

Abstract
BACKGROUND: Diabetes is a chronic, potentially debilitating, and often fatal disease. Dietary strategies to reduce postprandial glycemia are important in the prevention and treatment of diabetes. Nuts are rich in mono- and polyunsaturated fatty acids, which may reduce hyperglycemia and improve metabolism. OBJECTIVES: To evaluate the effectiveness of pistachio nut supplementation on glycemic and inflammatory measures in patients with type 2 diabetes. METHODS: In this double-blind, randomized, placebo-controlled, crossover trial, 48 diabetic patients were equally assigned to groups A and B. Patients in group A received a snack of 25 g pistachio nuts twice a day for 12 weeks and group B received a control meal without nuts. After 12 weeks of intervention, the patients had an 8-week washout. Then the groups were displaced, and group B received the same amount of pistachios for 12 weeks. RESULTS: With respect to the total change in variables over both phases, there was a marked decrease in HbA1c (-0.4%) and fasting blood glucose (FBG) concentrations (-16 mg/dl) in the pistachio group compared with the control group (p ≤ 0.001 for both). There was no overall significant change in BMI, blood pressure, HOMA-IR, and C-reactive protein (CRP) concentrations. Analysis of the two phases separately showed a decrease in FBG by 14 mg/dl and in HbA1c by 0.45% in the treatment group (A) after 12 weeks, while no significant differences were seen in group B (control group). In the second phase, FBG decreased from 151.36 ± 39.22 to 137.28 ± 28.65 mg/dl (-14 mg/dl) and HbA1c decreased from 7.42 ± 0.97 to 7.15 ± 0.68 mg/dl (-0.28%, p = 0.013 and p = 0.033, respectively) in the pistachio group (B). Pistachio consumption reduced systolic blood pressure (p = 0.007), BMI (p = 0.011), and CRP (p = 0.002) in patients from the treatment groups, but not insulin resistance. CONCLUSIONS: Dietary consumption of pistachio nuts as a snack has beneficial effects on glycemic control, blood pressure, obesity, and inflammation markers in diabetic patients.
Keywords: type 2 diabetes, pistachio nut, blood glucose, HbA1c, antiglycemic, antiobese
Abbreviations: ALT - alanine aminotransferase; AST - aspartate aminotransferase; BMI - body mass index; BP - blood pressure; CI - confidence interval; CV - coefficient of variation; CRP - C-reactive protein; FBG - fasting blood glucose; GLP-1 - glucagon-like peptide-1; HbA1c - glycosylated hemoglobin A1; HOMA-IR - homeostasis model assessment of insulin resistance; IL - interleukin; mmHg - millimeters of mercury; OGTT - oral glucose tolerance test; SPSS - Statistics Package for Social Sciences; TNF - tumor necrosis factor
1. Introduction
Diet is an important factor in controlling diabetes. The incidence of insulin resistance and therefore diabetes is lowered with diets higher in monounsaturated fats and lower in saturated fats. Also, monounsaturated fatty acids are supposed to reduce inflammation [1], and monounsaturated fatty acids may reduce adiposity [2]. Conflicting evidence exists on the role of polyunsaturated fatty acids in diabetes.
Nuts are rich in mono- and polyunsaturated fats (70-80%) [3], which are essential for a healthy diet. The consumption of nuts has been shown to reduce the risk of type 2 diabetes by 27% [4]. Pistachio (Pistacia vera L.) is a member of the Anacardiaceae family, which is native to arid zones of Central and West Asia, and distributed throughout the Mediterranean basin [5]. Pistachio nuts are mainly consumed as a snack; they are considered as a rich source of phenolic compounds, which have recently been ranked among the first 50 food resources with antioxidant activity [6]. Nuts are sources of unsaturated fats that alter the phospholipids in cell membranes, vitamins, minerals, fiber, magnesium, and selenium, all of which can improve insulin sensitivity and glucose homeostasis [7-9]. Also, nuts may reduce blood pressure (BP) and peripheral vascular resistance [10]. In particular, pistachios can improve lipid profiles in subjects with moderate hypercholesterolemia [11].
Randomized clinical trials found that patients consuming a pistachio-supplemented diet show significantly decreased postprandial glycemia, insulin, fasting glucose, and HOMA-IR, and increased GLP-1 [12, 13]. Based on these considerations, nuts may potentially improve glycemic control and reduce inflammatory factors in diabetic patients. However, there is little evidence for the efficacy of pistachio on glycemic control of diabetic patients [12-14]. Therefore, this study was designed to investigate the effectiveness of pistachio consumption on blood glucose of type 2 diabetic patients in a crossover clinical trial.
