

Abstract
Purpose
To report transient corneal edema after phacoemulsification as a predictive factor for the development of pseudophakic cystoid macular edema (PCME).
Methods
A total of 150 eyes from 150 patients (59 men and 91 women; mean age, 68.0 ± 10.15 years) were analyzed using spectral domain optical coherence tomography 1 week and 5 weeks after routine phacoemulsification cataract surgery. Transient corneal edema detected 1 week after surgery was analyzed to reveal any significant relationship with the development of PCME 5 weeks after surgery.
Results
Transient corneal edema developed in 17 (11.3%) of 150 eyes 1 week after surgery. A history of diabetes mellitus was significantly associated with development of transient corneal edema (odds ratio [OR], 4.04; 95% confidence interval [CI], 1.41 to 11.54; p = 0.011). Both diabetes mellitus and transient corneal edema were significantly associated with PCME development 5 weeks after surgery (OR, 4.58; 95% CI, 1.56 to 13.43; p = 0.007; and OR, 6.71; CI, 2.05 to 21.95; p = 0.003, respectively). In the 8 eyes with both diabetes mellitus and transient corneal edema, 4 (50%) developed PCME 5 weeks after surgery.
Conclusions
Transient corneal edema detected 1 week after routine cataract surgery is a predictive factor for development of PCME. Close postoperative observation and intervention is recommended in patients with transient corneal edema.
Keywords: Cataract, Corneal edema, Macular edema, Phacoemulsification, Risk factors
Recent innovations in instruments and surgical techniques have led to improvements in visual outcomes following cataract surgery. Nevertheless, pseudophakic cystoid macular edema (PCME) remains a common cause of unexpected visual deterioration, even after uncomplicated cataract surgery.
The incidence of clinical PCME ranges from 0.1% to 2.35% [1,2,3,4]. However, when including the subclinical level of PCME, which can only be detected by optical coherence tomography (OCT), the incidence increases and ranges from 4% to 11% after routine cataract surgery [5,6]. While most cases of PCME resolve spontaneously, some patients develop permanent visual impairment. The pathogenesis of PCME [1,7] remains uncertain, but previous studies have shown that inflammation is a major risk factor for PCME, leading to breakdown of the blood-aqueous and blood-retinal barriers and increased vascular permeability [1,7].
Transient corneal edema (TCE) with faint folds of Descemet's membrane is a relatively common finding after uncomplicated phacoemulsification cataract surgery, is usually detected in the early postoperative period, and spontaneously resolves in a few weeks. Factors contributing to TCE include previous corneal pathology, age, underlying systemic disease, and surgical trauma [8,9,10,11]. However, it is not rare to find TCE even in eyes without any detectable risk factors. TCE after phacoemulsification usually recovers by one week after surgery [12], but resolution can be delayed [13,14]. The exact etiology of early postoperative TCE is not clear, but it is probably the result of inflammation or endothelial injury during cataract surgery, such as direct mechanical trauma, ultrasound damage, or toxicity from irrigation solution [11,15,16,17]. Several studies have shown that flares and cells in the aqueous humor increase after cataract surgery, which indirectly reflect the degree of inflammation and the function of the blood-aqueous and blood-retinal barriers [18,19].
In this study, we analyzed eyes after uncomplicated phacoemulsification surgery using spectral domain OCT imaging of the cornea and retina. A significant number of eyes with TCE were detected one week after surgery. Further analysis revealed the incidence and risk factors for postoperative TCE and its relationship with PCME.
Materials and Methods
Medical records of patients who underwent uncomplicated cataract surgery between March 2012 and December 2013 at Dongguk University Ilsan Hospital, South Korea, were analyzed retrospectively. The study was approved by the Dongguk University Ilsan Hospital Institutional Review Board. All research adhered to the tenets of the Declaration of Helsinki.
Patients with brunescent cataract, preoperative corneal disease or degeneration, diabetic macular edema or abnormal retinal thickening or cystoid changes shown by baseline OCT exam, a history of uveitis, prior intraocular surgery, or treatment with topical prostaglandins or nonsteroidal anti-inflammatory drugs were not included. Other exclusion criteria were previous complicated (posterior capsule rupture, intraocular lens placement in the sulcus, remnant cortex) cataract surgery and postoperative inflammation or a postoperative intraocular pressure increase requiring additional therapy. One eye per individual was analyzed. In the case of patients who underwent cataract surgery in both eyes, only the right eyes were enrolled.
