

Abstract
Orthotopic neobladder reconstruction is becoming an increasingly common urinary diversion following cystectomy for bladder cancer. This is in recognition of the potential benefits of neobladder surgery over creation of an ileal conduit related to quality of life (QoL), such as avoiding the need to form a stoma with its cosmetic, psychological and other potential complications. The PubMed database was searched using relevant search terms for articles published electronically between January 1994 and April 2014. Full-text articles in English or with English translation were assessed for relevance to the topic before being included in the review. Patients with neobladders have comparable or better post-operative sexual function than those with ileal conduits. They also have comparable QoL to those with ileal conduits. Orthotopic neobladder is a good alternative to ileal conduit in suitable patients who do not want a stoma and are motivated to comply with neobladder training. However, the selection of a neobladder as the urinary diversion of choice requires that patients have good renal and liver functions and are likely to be compliant with neobladder training. With benefits also come potential risks of neobladder formation. These include electrolyte abnormalities and nocturnal incontinence. This short review highlights current aspects of neobladder formation and its potential advantages.
Keywords: Erectile dysfunction, quality of life, urinary bladder, urinary diversion, urinary incontinence
INTRODUCTION
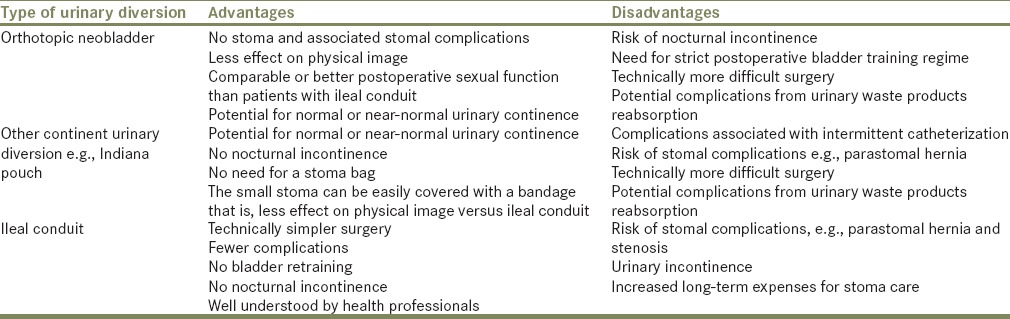
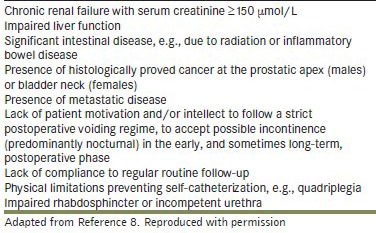
Bladder cancer (BC) is the ninth most common cancer worldwide. After prostate cancer, it is the second most common urologic malignancy worldwide. In both sexes, the age-standardized rate of BC in 2012 is 5.3/100,000 whereas the mortality rate stands at 1.9/100,000. The 5-year prevalence is 25.4/100,000.[1] BC is definitively diagnosed through histological examination of tissue samples that determines the degree of cell differentiation (tumor grade) and spread (tumor stage). BC is staged using the tumor, node and metastasis system which considers the extent of local tumor spread (T), presence of cancer in lymph nodes (N) or metastasis (M). The “gold standard” treatment for high-grade BC is radical cystectomy with extended lymphadenectomy and urinary diversion, which includes ileal conduit, continent urinary reservoir and orthotopic neobladder. The type of urinary diversion performed [Figure 1] depends on the patient's and surgeon's preference, associated comorbidity and target quality of life (QoL) postoperatively. An orthotopic neobladder avoids the need to form a stoma and risk of stomal complications with associated physical and psychosocial effects; up to 63%, 58% and 42% of patients with an ileal conduit felt less complete, were apprehensive about stomal leakage and embarrassed due to the stoma, respectively.[2] However, there are other issues to consider with this orthotopic diversion such as patient suitability from a co-morbidity perspective as well as for compliance to a neobladder training regime, continence, sexual function and their anticipated QoL [Table 1]. There are also some contraindications to orthotopic neobladder reconstruction such as renal and liver impairment, intestinal disease and cancer at the prostatic apex or bladder neck [Box 1]. The purpose of this review is to discuss the important considerations of orthotopic neobladder reconstruction, namely effects on electrolyte balance and nutrition, neobladder training and continence. The effect of this procedure on sexual function and QoL in comparison with ileal conduit urinary diversion are also discussed.