2. Methods
2.1. Subjects
This was a single-blind, randomized, case-control, crossover clinical trial, carried out in Shahid Beheshti Hospital of Qom, Iran, in the period between February 2012 and March 2013. The Ethics Committee of Qom University of Medical Sciences approved the study protocol. Forty-eight patients with type 2 diabetes met the inclusion criteria, and were enrolled in the study after obtaining written informed consent. Inclusion criteria were as follows: diabetes duration for at least one year, treatment with oral hypoglycemic agents, and serum creatinine levels and liver function tests within the normal range. Exclusion criteria included multivitamin supplementation consumption within one month prior to study start, pregnancy or pregnancy planning, and heart failure based on clinical examination.
After enrollment, demographic data were recorded, and the patients were asked not to alter their previous diet and physical activity during the study. Then, patients were examined and blood pressure (BP) was measured. Patients rested in the sit¬ting position for at least five minutes before BP measurement, which was done twice at ten-minute inter¬vals [15]. BP was measured in both arms using a mercury sphygmomanometer; the higher value was recorded [16].
Body mass index (BMI) was calculated by using the metric BMI formula (kg/m2) [17]. On the next day, fasting blood was obtained to measure fasting plasma glu¬cose, liver function tests including serum AST and ALT, serum creatinine, C-reactive protein (CRP), and insulin level. Patients with normal creatinine and liver function tests were included in the study.
After the determination of clinical parameters, the patients were visited by a nutritionist and endocrinologist, and subsequently referred to a third person for randomization. We used block randomization to randomly assign participants to groups. A block was defined as an elementary group from which participants were further assigned to study groups A and B. In this procedure, we acted as follows:
- We set up 6 blocks.
- Each block consisted of four different states, including two times A and two times B.
- In general, 4 patients were each assigned to a block.
- Practically, half of the patients within each block went to group A, and the other half to group B.
- The patients were partitioned randomly from the blocks using random numbers.
The order of patients was random. Therefore, there were 6 possible ways to equally assign participants to a block. The next step was to select patients randomly amongst the 12 blocks consisting of four participants each, and assign them to group A or B. The allocation of patients to groups was performed using random numbers for the participants.
The patients in group A received 2 snacks of 25 g pistachios per day for 12 weeks beside consuming morning and evening servings (case group). The patients in group B received their previous diet without pistachios and routine physical activity during 12 weeks (control group). In this way, half of the patients (group A) received 50 g pistachios, and the other half (group B) did not receive pistachios. Four weeks after initiation, patients were visited and their degree of compliance was determined. After 12 weeks, at the end of the first phase of the study, all laboratory tests and clinical evaluations were repeated, as in the initial visit.
The second phase of the study was started after an 8-week wash-out period. In this phase, the groups were crossed over, so that the patients in group B received 50 g pistachio per day, and those in group A acted as controls. Then, the protocol was repeated as in the first phase. Four patients withdrew from the study (one in group A and three in group B). Two patients started insulin therapy (one in each group), and were excluded from the study. Two patients were withdrawn because of poor compliance with the study protocol. Overall, 44 patients completed the study (23 in group A and 21 in group B). The study protocol is displayed in Figure 1.
Figure 1.
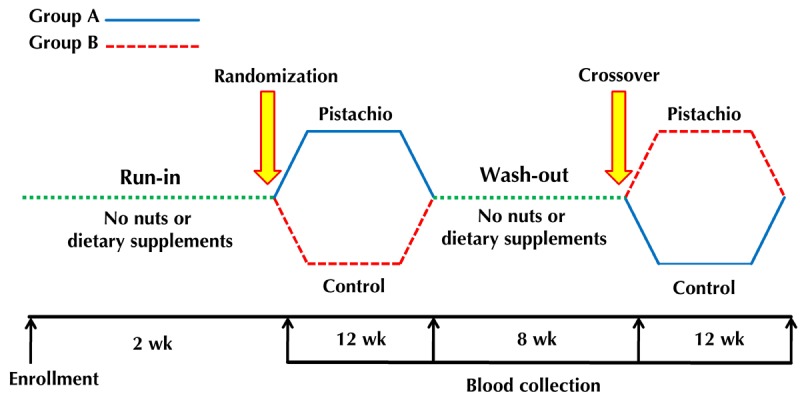
Flow chart of study protocol.
2.2. Biochemical analysis
After 12 hours of fasting, blood samples were collected from all patients at 8 am. The blood samples were stored at -70°C in Shahid Beheshti Hospital of Qom’s laboratory and assayed at the end of the study. Fasting plasma glucose was measured by the enzymatic method; the intra- and inter-assay coefficients of variation (CV) were 1.5% and 0.91%, respectively. HbA1c was measured by chromatography, with intra- and inter-assay CV of 5.8% and 6.7%, respectively. Serum insulin was assessed by ELISA (DiaMetra Co, Italy). The HOMA-IR value was calculated by multiplication of the fasting glucose value (mg/dl) by the serum insulin value (μIU/ml( in each person divided by 405 [18].