Surgical technique
All surgery was performed by one surgeon (CYP) using the same surgical techniques. Under topical anesthesia, a corneal paracentesis was made with a 1-mm diamond knife, and a clear corneal incision was made with a 2.8-mm diamond knife. After the anterior chamber was filled with 4% chondroitin sulfate and 3% sodium hyaluronate (Viscoat; Alcon Laboratories, Fort Worth, TX, USA), a continuous curvilinear capsulorhexis of 5 to 5.5 mm was created with a forceps, followed by hydrodissection with balanced salt solution using a hydration cannula. Phacoemulsification was performed with the Stellaris phacoemulsification machine (Bausch and Lomb, Rochester, NY, USA). A phaco chop technique was used with the following parameters: 400-mmHg vacuum, 20% initial power, and 110-cm bottle height. Phacoemulsification power was adjusted depending on the density of the lens nucleus. Automated aspiration of the remaining soft lens matter was set at 500-mmHg vacuum and 110-cm bottle height and was followed by capsule polish with a 15-mmHg vacuum and 80-cm bottle height. A single-piece hydrophobic acrylic intraocular lens (Tecnis IOL; Abbott Medical Optics, Santa Ana, CA, USA) was implanted in the capsular bag with an injector system, and residual viscoelastic material was removed from the anterior chamber. After hydro-sealing of the temporal corneal incision with a balanced salt solution, the anterior chamber was reformed with balanced salt solution.
Outcome parameters
Patients underwent spectral domain OCT examination before, 1 week after, and 5 weeks after cataract surgery. The cornea and macula were measured using a Cirrus HD-OCT (Model 4000, software ver. 6.0; Carl Zeiss Meditec, Dublin, CA, USA). All spectral domain OCT included a 512 × 128 macular cube scan and anterior segment 5-line raster scans. The 512 × 128 macular cube scan produced 128 horizontal scan lines, each comprising 512 A-scans per line, of a 6 mm × 6 mm area. Central subfield retinal thickness (CRT) was automatically measured at the macular center (1-mm-diameter) using a topographic map of the macular cube scan. The anterior segment 5-line raster scans allowed high-resolution imaging of the cornea. The line length was fixed at 3 mm, and each line was composed of 4096 A-scans. The lines were horizontal and separated by 250 µm, so that the five lines together covered a width of 1 mm.
Other preoperatively measured ocular biometric parameters included endothelial cell density and corneal thickness, determined using a Konan Noncon Robo-8400 noncontact specular microscope (Konan Medical, Hyogo, Japan). Anterior chamber angle, depth, and volume were also measured preoperatively using Scheimpflug imaging (Pentacam, ver. 1.17r24; Oculus, Wetzlar, Germany).
TCE was defined as the visible folds of Descemet's membrane by slit lamp examination at the 1-week postoperative visit. The folds were verified by anterior OCT as the presence of a definite wave-like irregular appearance at the posterior corneal surface (anterior segment 5-line raster scans) in every TCE case (Fig. 1). Some corneal edema cases were first diagnosed by OCT and later confirmed by slit lamp re-examination.
Fig. 1.
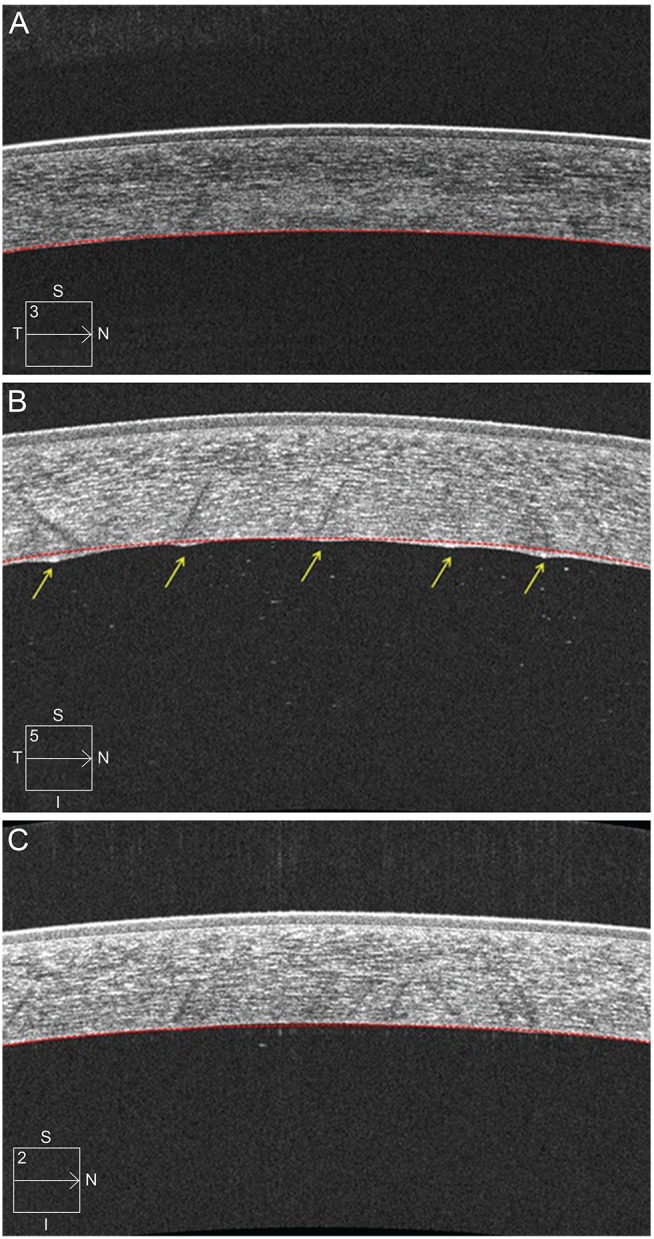
Image of corneal anterior segment 5-line raster scans from an 80-year-old male before and after uncomplicated phacoemulsification surgery. (A) Preoperative anterior optical coherence tomography (OCT) image. The anterior and posterior surfaces of the cornea had a continuous, smooth contour. (B) Anterior OCT of the cornea one week after surgery. The corneal anterior surface had a continuous, smooth contour, while the posterior corneal surface had 5 points of irregular wave-like appearance (arrows) compared to the posterior virtual contour (red colored dotted lines). (C) Anterior OCT of the cornea one month after surgery. All points of the irregular posterior surface resolved and appeared smooth again. I = inferior; N = nasal; S = superior; T = temporal.