Figure 1.
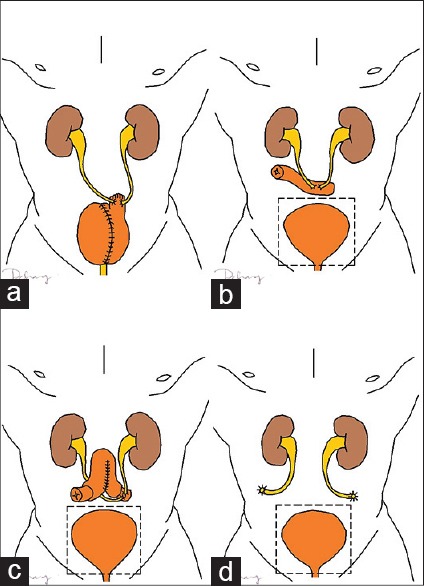
Types of urinary diversion surgery; (a) orthotopic neobladder (specifically Hautmann neobladder with chimney ureteroileal anastomosis), (b) ileal conduit, (c) continent ileostomy, and (d) cutaneous ureterostomy. Fenestrated box represents the removed native bladder. (Figure illustrated by Dwayne Chang. Copyright Nathan Lawrentschuk and Dwayne Chang. Reproduced with permission.)
Table 1.
Advantages and disadvantages of orthotopic neobladder and ileal conduit urinary diversions
Box 1.
Characteristics of patients who are not suitable to undergo orthotopic neobladder reconstruction
LITERATURE REVIEW
The PubMed database was searched using the following terms: “neobladder,” “orthotopic,” “urinary diversion,” “ileal conduit,” “BC,” “cystectomy,” “continence,” “QoL,” “urodynamics,” “complication” and “sexual function” in various AND/OR combinations for articles published electronically between January 1994 and April 2014. All original full-text articles in English were assessed for relevance to the topic so that this review can present a balanced view of current research findings. There was no exclusion of articles based on the level of evidence as a significant portion of relevant articles were case series. Publications in other languages were also included only if there was an English translation of the article and the content supplied useful information. Furthermore, the reference lists of included articles were searched to include further relevant papers even though they may be published prior to year 1994.
PROCEDURE/TYPES OF ORTHOTOPIC NEOBLADDER
Although there are various ways of folding intestinal segments to construct a neobladder, each method has the aim of creating a spherical reservoir, the significance of which will be discussed below. Described types include Camey I and II (U-shaped), modified Camey II (Z-shaped), Kock (sagitally-folded U-shaped), T-pouch (sagitally-folded U-shaped), Studer (sagitally-folded U-shaped), Hautmann (W-shaped) and the Abol-Enein and Ghoneim modification of the W pouch,[3] and vesica ileale Padovana (circular). Ileocolonic neobladders include the Mainz pouch and Le Bag pouch, and an example of a sigmoid neobladder is the Reddy pouch.