2.3. Statistical analysis
At first, the Kolmogorov-Smirnov test was performed to assess normality of the variables. Blood pressure, HOMA-IR, and CRP were not normally distributed. Therefore, they were log-transformed. The paired t-test was used to compare the data between the pistachio and control group. Chi-square test was used to compare qualitative variables. Data are presented as mean ± SD for normally distributed variables and median (25th, 75th percentile) for non-normal data (BP, HOMA-IR, and CRP). P-values less than 0.05 were considered statistically significant. The statistical analysis was performed by SPSS version 17.0.
3. Results
Forty-eight diabetic patients met the inclusion criteria and were enrolled in the study. Overall, 44 patients completed the study. The demographic data and comparisons of the metabolic profiles are summarized in Tables 1 and 2. There was no significant difference between the two groups at baseline.
Table 1. Demographic characteristics of the two groups of type 2 diabetic patients.
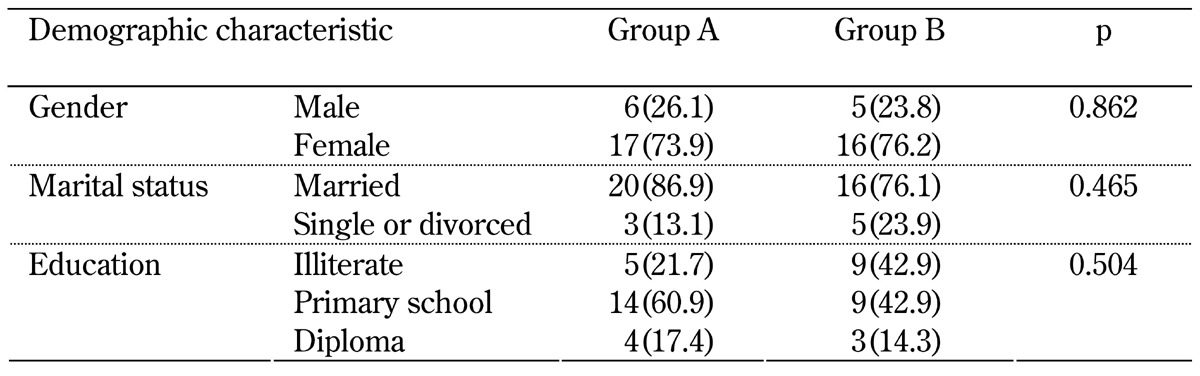
Legend: Data are number (percent).
Table 2. Baseline demographic characteristics and biochemical and clinical characteristics of the two groups of type 2 diabetic patients.
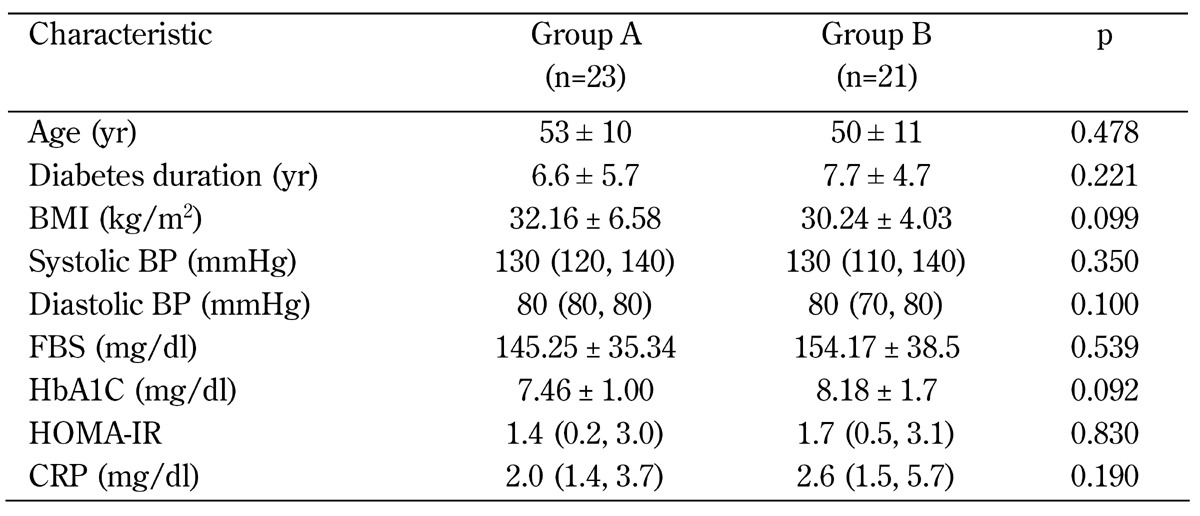
Legend: Data are mean ± SD (for the normally distributed variables) or median (25th, 75th percentile) for the variables not distributed normally. Abbreviations: BMI – body mass index; BP – blood pressure; FBS – fasting blood sugar; HbA1c – glycosylated hemoglobin; HOMA-IR – homeostasis model assessment of insulin resistance; CRP – C-reactive protein.