PCME was defined based on OCT as an increased CRT of at least 300 µm or the presence of intraretinal cystoid spaces (Fig. 2) [20,21].
Fig. 2.
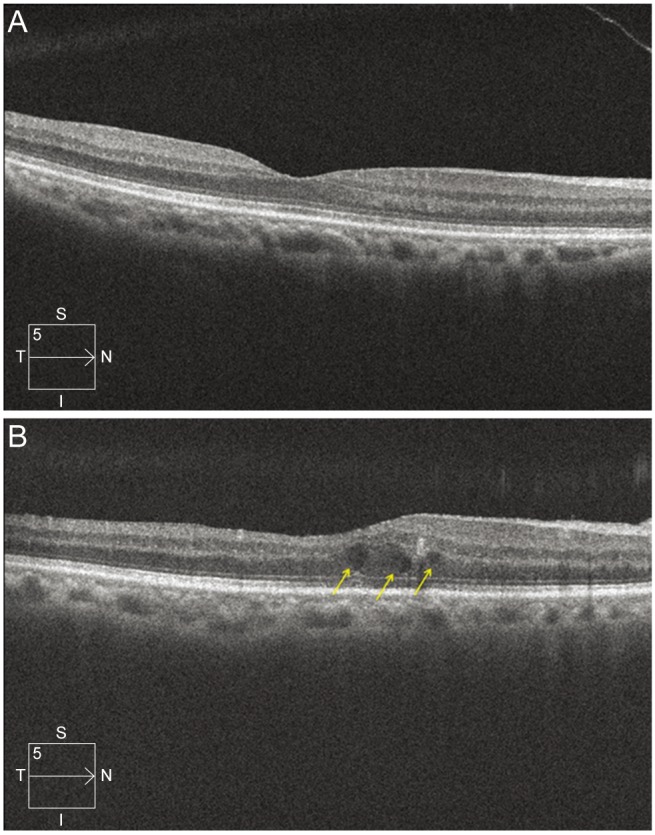
Macular scan image of the same patient in Fig. 1. (A) Preoperative macular cube scan image. The central subfield retinal thickness (CRT) was 267 µm, and the fovea did not show retinal thickening or cystoid change. (B) Image of macular cube scan 1 month after surgery. CRT increased to 324 µm. The normal foveal depression disappeared, and the images show cystoid change at the fovea (arrows). I = inferior; N = nasal; S = superior; T = temporal.
Statistical analysis
All statistical analyses were performed using IBM SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA). The independent t-test or Mann-Whitney U-test was used to compare continuous variables between groups, and chi-square analysis or Fisher's exact test was used to compare categorical variables. Multiple logistic regression analysis was used to evaluate multiple independent variables. A p-value less than 0.05 indicated a significant difference.
Results
A total of 150 eyes from 150 patients (59 men and 91 women) were included in the study. The mean age of the patients was 68.0 ± 10.15 years (range, 42 to 87 years), and there were 106 right eyes and 44 (29%) left eyes.
Postoperative transient corneal edema 1 week after surgery
TCE developed in 17 (11.3%) of 150 eyes 1 week after surgery. The characteristics of the groups with or without corneal edema are shown in Table 1. A history of diabetes mellitus (DM) was significantly associated with development of TCE 1 week after surgery (odds ratio [OR], 4.04; 95% confidence interval [CI], 1.41 to 11.54; p = 0.011). Mean preoperative endothelial cell count and anterior chamber volume were significantly lower in the group with corneal edema (p = 0.037 and p = 0.035, respectively). Other preoperative biometric values and duration of surgery did not differ between the two groups.
Table 1.
