LA. Mode of action of abatacept in rheumatoid arthritis patients having failed tumour necrosis factor blockade: a histological, gene expression and dynamic magnetic resonance imaging pilot study. Ann Rheum Dis. 2009;68:1220–7. doi: 10.1136/ard.2008.091876. , et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Genovese MC, Becker JC, Schiff M, Luggen M, Sherrer Y, Kremer J. Abatacept for rheumatoid arthritis refractory to tumor necrosis factor α inhibition. N Engl J Med. 2005;353:1114–23. doi: 10.1056/NEJMoa050524. , et al. [DOI] [PubMed] [Google Scholar]
- 11.Kremer JM, Dougados M, Emery P, Durez P, Sibilia J, Shergy W. Treatment of rheumatoid arthritis with the selective costimulation modulator abatacept: twelve-month results of a phase IIb, double-blind, randomized, placebo-controlled trial. Arthritis Rheum. 2005;52:2263–71. doi: 10.1002/art.21201. , et al. [DOI] [PubMed] [Google Scholar]
- 12.Kremer JM, Genant HK, Moreland LW, Russell AS, Emery P, Abud-Mendoza C. Effects of abatacept in patients with methotrexate-resistant active rheumatoid arthritis: a randomized trial. Ann Intern Med. 2006;144:865–76. doi: 10.7326/0003-4819-144-12-200606200-00003. , et al. [DOI] [PubMed] [Google Scholar]
- 13.Schiff M, Keiserman M, Codding C, Songcharoen S, Berman A, Nayiager S. Efficacy and safety of abatacept or infliximab vs placebo in ATTEST: a phase III, multi-centre, randomised, double-blind, placebo-controlled study in patients with rheumatoid arthritis and an inadequate response to methotrexate. Ann Rheum Dis. 2008;67:1096–103. doi: 10.1136/ard.2007.080002. , et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Schiff M, Pritchard C, Huffstutter JE, Rodriguez-Valverde V, Durez P, Zhou X. The 6-month safety and efficacy of abatacept in patients with rheumatoid arthritis who underwent a washout after anti-tumour necrosis factor therapy or were directly switched to abatacept: the ARRIVE trial. Ann Rheum Dis. 2009;68:1708–14. doi: 10.1136/ard.2008.099218. , et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Weinblatt M, Combe B, Covucci A, Aranda R, Becker JC, Keystone E. Safety of the selective costimulation modulator abatacept in rheumatoid arthritis patients receiving background biologic and nonbiologic disease-modifying antirheumatic drugs: a one-year randomized, placebo-controlled study. Arthritis Rheum. 2006;54:2807–16. doi: 10.1002/art.22070. [DOI] [PubMed] [Google Scholar]
- 16.Weinblatt M, Schiff M, Goldman A, Kremer J, Luggen M, Li T. Selective costimulation modulation using abatacept in patients with active rheumatoid arthritis while receiving etanercept: a randomised clinical trial. Ann Rheum Dis. 2007;66:228–34. doi: 10.1136/ard.2006.055111. , et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kremer JM, Russell AS, Emery P, Abud-Mendoza C, Szechinski J, Westhovens R. Long-term safety, efficacy and inhibition of radiographic progression with abatacept treatment in patients with rheumatoid arthritis and an inadequate response to methotrexate: 3-year results from the AIM trial. Ann Rheum Dis. 2011;70:1826–30. doi: 10.1136/ard.2010.139345. , et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Genovese MC, Schiff M, Luggen M, Le Bars M, Aranda R, Elegbe A. Longterm safety and efficacy of abatacept through 5 years of treatment in patients with rheumatoid arthritis and an inadequate response to tumor necrosis factor inhibitor therapy. J Rheumatol. 2012;39:1546–54. doi: 10.3899/jrheum.111531. , et al. [DOI] [PubMed] [Google Scholar]
- 19.Westhovens R, Kremer JM, Moreland LW, Emery P, Russell AS, Li T. Safety and efficacy of the selective costimulation modulator abatacept in patients with rheumatoid arthritis receiving background methotrexate: a 5-year extended phase IIB study. J Rheumatol. 2009;36:736–42. doi: 10.3899/jrheum.080813. , et al. [DOI] [PubMed] [Google Scholar]
- 20.Gottenberg J, Ravaud P, Bardin T. Prospective follow-up of abatacept treatment in 682 patients with refractory rheumatoid arthritis: tolerance and efficacy data from the French ORA (Orencia and rheumatoid arthritis) registry. Joint Bone Spine. 2009;76:980. [Google Scholar]
- 21.Nusslein H, Alten R, Galeazzi M, Lorenz HM, Boumpas D, Nurmohamed MT. Real-world efficacy and safety of abatacept treatment for RA: 12-month interim analysis of the ACTION study. Arthritis Rheum. 2012;64(Suppl):S199. , et al. [abstract] [Google Scholar]
- 22.Weinblatt ME, Moreland LW, Westhovens R, Cohen RB, Kelly SM, Khan N. Safety of abatacept administered intravenously in treatment of rheumatoid arthritis: integrated analyses of up to 8 years of treatment from the abatacept clinical trial program. J Rheumatol. 2013;40:787–97. doi: 10.3899/jrheum.120906. , et al. [DOI] [PubMed] [Google Scholar]