3.1 Total effects over both phases
At first, we calculated the overall effect of pistachio supplementation on study end-points. We compared the average changes in glycemic and other variables over both phases, and found that subjects randomized to pistachio showed a marked decrease in their HbA1c (-0.4%) and FBG (-16 mg/dl) concentrations (Table 3). Also, there was a trend towards a decrease in BMI. Blood pressure, HOMA-IR, and CRP concentrations showed no significant changes.
Table 3. Total effects of pistachio and control diet on study end-points over both phases.
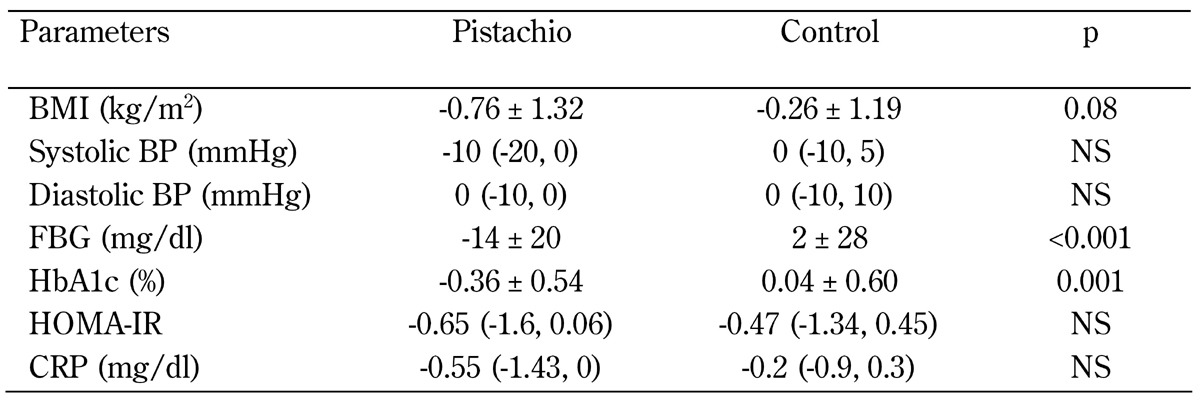
Legend: Data are mean ± SD (for the normally distributed variables) or median (25th, 75th percentile) for the variables not distributed normally. Abbreviations: BMI – body mass index; BP – blood pressure; FBS – fasting blood sugar; HbA1c – glycosylated hemoglobin; HOMA-IR – homeostasis model assessment of insulin resistance; CRP – C-reactive protein.
3.2. Effects in the first and second phase separately
In the first phase, pistachio nuts were given to patients in group A; group B received a control diet. At the end of phase 1, FBG and HbA1c values were decreased significantly in group A (p < 0.005), while there was no significant change in group B (Table 4). At the end of the wash-out period, mean FBG in group A had increased again (150.78 ± 43.69 mg/dl) to almost baseline level (154.17 ± 38.5 mg/dl). This increase was significantly different from FBG concentrations observed directly after the first phase (140.21 ± 34.5, p = 0.03), showing that the antiglycemic effect of pistachios was present during supplementation only (Tables 4 and 5). The beneficial effect was more prolonged for HbA1c values, which were significantly reduced after the first phase (-0.45%, p < 0.001), and reduced again at the end of the wash-out period, albeit slightly (-0.06%). At the end of the second phase, FBG and HbA1c levels in group B had decreased on pistachio consumption similar to phase 1 in group A. FBG and HbA1c values in the control group increased after 12 weeks, but the increase was not statistically significant (Table 5). This increase in phase 2 represents the persistent return to normal glycemic values even after wash-out, and may be a result of the prolonged antidiabetic effect of pistachio consumption.
Table 4. Comparison of the two groups of type 2 diabetic patients in the first phase.