Characteristics of patients with or without transient corneal edema on optical coherence tomography
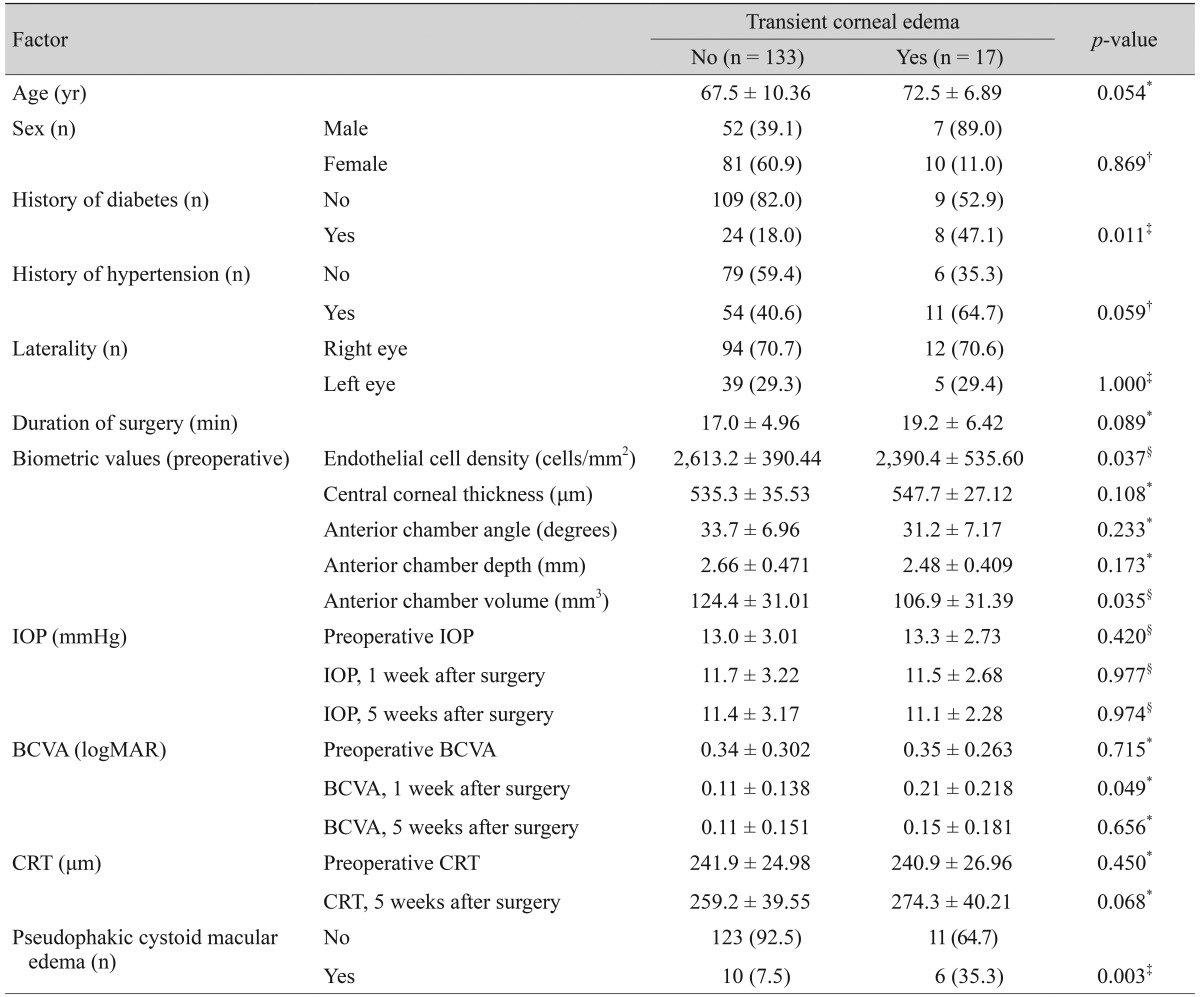
Values are presented as mean ± standard deviation or number (%).
IOP = intraocular pressure; BCVA = best-corrected visual acuity; logMAR = logarithm of the minimum angle of resolution; CRT = central subfield retinal thickness.
*t-test; †Chi-square analysis; ‡Fisher's exact test; §Mann-Whitney U-test.
The mean best-corrected visual acuity (BCVA) measured 1 week after surgery was worse in eyes with TCE (p = 0.049). However, this difference disappeared 5 weeks after surgery, with resolution of corneal edema. CRT did not differ between the two groups when measured 1 week and 5 weeks after surgery. Among the 17 eyes with TCE at 1 week, 2 (11.8%) demonstrated continued edematous morphologic changes on OCT through 5 weeks after surgery. In these two eyes, OCT at 3 months after surgery revealed resolution of edematous morphologic changes.
Among the 17 eyes with TCE at 1 week, 6 (35.3%) developed PCME on OCT 5 weeks after surgery. The incidence of PCME in the group with corneal edema (35.3%) was higher compared to the group without corneal edema (7.5%). TCE was significantly associated with PCME development 5 weeks after surgery (OR, 6.71; 95% CI, 2.05 to 21.95; p = 0.003).
Pseudophakic cystoid macular edema 5 weeks after surgery
OCT revealed development of PCME in 16 (10.7%) of 150 eyes 5 weeks after surgery. The characteristics of the groups with or without PCME are shown in Table 2. Age, sex, history of hypertension, laterality, preoperative BCVA, preoperative biometric values, and duration of surgery did not differ between the two groups; however, a history of DM was associated with development of PCME 5 weeks after the surgery (OR, 4.58; 95% CI, 1.56 to 13.43; p = 0.007). The mean postoperative CRT measured 5 weeks after surgery was thicker in eyes with PCME than in eyes without PCME (p = 0.001). TCE was more frequently found in eyes with PCME (p = 0.003); TCE was found in 8.2% of eyes without PCME but in 35.3% of eyes with PCME. A history of DM (OR, 2.254; p = 0.001) or TCE (OR, 3.284; p = 0.020) was significantly associated with PCME development on univariate analysis of logistic regression, while multivariate logistic regression analysis revealed only TCE to be significantly associated with PCME development (Table 3). Eight eyes were positive for both DM and TCE. Of these, four (50%) eyes developed PCME 5 weeks after surgery.