- 23.Corbo M, Valencia X, Raymond R, Summerill R, Agrawal S, Shergy W. A subcutaneous administration regimen for abatacept in patients with rheumatoid arthritis: pharmacokinetics, safety and immunogenicity. Arthritis Rheum. 2008;(Suppl 58):S307. , et al. [abstract] [Google Scholar]
- 24.Genovese MC, Covarrubias A, Leon G, Mysler E, Keiserman M, Valente R. Subcutaneous abatacept versus intravenous abatacept: a phase IIIb noninferiority study in patients with an inadequate response to methotrexate. Arthritis Rheum. 2011;63:2854–64. doi: 10.1002/art.30463. , et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kaine J, Gladstein G, Strusberg I, Robles M, Louw I, Gujrathi S. Evaluation of abatacept administered subcutaneously in adults with active rheumatoid arthritis: impact of withdrawal and reintroduction on immunogenicity, efficacy and safety (phase IIIb ALLOW study) Ann Rheum Dis. 2012;71:38–44. doi: 10.1136/annrheumdis-2011-200344. , et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Keystone EC, Kremer JM, Russell A, Box J, Abud-Mendoza C, Elizondo MG. Abatacept in subjects who switch from intravenous to subcutaneous therapy: results from the phase IIIb ATTUNE study. Ann Rheum Dis. 2012;71:857–61. doi: 10.1136/annrheumdis-2011-200355. , et al. [DOI] [PubMed] [Google Scholar]
- 27.Nash P, Nayiager S, Genovese M, Rodriguez C, Delaet I, Elegbe A. Low immunogenicity, consistent safety and sustained clinical efficacy over 18 months of subcutaneous administration of abatacept with and without methotrexate in patients with rheumatoid arthritis-results from a phase III study. Ann Rheum Dis. 2010;69:iii97. , et al. [Google Scholar]
- 28.Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31:315–24. doi: 10.1002/art.1780310302. , et al. [DOI] [PubMed] [Google Scholar]
- 29.Hochberg MC, Chang RW, Dwosh I, Lindsey S, Pincus T, Wolfe F. The American College of Rheumatology 1991 revised criteria for the classification of global functional status in rheumatoid arthritis. Arthritis Rheum. 1992;35:498–502. doi: 10.1002/art.1780350502. [DOI] [PubMed] [Google Scholar]
- 30.Genovese MC, Cobos AC, Leon G, Mysler EF, Keiserman MW, Valente RM. Subcutaneous (SC) abatacept (ABA) versus intravenous (IV) ABA in patients (pts) with rheumatoid arthritis: long-term data from the ACQUIRE (Abatacept Comparison of sub[QU]cutaneous versus intravenous in Inadequate Responders to methotrexatE) trial. Arthritis Rheum. 2011;63(Suppl):S150. , et al. [abstract] [Google Scholar]
- 31.Nash P, Nayiager S, Genovese M, Kivitz A, Oelke K, Ludivico C. Immunogenicity is not increased with subcutaneous administration of abatacept with and without methotrexate in patients with rheumatoid arthritis: results from a phase III study. Arthritis Rheum. 2009;60:S633–4. , et al. [Google Scholar]
- 32.Alten R, Kaine J, Keystone E, Nash P, Delaet I, Qi K. Safety of SC abatacept in patients with RA: update from pooled clinical trial data. Ann Rheum Dis. 2012;71:670. , et al. [Google Scholar]
- 33.Salliot C, Dougados M, Gossec L. Risk of serious infections during rituximab, abatacept and anakinra treatments for rheumatoid arthritis: meta-analyses of randomised placebo-controlled trials. Ann Rheum Dis. 2009;68:25–32. doi: 10.1136/ard.2007.083188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kaine J, Gladstein G, Strusberg I, Robles M, Pappu R, Delaet I. Subcutaneous abatacept is effective and well tolerated, with low immunogenicity following temporary withdrawal and re-introduction in the long term extension of the ALLOW trial. Arthritis Rheum. 2011;(Suppl 63):S853. , et al. [abstract] [Google Scholar]
- 35.Westhovens R, Kremer JM, Moreland LW, Emery P, Russell AS, Li T. Safety and efficacy of the selective costimulation modulator abatacept in patients with rheumatoid arthritis receiving background methotrexate: a 5-year extended phase IIB study. J Rheumatol. 2009;36:736–42. doi: 10.3899/jrheum.080813. , et al. [DOI] [PubMed] [Google Scholar]
- 36.Prevoo ML, van 't Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Modified disease activity scores that include twenty-eight–joint counts: development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995;38:44–8. doi: 10.1002/art.1780380107. [DOI] [PubMed] [Google Scholar]
- 37.Fries JF, Spitz P, Kraines RG, Holman HR. Measurement of patient outcome in arthritis. Arthritis Rheum. 1980;23:137–45. doi: 10.1002/art.1780230202. [DOI] [PubMed] [Google Scholar]