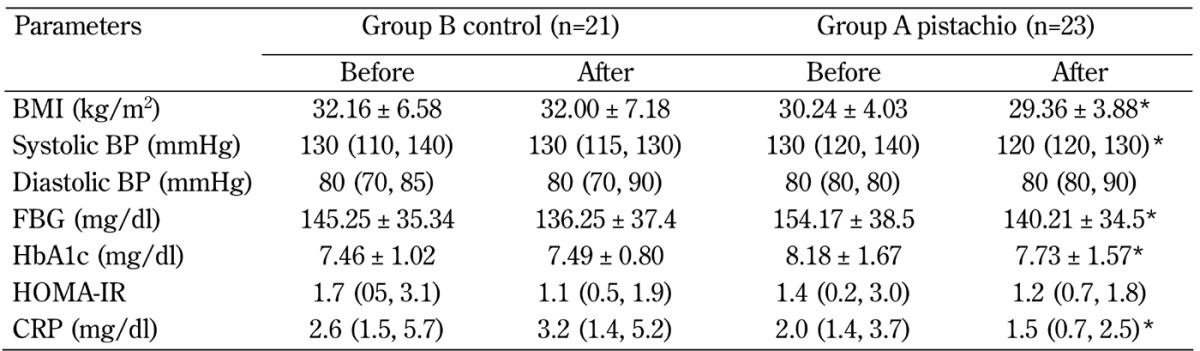
Legend: Data are mean ± SD (for the normally distributed variables) or median (25th, 75th percentile) for the variables not distributed normally. * p < 0.05. Abbreviations: BMI – body mass index; BP – blood pressure; FBS – fasting blood sugar; HbA1c – glycosylated hemoglobin; HOMA-IR – homeostasis model assessment of insulin resistance; CRP – C-reactive protein.
Table 5. Comparison of the two groups of type 2 diabetic patients in the second phase.
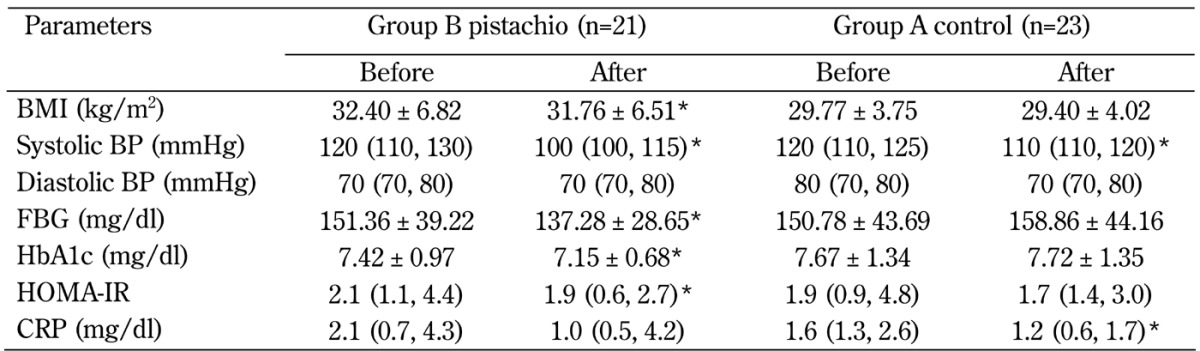
Legend: Data are mean ± SD (for the normally distributed variables) or median (25th, 75th percentile) for the variables not distributed normally. * p < 0.05. Abbreviations: BMI – body mass index; BP – blood pressure; FBS – fasting blood sugar; HbA1c – glycosylated hemoglobin; HOMA-IR – homeostasis model assessment of insulin resistance; CRP – C-reactive protein.
In the first phase, the BMI in group-A patients decreased significantly (p = 0.011, 95% CI: 0.22-1.54). Patients in group B, who did not receive the pistachios, showed no change in BMI (Table 4). In the second phase, mean BMI decreased significantly in group-B patients, who received pistachios (p = 0.015, 95% CI: 0.13-1.13), while no difference in BMI values was found in group A, which acted as control group (Table 5). As for glycemic parameters, the positive effect of pistachio consumption on BMI also seems to be preserved beyond the wash-out period of 8 weeks, as (after the reduction of 0.88 kg/m2 in phase 1) another reduction was seen in group-A patients, who did not receive pistachio supplementation in phase 2 (-0.37 kg/m2), although there was an increase during the wash-out period.
In both groups, systolic blood pressure decreased during pistachio consumption (group A: p = 0.007; group B in the second phase: p = 0.001). There was no significant effect on diastolic blood pressure (Tables 4 and 5). In the phase-2 but not phase-1 control group, the variation in systolic blood pressure was statistically significant (p = 0.044) (Tables 4 and 5). This points again to a sustained effect of pistachio consumption, indicating that the wash-out period may have been too short.
The effects of pistachio consumption on insulin resistance and CRP were inconclusive. While the reductions were significant in the treatment groups (except for HOMA-IR), patients in the phase-2 control group also showed significant reductions in CRP concentrations (p = 0.023) (Tables 4 and 5). In analogy to the effect on systolic blood pressure, pistachio consumption also showed a prolonged effect on CRP throughout the wash-out period and across the study phases. The effect seems to be sustainable over a long period even after discontinuation of pistachio supplementation.