Table 2.
Characteristics of patients with or without PCME on optical coherence tomography
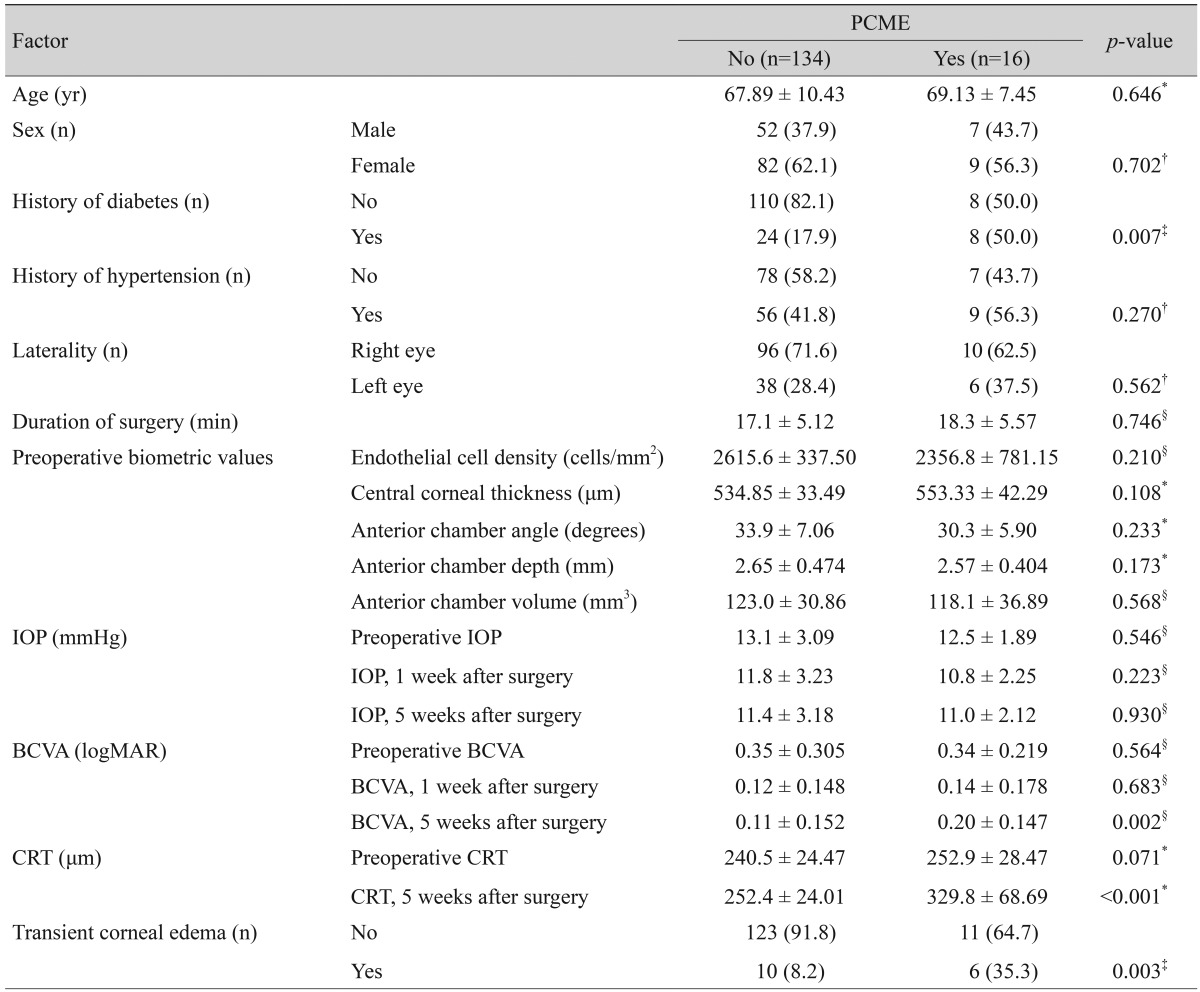
Values are presented as mean ± standard deviation or number (%).
PCME = pseudophakic cystoid macular edema; IOP = intraocular pressure; BCVA = best-corrected visual acuity; logMAR = logarithm of the minimum angle of resolution; CRT = central subfield retinal thickness.
*t-test; †Chi-square analysis; ‡Fisher's exact test; §Mann-Whitney U-test.
Table 3.