Formation of a neobladder requires reconstruction of intestinal segments. There are thus two important considerations: (1) The type of the intestinal segment and (2) the construction type. Ileum, colon and sigmoid are commonly used intestinal segments used for neobladder reconstruction. Terminal ileum is more favored among the three as it is more distensible and has larger capacity;[4] it therefore stores urine at lower pressures thus there is less risk of causing high-pressure damage to the kidneys. The terminal ileum also experiences more mucosal atrophy in the long term which means reduced risk of metabolic consequences as there will be less electrolyte exchange across the mucosa.[4]
The second consideration is the type of construction. Intestinal segments are naturally cylindrical in shape but according to Laplace law [Box 2], this is not the best shape to maintain a low pressure in the reservoir. Due to the smaller radius in a cylindrical reservoir, there will be higher intraluminal pressures at lower volumes. Detubularized bowel may be refashioned to a spherical reservoir; however, the larger radius enables it to contain higher volumes at lower intraluminal pressures.[5] The sphere has the smallest surface area for the same volume meaning: (1) This has the smallest risk of metabolic consequences secondary to electrolyte exchange across the gut mucosal lining in the neobladder and (2) a minimal length of intestinal segment is required to form a sphere.
Box 2.
Laplace law for a spherical reservoir

ELECTROLYTE DISORDERS
The wall of a neobladder is lined with intestinal mucosa which is more permeable to urinary electrolytes than urothelium. Hence, metabolic issues may arise due to extended contact time of urine to the intestinal mucosa compared with incontinent urinary diversion. Urine contains elevated concentrations of potassium, hydrogen and chloride. These ions are absorbed in exchange with sodium and bicarbonate from the blood stream, thus resulting in hyperchloremic, hyperkalemic metabolic acidosis and salt-loss syndrome.[6,7] These conditions can manifest clinically with lethargy, fatigue and dehydration. It is important to detect and treat metabolic acidosis early as it can induce calcium resorption from bone and hypophosphatemia thus leading to osteoporosis and osteomalacia. In addition, metabolic acidosis can cause hypercalciuria that increases the risk of developing renal stones.[7,8] Furthermore, urine is more concentrated than intracellular conditions. This promotes fluid shifts from the neobladder walls into the urine and can lead to dehydration.
Other urinary wastes such as creatinine, urea and ammonia excreted in the urine are reabsorbed by the gut mucosa as well. Therefore, impaired renal function is a contraindication to having a neobladder as there will be extra burden on impaired kidneys to excrete reabsorbed these urinary waste products. The same applies to liver function as well because increased burden on an impaired liver to metabolize reabsorbed urinary wastes such as ammonia can increase the risk of liver failure.[9]
NUTRITION
Patients undergoing neobladder formation have a higher risk of experiencing ileus ≥5 days postoperative than those undergoing ileal conduit formation (14.8% vs. 5.5%, P = 0.018).[10] Therefore, it is imperative that they have sufficient glycogen stores in their liver by means of pre-operative carbohydrate and protein supplementation, e.g., high-carbohydrate drinks as close as possible to surgery. Adequate dietary fiber postoperatively to reduce constipation and monitoring of vitamin B12 and folic acid are important due to potential impact on the terminal ileum – the only part of the intestine that can absorb these nutrients – are significantly shorter postoperatively. Terminal ileal reduction also interferes with bile acid reabsorption, resulting in malabsorption of fat which can precipitate diarrhea and dehydration. Such issues are more prominent if the surgery involves resection of the ileocecal valve, as colonic organisms (e.g. bacteroides) can enter the ileum and cleave bile acids from their conjugates; the resultant free bile acids are poor fat emulsifiers.[7,11] Patients with a neobladder also need to ensure adequate hydration as they could potentially lose a significant amount of water into the urine.