4. Discussion
Diabetes mellitus is a chronic disease that affects about 5-10% of the world population [4, 19]. Diet and weight control are the basic principles in the treatment of type 2 diabetes. Nuts contain magnesium and monounsaturated and polyunsaturated fats, which are supposed to improve insulin sensitivity, carbohydrate metabolism, and insulin homeostasis [20]. In a study investigating the effects of nuts on diabetic patients, Jiang et al. showed that the relative risk of developing diabetes was reduced by 27% in women who consumed nuts for five or more times per week compared with those who rarely or never ate nuts [4]. Other studies showed that daily intake of 30-90 g of almonds improved the glycemic status [21, 22]. However, the number of studies investigating the effects of specific nuts like pistachios is low. Therefore, we designed this crossover trial to investigate the effect of regularly consuming pistachio nuts on blood glucose and insulin resistance in patients with type 2 diabetes.
In this study, FBG and HbA1c decreased significantly in patients who consumed pistachio nuts, resulting in improved glycemic status. The improvements in FBG and HbA1c were observed after intervention at the end of the treatment phases. Also, prolonged antiglycemic effects have been observed far beyond the treatment period. Our results are in agreement with other studies which also observed reductions in FBG after pistachio consumption. Wang et al. showed that the consumption of 70 g pistachios for 12 weeks improved FBG. This study compared three groups (42 g pistachios daily, 70 g pistachios, and no pistachios). Glucose values 2 h after a 75 g glucose challenge were significantly lower at week 12 compared with baseline in the first and second group, while no significant changes were seen in the third group (no pistachios) [11]. The study by Josse et al. showed that the consumption of pistachio nuts, when consumed in combination with high carbohydrate foods, decreased the absorption of carbohydrate, and lowered postprandial blood glucose [21].
The effects on systolic blood pressure and CRP concentrations showed an analogy to the prolonged antiglycemic effect throughout the study phases. This finding points to sustainable anti-hypertensive, and anti-inflammatory effects. The effect on insulin resistance was inconclusive, with similar reductions in control subjects. This was in stark contrast to the observed antiglycemic effect, but may be explained by the use of HOMA-IR, which is an unfeasible measure for insulin resistance in type 2 diabetes patients as it is sometimes falsely low in type 2 diabetes patients (see limitations below).
Generally, pistachio nuts have antioxidant properties that may contribute to the antiglycemic effects observed in this study. These properties may be due to their richness in natural phenolic compounds [6], aldohexose inhibition [11], and the presence of magnesium (120 mg in 100 g pistachios each) [23, 24]. CRP is considered an inflammatory marker, and its involvement in insulin resistance has been proven [25, 26]. Our study provides evidence on the relationship between the specific consumption of pistachio nuts and beneficial CRP effects, which has not been found before.
In agreement with our study, Li et al. found that daily consumption of pistachios significantly reduced BMI in postmenopausal women with prediabetes or early untreated diabetes. During a 12-week consumption period, the BMI decreased from 30.1 ± 0.4 to 28.8 ± 0.4 [25]. The antiobese effect of pistachio consumption may be attributed to several properties of pistachio nuts, including starch blockage, inhibition of appetite and fat absorption, low energy density, and inhibition of enzymatic activity of amylase and α-glucosidase [27-29]. Therefore, based on these properties, pistachios can be considered as a beneficial supplement in the treatment of diabetes, and they can be taken without the fear of weight gain, which is sometimes said to be the case after consumption of nuts [29].
5. Limitations
This study has some limitations. Firstly, the wash-out period was only 8 weeks. Since HbA1c is a reflection of glycemic control over 12 weeks, it is likely that there was an effect on the second phase of treatment from diet consumption during the first phase. Secondly, glucagon hormone was not measured, and OGTT was not performed. The inclusion of these measures could have provided a more comprehensive picture of the antidiabetic properties of pistachio nuts. Another limitation was due to the use of HOMA-IR in type 2 diabetes. HOMA-IR is falsely low in patients with diabetes because these patients cannot secret sufficient insulin in response to insulin resistance.
6. Conclusion
In conclusion, based on the antidiabetic, antiobese, and anti-inflammatory properties of pistachio nuts, their consumption should be considered as a supplement in the diet of type 2 diabetic persons.
Disclosures: The authors report no conflict of interests.