Univariate and multivariate analyses of the associations between all baseline parameters and pseudophakic cystoid macular edema on optical coherence tomography
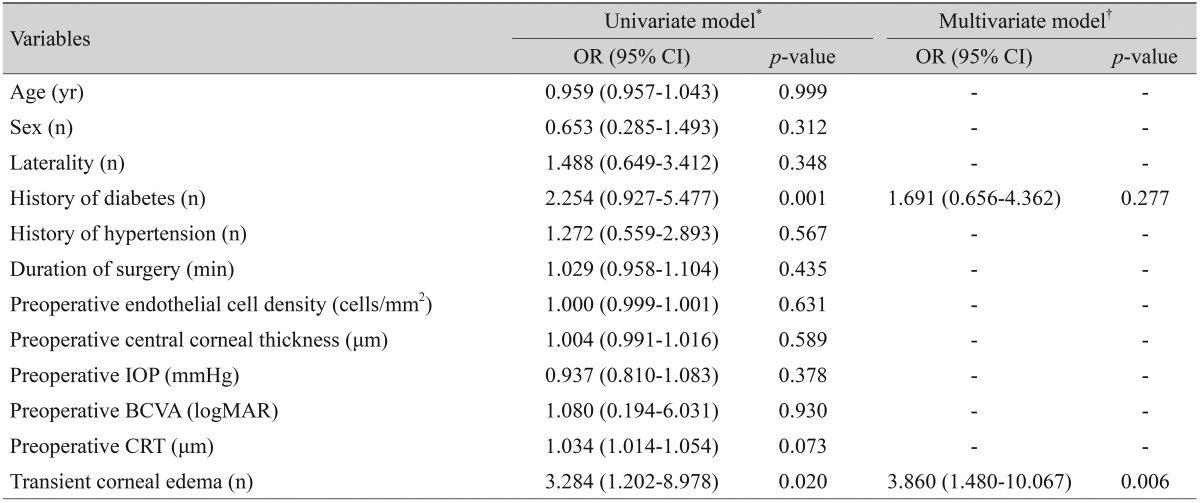
*Univariate model including each variable independently; †Stepwise multivariate model including baseline parameters along with other clinical variables.
OR = odds ratio; CI = confidence interval; IOP = intraocular pressure; BCVA = best-corrected visual acuity; logMAR = logarithm of the minimum angle of resolution; CRT = central subfield retinal thickness.
Discussion
In this study, we found that early postoperative TCE can be detected using OCT 1 week after surgery, and that the incidence is relatively common (11.3%), even after uncomplicated cataract surgery. Diabetes is a strong risk factor for corneal edema, with an OR of 4.04, as is PCME, with an OR of 6.71. We also found that the presence of TCE 1 week after surgery increased the risk of PCME 5 weeks after surgery, with an OR of 4.463. The presence of both DM and TCE resulted in a high incidence (50%) of PCME 5 weeks after surgery.
Postoperative TCE is usually subclinical and may deteriorate visual acuity by one or two lines. This was demonstrated in our study, as the BCVA in eyes with corneal edema 1 week after surgery showed slightly lower visual acuity compared to eyes without corneal edema. However, there was no statistically significant difference 5 weeks after surgery. It has been shown that the eyes with corneal edema early after cataract surgery have irregular wave-like posterior corneal surfaces on spectral domain OCT, and the majority of eyes with corneal edema recovered within 1 week of surgery [12]; however, we found a significant number of eyes with TCE even 1 week after surgery.
Previously, Tao et al. [12] reported that eyes with corneal edema after cataract surgery had an irregular wave-like posterior surface on OCT, and the majority of the eyes with corneal edema recovered within 1 week of surgery. In the present study, we verified all TCE using spectral domain OCT and demonstrated that Descemet's fold according to slit lamp exam was equal to the presence of spikes on anterior OCT. Four of 17 cases of corneal edema missed on the first slit lamp exam were later diagnosed by OCT; however, all 4 cases of corneal edema were confirmed by slit lamp exam.
Similar to previous studies, the eyes in subjects with DM have a higher risk of developing PCME. In this study, the incidence of PCME 5 weeks after surgery was 10.7%, and the incidence of PCME in patients with DM was 25%. This result is consistent with the incidences of OCT-proven PCME (4% to 11%) and the incidence of OCT-proven PCME in diabetic patients (22%) reported previously [5,6,21,22]. DM also increased the incidence of corneal edema after cataract surgery. Antcliff et al. [23] reported an increased incidence of TCE after cataract surgery in patients with DM. Morikubo et al. [24] reported that corneal endothelial cell losses 1 week after cataract surgery were significantly greater in patients with DM.
It is interesting that eyes with TCE 1 week after surgery had a higher incidence of PCME 5 weeks after surgery. The relationship between TCE and development of PCME suggests that TCE and PCME may partly share the same etiologies of inf lammation, breakdown of the blood-aqueous and blood-retinal barriers, and increased vascular permeability [1,7,18,19].
Recent analyses confirmed that topical nonsteroidal anti-inflammatory drugs and steroids are effective in preventing and treating postoperative inflammation and can reduce the incidence of PCME [25,26,27]. However, these drugs have well-known side effects with long-term use. Therefore, it is necessary to select eyes with high risk factors for PCME and treat them efficiently. Several previous studies have reported that the increased incidence of postoperative CME is associated with a history of uveitis, preoperative prostaglandin use, history of diabetes, and complicated cataract surgery [1,3,21,22]. However, not all cases of PCME can be explained by the previously reported risk factors. Therefore, studies to identify new risk factors are highly recommended.