CONTINENCE
Neobladders are a form of continent urinary diversion but are not free of continence issues. Continence rates vary with surgical technique, length of time after the operation and time of day. Total continence rates with neobladders range from 22.3% to 63.2% at 12 months postoperatively,[12,13] and 17.7–74.5% beyond 40 months postoperatively.[14,15] Daytime continence rates vary from 21.4% to 99.0% at 3–48 months postoperatively.[13,14,15,16,17,18] The Abol-Enein and Ghoneim modification of the W pouch, a commonly used technique, recorded a daytime continence rate of 93.3%.[3] Interestingly, Sevin et al. demonstrated a gradually increasing daytime continence rate with time; at 6, 12, 24, 36 and ≥ 48 months postoperatively, daytime continence rates were 63%, 70%, 76%, 88% and 92%, respectively.[19] Furthermore, there were no significant difference in daytime incontinence rates between patients with a modified S-pouch neobladder and a healthy control population without urinary diversion (10% vs. 9.3%, P = 0.1).[20]
Patients with a neobladder are generally less continent at night than in the daytime. In the nighttime, 18.9–79%, 74%, 23%, 77.6% and 44% of patients were continent at 12, 38 (mean), 44 (median), 48 and 54 (mean) months postoperatively, respectively.[13,14,15,17,18,19,21] The Abol-Enein and Ghoneim modification of the W pouch has a high nighttime continence rate of 80% at a mean follow-up of 38 months.[3] Again, Sevin et al. demonstrated a gradually increasing nocturnal continence rate with time; at 6, 12, 24, 36 and ≥48 months postoperatively, nocturnal continence rates were 55%, 62%, 73%, 85% and 90%, respectively.[19] In comparison with healthy subjects of similar age, gender and comorbidities, patients with a modified S-pouch neobladder had a significantly higher rate of nocturnal incontinence (28% vs. 3.7%, P = 0.003).[20] Nocturnal incontinence is a significant issue as 48% of patients with nocturnal incontinence at least once a week suffered moderate-severe negatively affected sleep compared with 16% of patients with nocturnal incontinence of up to once a month (relative risk 3.0, 95% CI: 2.0–4.7). Furthermore, self-assessed QoL was lower in those patients who had moderate-severe negatively affected sleep than those with minimal adversely affected sleep.[21]
Lack of standardization in the definition of continence, different surgical techniques in neobladder reconstruction and variation in patients’ record-keeping may account for such a wide range in continence rates between studies. The definition and measurement of continence should be based on an approved scoring system such as the International Consultation on Incontinence Questionnaire–Urinary Incontinence Short Form (ICIQ-UI SF) scoring system. Practicably, patients should keep a diary to record the frequency and severity of daytime and nocturnal incontinence to improve the accuracy of future studies, and this is part of neobladder training in any case.
NEOBLADDER TRAINING
Laplace law [Box 2] dictates that increasing the radius of a reservoir will increase the wall tension thus inducing more tissue damage. When pressure within a spherical reservoir increases, the wall tension will increase by the same factor if the wall thickness and radius of the reservoir is maintained. In a real neobladder, however, any further distention beyond the full capacity will increase the size and thus the radius of the reservoir, along with stretching the neobladder wall, which reduces the wall thickness. Over-distension should be avoided, especially in the immediate and early postoperative period to avoid damage to the healing tissues by intensive neobladder training – an important consideration with patient selection.
In the immediate postoperative stage, an indwelling and suprapubic catheter remains in the neobladder postoperatively to allow for adequate surgical recovery before commencing neobladder training. Regular 6–8 hourly flushing of the indwelling catheter with 100 mL of normal saline 0.9% is performed to reduce the risk of catheter blockage. At our institutions, a cystogram is performed at 2–3 weeks postoperatively to confirm that the new reservoir is watertight. Removal of the indwelling catheter and trial of void is then performed under supervision to allow for close monitoring of voided and post-void volumes, blood pH and bicarbonate levels, teaching of neobladder emptying techniques and if necessary, teaching of intermittent self-catheterization techniques. Techniques to void urine from a neobladder are important as it lacks the contractility of a native bladder. We instruct our patients to void in the sitting position, consciously relax the sphincter and pelvic floor muscles and then use a Valsalva maneuver to empty their neobladder. If required, patients may also increase their intra-abdominal pressure by leaning forward or exert gentle manual pressure over the lower abdomen and suprapubic area.[6] Pelvic floor muscular awareness and education are also critical in recovery and is well-summarized elsewhere.[6,9] As with radical prostatectomy stress incontinence may ensue early, but gradually recovers with correct pelvic floor muscle contraction assisting with strength and control.