References
- 1.Kabir M, Skurnik G, Naour N, Pechtner V, Meugnier E, Rome S, Quignard-Boulange A, Vidal H, Slama G, Clement K, Guerre-Millo M, Rizkalla SW. Treatment for 2 mo with n 3 polyunsaturated fatty acids reduces adiposity and some atherogenic factors but does not improve insulin sensitivity in women with type 2 diabetes: a randomized controlled study. Am J Clin Nutr. 2007;86(6):1670–1679. doi: 10.1093/ajcn/86.5.1670. [DOI] [PubMed] [Google Scholar]
- 2.Zhao G, Etherton TD, Martin KR, Vanden Heuvel JP, Gillies PJ, West SG, Kris-Etherton PM. Anti-inflammatory effects of polyunsaturated fatty acids in THP-1 cells. Biochem Biophys Res Commun. 2005;336(3):909–917. doi: 10.1016/j.bbrc.2005.08.204. [DOI] [PubMed] [Google Scholar]
- 3.Brehm BJ, Lattin BL, Summer SS, Boback JA, Gilchrist GM, Jandacek RJ, D'Alessio DA. One-year comparison of a high-monounsaturated fat diet with a high-carbohydrate diet in type 2 diabetes. Diabetes Care. 2009;32(2):215–220. doi: 10.2337/dc08-0687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jiang R, Manson JE, Stampfer MJ, Liu S, Willett WC, Hu FB. Nut and peanut butter consumption and risk of type 2 diabetes in women. JAMA. 2002;288(20):2554–2560. doi: 10.1001/jama.288.20.2554. [DOI] [PubMed] [Google Scholar]
- 5.Gentile C, Tesoriere L, Butera D, Fazzari M, Monastero M, Allegra M, Livrea MA. Antioxidant activity of Sicilian pistachio (Pistaciavera L. var. Bronte) nut extract and its bioactive components. J Agric Food Chem. 2007;55(3):643–648. doi: 10.1021/jf062533i. [DOI] [PubMed] [Google Scholar]
- 6.Tomaino A, Martorana M, Arcoraci T, Monteleone D, Giovinazzo C, Saija A. Antioxidant activity and phenolic profile of pistachio (Pistaciavera L., variety Bronte) seeds and skins. Biochimie. 2010;92(9):1115–1122. doi: 10.1016/j.biochi.2010.03.027. [DOI] [PubMed] [Google Scholar]
- 7.Due A, Larsen TM, Mu H, Hermansen K, Stender S, Astrup A. Comparison of 3 ad libitum diets for weight-loss maintenance, risk of cardiovascular dis¬ease, and diabetes: a 6-month randomized, controlled trial. Am J Clin Nutr. 2008;88(5):1232–1241. doi: 10.3945/ajcn.2007.25695. [DOI] [PubMed] [Google Scholar]
- 8.Adeghate E, Schattner P, Dunn E. An update on the etiology and epidemiology of diabetes mellitus. Ann NY Acad Sci. 2006;1084:1–29. doi: 10.1196/annals.1372.029. [DOI] [PubMed] [Google Scholar]
- 9.Kris-Etherton PM, Hu FB, Ros E, Sabate J. The role of tree nuts and peanuts in the prevention of coronary heart disease: multiple potential mechanisms. J Nutr. 2008;138(9):S1746–S1751. doi: 10.1093/jn/138.9.1746S. [DOI] [PubMed] [Google Scholar]
- 10.West SG, Gebauer SK, Kay CD, Bagshaw DM, Savastano DM, Diefenbach C, Kris-Etherton PM. Diets containing pistachios reduce systolic blood pressure and peripheral vascular responses to stress in adults with dyslipidemia. Hypertension. 2012;60(1):58–63. doi: 10.1161/HYPERTENSIONAHA.111.182147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wang X, Li Z, Liu Y, Lv X, Yang W. Effects of pistachios on body weight in Chinese subjects with metabolic syndrome. Nutr J. 2012;11:20. doi: 10.1186/1475-2891-11-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hernandez-Alonso P, Salas-Salvado J, Baldrich-Mora M, Juanola-Falgarona M, Bullo M. Beneficial effect of pistachio consumption on glucose metabolism, insulin resistance, inflammation, and related metabolic risk markers: a randomized clinical trial. Diabetes Care. 2014 doi: 10.2337/dc14-1431. In press. [DOI] [PubMed] [Google Scholar]
- 13.Kendall CW, West SG, Augustin LS, Esfahani A, Vidgen E, Bashyam B, Sauder KA, Campbell J, Chiavaroli L, Jenkins AL, Jenkins DJ. Acute effects of pistachio consumption on glucose and insulin, satiety hormones and endothelial function in the metabolic syndrome. Eur J Clin Nutr. 2014;68(3):370–375. doi: 10.1038/ejcn.2013.275. [DOI] [PubMed] [Google Scholar]