In this study, we controlled for several variables to discover new predictive factors for PCME development after uncomplicated cataract surgery; endothelial cell density, central corneal thickness, and preoperative CRT were not associated with PCME development. Several studies have reported that the incidence of PCME after cataract surgery increased in older patients; however, age was not associated with PCME development in the present study [28,29]. This may be explained by the fact that we excluded patients with brunescent cataracts, retinal diseases, or a history of intraocular surgery.
Our study has several limitations. Nuclear density and cumulative ultrasound energy may affect the incidence of corneal edema or PCME after surgery; however, we were not able to analyze cataract density or accurate cumulative ultrasound energy because of the retrospective study design. In this study, we only analyzed OCT obtained 5 weeks after surgery, and thereby late onset PCME might have been missed. In addition, we examined corneas with OCT 1 week after surgery; therefore, any cases of TCE resolving before this time were not accounted for in the cases of TCE. This may have led to underestimation of the incidence of TCE; Tao et al. [12] reported that 50% of patients developed corneal edema one day after cataract surgery, and Shakya et al. [30] reported a 29.2% incidence one day after surgery. In the present study, we only used one viscoelastic during surgery. Therefore, we could not compare the effect of different viscoelastics on TCE and PCME development.
In conclusion, TCE detected by slit lamp exam 1 week after surgery was significantly associated with the development of PCME 5 weeks after surgery. By combining both history of DM and history of TCE, the development of PCME was correctly predicted in 50% of the patients in this study. Therefore, close observation and active intervention are strongly recommended in diabetic eyes with TCE in order to prevent the development of PCME.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Flach AJ. The incidence, pathogenesis and treatment of cystoid macular edema following cataract surgery. Trans Am Ophthalmol Soc. 1998;96:557–634. [PMC free article] [PubMed] [Google Scholar]
- 2.Halpern DL, Pasquale LR. Cystoid macular edema in aphakia and pseudophakia after use of prostaglandin analogs. Semin Ophthalmol. 2002;17:181–186. doi: 10.1076/soph.17.3.181.14789. [DOI] [PubMed] [Google Scholar]
- 3.Henderson BA, Kim JY, Ament CS, et al. Clinical pseudophakic cystoid macular edema: risk factors for development and duration after treatment. J Cataract Refract Surg. 2007;33:1550–1558. doi: 10.1016/j.jcrs.2007.05.013. [DOI] [PubMed] [Google Scholar]
- 4.Loewenstein A, Zur D. Postsurgical cystoid macular edema. Dev Ophthalmol. 2010;47:148–159. doi: 10.1159/000320078. [DOI] [PubMed] [Google Scholar]
- 5.Belair ML, Kim SJ, Thorne JE, et al. Incidence of cystoid macular edema after cataract surgery in patients with and without uveitis using optical coherence tomography. Am J Ophthalmol. 2009;148:128–135. doi: 10.1016/j.ajo.2009.02.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Perente I, Utine CA, Ozturker C, et al. Evaluation of macular changes after uncomplicated phacoemulsification surgery by optical coherence tomography. Curr Eye Res. 2007;32:241–247. doi: 10.1080/02713680601160610. [DOI] [PubMed] [Google Scholar]
- 7.Benitah NR, Arroyo JG. Pseudophakic cystoid macular edema. Int Ophthalmol Clin. 2010;50:139–153. doi: 10.1097/IIO.0b013e3181c551da. [DOI] [PubMed] [Google Scholar]
- 8.Setala K. Corneal endothelial cell density in iridocyclitis. Acta Ophthalmol. 1979;57:277–286. doi: 10.1111/j.1755-3768.1979.tb00492.x. [DOI] [PubMed] [Google Scholar]
- 9.Weston BC, Bourne WM, Polse KA, Hodge DO. Corneal hydration control in diabetes mellitus. Invest Ophthalmol Vis Sci. 1995;36:586–595. [PubMed] [Google Scholar]
- 10.O'sNeal MR, Polse KA. Decreased endothelial pump function with aging. Invest Ophthalmol Vis Sci. 1986;27:457–463. [PubMed] [Google Scholar]
- 11.Glasser DB, Schultz RO, Hyndiuk RA. The role of viscoelastics, cannulas, and irrigating solution additives in post-cataract surgery corneal edema: a brief review. Lens Eye Toxic Res. 1992;9:351–359. [PubMed] [Google Scholar]