The second important consideration is gradual increment of neobladder capacity with a transition from a capacity of 150–200 mL to 400–500 mL in the longer term. During the early stages, frequent neobladder emptying is performed 2–3 hourly daily and 3-hourly timed nightly to avoid overflow incontinence.[6,22] Voiding intervals can then be increased gradually over the next few weeks to achieve the aim of voiding every 5–6 h during the day and just once at night. It is also important to note that high post-void residual urine volumes will require the need to void more frequently as the neobladder fills up more rapidly. Patients faced with the issue of inadequate emptying even after performing the correct maneuvers may have to consider intermittent self-catheterization. Patients with higher body mass index are at risk (OR 1.5; 95% CI: 1.06–2.15, P = 0.023).[15]
URODYNAMICS
The etiology of incontinence in neobladders has also been investigated by means of urodynamic studies. Multivariate analysis revealed that large post-void residual urine volume, and frequency and maximum amplitude of uninhibited contractions were the most significant parameters associated with nocturnal incontinence.[23] Pharmacotherapy has a role in improving continence. A small trial has yielded promising results with oxybutynin (5 mg 3 times/day) and verapamil (240 mg once daily) with 70% and 55% clinical improvement, respectively.[24]
Besides incontinence, some patients experience poor neobladder emptying or “hypercontinence” as well. Certain complications of neobladders such as electrolyte disorders, acidosis, urinary tract infections and pouch calculi formation are more pronounced in such patients. Final bladder shape and length of the bowel segment may affect post-void residual urine volumes. It is important to recognize and teach intermittent catheterization as required.
SEXUAL FUNCTION
Effects on erectile function and sexual desire are important considerations in cystectomy. Therefore, techniques to preserve the neurovascular bundle supplying the genitalia have been developed to help maintain preoperative sexual function. Bilateral preservation of the neurovascular bundle in ileal neobladder formation has been shown to achieve a 2-year potency rate of up to 60% compared with a rate of 30% achieved with unilateral preservation techniques.[25] There are conflicting findings. Protogerou et al. found no statistically significant indication of sexual dysfunction in women with nerve-sparing modified S-pouch neobladder and those without.[20] Even with nerve-sparing procedures, men with a modified S-pouch neobladder still experienced significantly lower rates of erections (35.5 vs. 83.3%, P = 0.003) and decreased erection quality (22.2 vs. 83.3%, P = 0.002) than normal subjects.[20] A recent case series also supported these findings; Asgari et al. found that men experienced significant deterioration in both erectile function and sexual desire postoperatively, irrespective of the type of urinary diversion performed.[26]
Between 23.7–35.5% of patients retain adequate erectile function after neobladder reconstruction.[15,20,26] Some studies demonstrated that neobladder reconstruction results in better preservation of sexual function when compared with an ileal conduit using the International Index of Erectile Function questionnaire. Specifically, 35.0% of men in the ileal neobladder group were able to achieve and maintain erections sufficient for vaginal penetration throughout sexual intercourse, compared with 9.8% of men in the ileal conduit group (P = 0.006). In addition, more men in the ileal neobladder group rated their sexual desire high or very high in comparison with men in the ileal conduit group (45.0% vs. 24.4%, P = 0.01).[26] Asgari et al. also found that more men with an ileal neobladder reported unaltered sexual desire compared with patients who had an ileal conduit (17.5% vs. 7.2%, P = 0.01).[27] There are conflicting results from other studies where no difference was found.[27,28]
QUALITY OF LIFE
Quality of life is a very broad term; it is typically subdivided into a number of parameters to help ascertain the effect on an aspect of someone's life. Comparing QoL is affected by the lack of standardization in the use of various questionnaires types among comparison studies and the suitability or relevance of each. Some instruments measure QoL in general whereas some are more specific toward the unique ways urinary diversion can impact on life. The QoL in patients who had neobladder reconstruction are commonly compared to the life experienced by those with an ileal conduit, likely because these are the two most common urinary diversion procedures performed in most locations.