- 14.Sari I, Baltaci Y, Bagci C, Davutoglu V, Erel O, Celik H, Ozer O, Aksoy N, Aksoy M. Effect of pistachio diet on lipid parameters, endothelial function, inflammation, and oxidative status: A prospective study. Nutrition. 2010;26(4):399–404. doi: 10.1016/j.nut.2009.05.023. [DOI] [PubMed] [Google Scholar]
- 15.O'Brien E, Asmar R, Beilin L. Practice guidelines of the European Society of hypertension for clinic, ambulatory and self-blood pressure measurement. J Hypertens. 2005;23(4):697–702. doi: 10.1097/01.hjh.0000163132.84890.c4. [DOI] [PubMed] [Google Scholar]
- 16.Gosse P. Blood pressure should be measured in both arms on the first consultation. J Hypertens. 2002;20(6):1045–1055. doi: 10.1097/00004872-200206000-00004. [DOI] [PubMed] [Google Scholar]
- 17.Eknoyan G. Adolphe Quetelet (1796-1874) - the average man and indices of obesity. Nephrol Dial Transplant. 2008;23(1):47–51. doi: 10.1093/ndt/gfm517. [DOI] [PubMed] [Google Scholar]
- 18.Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–419. doi: 10.1007/BF00280883. [DOI] [PubMed] [Google Scholar]
- 19.Kameswararao B, Kesavulu MM, Apparao C. Evaluation of antidiabetic effect of Momordicacymbalaria fruit in alloxan-diabetic rats. Fitoterapia. 2013;74(1-2):7–13. doi: 10.1016/s0367-326x(02)00297-6. [DOI] [PubMed] [Google Scholar]
- 20.Lovejoy JC, Most MM, Lefevre M, Greenway FL, Rood JC. Effect of diets enriched in almonds on insulin action and serum lipids in adults with normal glucose tolerance or type 2 diabetes. Am J Clin Nutr. 2002;76(5):1000–1006. doi: 10.1093/ajcn/76.5.1000. [DOI] [PubMed] [Google Scholar]
- 21.Josse AR, Kendall CW, Augustin LS, Ellis PR, Jenkins DJ. Almonds and postprandial glycemia-a dose-response study. Metabolism. 2007;56(3):400–404. doi: 10.1016/j.metabol.2006.10.024. [DOI] [PubMed] [Google Scholar]
- 22.Rudkowska L. Functional foods for health: Focus on diabetes. Maturitas. 2009;62(3):263–269. doi: 10.1016/j.maturitas.2009.01.011. [DOI] [PubMed] [Google Scholar]
- 23.Hata A, Doi Y, Ninomiya T, Mukai N, Hirakawa Y, Hata J, Ozawa M, Uchida K, Shirota T, Kitazono T. et al. Magnesium intake decreases type 2 diabetes risk through the improvement of insulin resistance and inflammation: the Hisayama Study. Diabet Med. 2013;30(12):1487–1494. doi: 10.1111/dme.12250. [DOI] [PubMed] [Google Scholar]
- 24.Irandoost P, Ebrahimi-Mameghani M, Pirouzpanah S. Does grape seed oil improve inflammation and insulin resistance in overweight or obese women? Int J Food Sci Nutr. 2013;64(6):706–710. doi: 10.3109/09637486.2013.775228. [DOI] [PubMed] [Google Scholar]
- 25.Liu ZM, Ho SC. The association of serum C-reactive protein, uric acid and magnesium with insulin resistance in Chinese postmenopausal women with prediabetes or early untreated diabetes. Maturitas. 2011;70(2):176–181. doi: 10.1016/j.maturitas.2011.07.007. [DOI] [PubMed] [Google Scholar]
- 26.Asemi Z, Jazayeri S, Najafi M, Samimi M, Shidfar F, Tabassi Z, Shahaboddin M, Esmaillzadeh A. Association between markers of systemic inflammation, oxidative stress, lipid profiles, and insulin resistance in pregnant women. ARYA Atheroscler. 2013;9(3):172–178. [PMC free article] [PubMed] [Google Scholar]
- 27.Kotowaroo MI, Mahomoodally MF, Gurib-Fakim A, Subratty AH. Screening of traditional antidiabetic medicinal plants of Mauritius for possible alpha amylase inhibitory effects in vitro. Phytotherapy Research. 2006;20(3):228–231. doi: 10.1002/ptr.1839. [DOI] [PubMed] [Google Scholar]
- 28.Coates AM, Howe PR. Edible nuts and metabolic health. Curr Opin Lipidol. 2007;18(1):25–30. doi: 10.1097/MOL.0b013e3280123a47. [DOI] [PubMed] [Google Scholar]
- 29.Baer DJ, Gebauer SK, Novotny JA. Measured energy value of pistachios in the human diet. Br J Nutr. 2012;107(1):120–125. doi: 10.1017/S0007114511002649. [DOI] [PubMed] [Google Scholar]