- 12.Tao A, Chen Z, Shao Y, et al. Phacoemulsification induced transient swelling of corneal Descemet's Endothelium Complex imaged with ultra-high resolution optical coherence tomography. PLoS One. 2013;8:e80986. doi: 10.1371/journal.pone.0080986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Behndig A, Lundberg B. Transient corneal edema after phacoemulsification: comparison of 3 viscoelastic regimens. J Cataract Refract Surg. 2002;28:1551–1556. doi: 10.1016/s0886-3350(01)01219-6. [DOI] [PubMed] [Google Scholar]
- 14.Li YJ, Kim HJ, Joo CK. Early changes in corneal edema following torsional phacoemulsification using anterior segment optical coherence tomography and Scheimpflug photography. Jpn J Ophthalmol. 2011;55:196–204. doi: 10.1007/s10384-011-0007-5. [DOI] [PubMed] [Google Scholar]
- 15.Zetterstrom C, Laurell CG. Comparison of endothelial cell loss and phacoemulsification energy during endocapsular phacoemulsification surgery. J Cataract Refract Surg. 1995;21:55–58. doi: 10.1016/s0886-3350(13)80480-4. [DOI] [PubMed] [Google Scholar]
- 16.Hayashi K, Nakao F, Hayashi F. Corneal endothelial cell loss following phacoemulsification using the Small-Port Phaco. Ophthalmic Surg. 1994;25:510–513. [PubMed] [Google Scholar]
- 17.Kosrirukvongs P, Slade SG, Berkeley RG. Corneal endothelial changes after divide and conquer versus chip and flip phacoemulsification. J Cataract Refract Surg. 1997;23:1006–1012. doi: 10.1016/s0886-3350(97)80072-7. [DOI] [PubMed] [Google Scholar]
- 18.Ersoy L, Caramoy A, Ristau T, et al. Aqueous flare is increased in patients with clinically significant cystoid macular oedema after cataract surgery. Br J Ophthalmol. 2013;97:862–865. doi: 10.1136/bjophthalmol-2012-302995. [DOI] [PubMed] [Google Scholar]
- 19.Shah SM, Spalton DJ. Changes in anterior chamber flare and cells following cataract surgery. Br J Ophthalmol. 1994;78:91–94. doi: 10.1136/bjo.78.2.91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Oh JH, Chuck RS, Do JR, Park CY. Vitreous hyper-reflective dots in optical coherence tomography and cystoid macular edema after uneventful phacoemulsification surgery. PLoS One. 2014;9:e95066. doi: 10.1371/journal.pone.0095066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yonekawa Y, Kim IK. Pseudophakic cystoid macular edema. Curr Opin Ophthalmol. 2012;23:26–32. doi: 10.1097/ICU.0b013e32834cd5f8. [DOI] [PubMed] [Google Scholar]
- 22.Schmier JK, Halpern MT, Covert DW, Matthews GP. Evaluation of costs for cystoid macular edema among patients after cataract surgery. Retina. 2007;27:621–628. doi: 10.1097/01.iae.0000249577.92800.c0. [DOI] [PubMed] [Google Scholar]
- 23.Antcliff RJ, Poulson A, Flanagan DW. Phacoemulsification in diabetics. Eye (Lond) 1996;10:737–741. doi: 10.1038/eye.1996.171. [DOI] [PubMed] [Google Scholar]
- 24.Morikubo S, Takamura Y, Kubo E, et al. Corneal changes after small-incision cataract surgery in patients with diabetes mellitus. Arch Ophthalmol. 2004;122:966–969. doi: 10.1001/archopht.122.7.966. [DOI] [PubMed] [Google Scholar]
- 25.Hariprasad SM, Callanan D, Gainey S, et al. Cystoid and diabetic macular edema treated with nepafenac 0.1% J Ocul Pharmacol Ther. 2007;23:585–590. doi: 10.1089/jop.2007.0062. [DOI] [PubMed] [Google Scholar]
- 26.Wolf EJ, Braunstein A, Shih C, Braunstein RE. Incidence of visually significant pseudophakic macular edema after uneventful phacoemulsification in patients treated with nepafenac. J Cataract Refract Surg. 2007;33:1546–1549. doi: 10.1016/j.jcrs.2007.05.018. [DOI] [PubMed] [Google Scholar]
- 27.Miyake K, Ota I, Miyake G, Numaga J. Nepafenac 0.1% versus fluorometholone 0.1% for preventing cystoid macular edema after cataract surgery. J Cataract Refract Surg. 2011;37:1581–1588. doi: 10.1016/j.jcrs.2011.03.052. [DOI] [PubMed] [Google Scholar]
- 28.Stern AL, Taylor DM, Dalburg LA, Cosentino RT. Pseudophakic cystoid maculopathy: a study of 50 cases. Ophthalmology. 1981;88:942–946. doi: 10.1016/s0161-6420(81)80009-7. [DOI] [PubMed] [Google Scholar]
- 29.Rossetti L, Autelitano A. Cystoid macular edema following cataract surgery. Curr Opin Ophthalmol. 2000;11:65–72. doi: 10.1097/00055735-200002000-00010. [DOI] [PubMed] [Google Scholar]
- 30.Shakya K, Pokharel S, Karki KJ, et al. Corneal edema after phacoemulsification surgery in patients with type II diabetes mellitus. Nepal J Ophthalmol. 2013;5:230–234. doi: 10.3126/nepjoph.v5i2.8734. [DOI] [PubMed] [Google Scholar]