Fujisawa et al. compared the health-related QoL using the SF-36 questionnaire in 56 patients and found no statistically significant difference in scoring parameters between patients who had neobladder and those with an ileal conduit. However, patients with either a neobladder or ileal conduit scored significantly lower than the general United States population norm in terms of role-physical functioning and role-emotional functioning.[29] In a similar study on 88 Italian men using the SF-36 questionnaire, there was again no statistically significant difference in scoring parameters between patients who had neobladder and those with an ileal conduit. However, patients with either a neobladder or ileal conduit scored significantly lower than the general Italian population norm in terms of role-physical functioning, social functioning and role-emotional functioning.[30] Studies using different QoL questionnaires (QLQ) also found similar results. Sogni et al. did not find any statistically significant difference in any questionnaire parameters among patients who had a neobladder and those with an ileal conduit when assessed using the European Organization for Research and Treatment of Cancer instruments QoL questionnaire-C30 (QLQ-C30) and QLQ-muscle-invasive BC module (QLQ-BLM).[31] In addition to no statistically significant difference in the QoL of patients with a neobladder or ileal conduit, Protogerou et al. also found no significant difference when compared to the QoL of a control population (patients without BC) using the QLQ-C30 questionnaire.[20]
There are, however, conflicting findings in other studies. In a prospective study by Singh et al. using the QLQ-C30 questionnaire, patients who underwent orthotopic neobladder reconstruction reported significantly better physical functioning (P ≤ 0.001), role functioning (P ≤ 0.01), social functioning (P = 0.01) and global health status/QoL (P ≤ 0.002) throughout the first 18 months postoperatively compared with patients who had ileal conduit formation.[32] Although the patients who had orthotopic neobladder reconstruction were significantly younger by a mean age of 2-year, there was no significant differences in any of the baseline QoL variables and none of the preoperative QoL domains were correlated with age.[32] Using the QLQ-C30 questionnaire, Erber et al., also found significantly better global health status/QoL (P = 0.019) and better physical functioning (P = 0.018) in patients with an ileal neobladder compared with those with ileal conduit formation.[10] Physical and emotional well-being scores in women with a neobladder were also significantly better (P < 0.03) than those with a cutaneous ureterostomy when assessed using the Functional Assessment of Cancer Therapy for BC (BL) questionnaire.[33] Using a 98-item questionnaire, Asgari et al. found a significantly higher global satisfaction rate among those with an ileal neobladder compared with those with an ileal conduit (76.2% vs. 52.8%, P = 0.002).[27] Contradictory findings were present in a study by Thulin et al. who found that 37% of those with an orthotopic neobladder reported that it adversely affected their sleeping patterns, compared with 22% of those with a urostomy. Moderate or much bother due to the daytime and nighttime emptying frequency was statistically significantly higher in those with orthotopic neobladder versus non-continent urostomy, 29% versus 19%, respectively.[21] In this study, one possible reason for patients with neobladder not reporting a better QoL than those with ileal conduit is that the higher incidence of sleep disturbances negatively affect the energy level and QoL in the daytime.
CONCLUSION
Orthotopic neobladder reconstruction has a number of unique advantages and disadvantages as compared with other forms of urinary diversion. This procedure requires comprehensive counseling between the patient and the surgeon to discuss the various considerations of the procedure. The important issues include preventing metabolic complications, managing urinary incontinence especially during the early postoperative stage and ensuring patient compliance to a neobladder training regime. In addition, potential patients should be carefully selected, keeping in mind the contraindications for this surgery in order to reduce the risk of postoperative complications. Continence rates vary widely among studies depending on the time since the operation, type of neobladder reconstruction and definition of urinary incontinence in the studies. Urinary incontinence rates are higher at night than in the daytime, and this reduces sleep quality. In comparison with ileal conduit formation, patients who had orthotopic neobladder reconstruction surgery reported predominantly comparable or better QoL and sexual function.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012. International Agency for Research on Cancer. 2012. [Last cited on 2014 Jan 23]. Available from: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx .
- 2.Philip J, Manikandan R, Venugopal S, Desouza J, Javlé PM. Orthotopic neobladder versus ileal conduit urinary diversion after cystectomy – A quality-of-life based comparison. Ann R Coll Surg Engl. 2009;91:565–9. doi: 10.1308/003588409X432293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Abol-Enein H, Ghoneim MA. Functional results of orthotopic ileal neobladder with serous-lined extramural ureteral reimplantation: Experience with 450 patients. J Urol. 2001;165:1427–32. [PubMed] [Google Scholar]
- 4.Gakis G, Stenzl A. Ileal neobladder and its variants. Eur Urol Suppl. 2010;9:745–53. [Google Scholar]
- 5.Basford JR. The Law of Laplace and its relevance to contemporary medicine and rehabilitation. Arch Phys Med Rehabil. 2002;83:1165–70. doi: 10.1053/apmr.2002.33985. [DOI] [PubMed] [Google Scholar]
- 6.Herdiman O, Ong K, Johnson L, Lawrentschuk N. Orthotopic bladder substitution (Neobladder): Part II: Postoperative complications, management, and long-term follow-up. J Wound Ostomy Continence Nurs. 2013;40:171–80. doi: 10.1097/WON.0b013e31827e8499. [DOI] [PubMed] [Google Scholar]
- 7.Stein R, Schröder A, Thüroff JW. Bladder augmentation and urinary diversion in patients with neurogenic bladder: Nonsurgical considerations. J Pediatr Urol. 2012;8:145–52. doi: 10.1016/j.jpurol.2011.03.015. [DOI] [PubMed] [Google Scholar]
- 8.Wiederkehr M, Krapf R. Metabolic and endocrine effects of metabolic acidosis in humans. Swiss Med Wkly. 2001;131:127–32. doi: 10.4414/smw.2001.09666. [DOI] [PubMed] [Google Scholar]
- 9.Ong K, Herdiman O, Johnson L, Lawrentschuk N. Orthotopic bladder substitution (neobladder): Part I: Indications, patient selection, preoperative education, and counseling. J Wound Ostomy Continence Nurs. 2013;40:73–82. doi: 10.1097/WON.0b013e31827759ea. [DOI] [PubMed] [Google Scholar]
- 10.Erber B, Schrader M, Miller K, Schostak M, Baumunk D, Lingnau A, et al. Morbidity and QoL in BC patients following cystectomy and urinary diversion: A single-institution comparison of ileal conduit versus orthotopic neobladder. ISRN Urol 2012. 2012:342796. doi: 10.5402/2012/342796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Thorstenson A, Jacobsson H, Onelöv E, Holst JJ, Hellström PM, Kinn AC. Gastrointestinal function and metabolic control after construction of an orthotopic ileal neobladder in BC. Scand J Urol Nephrol. 2007;41:14–9. doi: 10.1080/00365590600911217. [DOI] [PubMed] [Google Scholar]
- 12.Aleksic P, Bancevic V, Milovic N, Kosevic B, Stamenkovic DM, Karanikolas M, et al. Short ileal segment for orthotopic neobladder: A feasibility study. Int J Urol. 2010;17:768–73. doi: 10.1111/j.1442-2042.2010.02599.x. [DOI] [PubMed] [Google Scholar]
- 13.Ahmadi H, Skinner EC, Simma-Chiang V, Miranda G, Cai J, Penson DF, et al. Urinary functional outcome following radical cystoprostatectomy and ileal neobladder reconstruction in male patients. J Urol. 2013;189:1782–8. doi: 10.1016/j.juro.2012.11.078. [DOI] [PubMed] [Google Scholar]
- 14.Meyer JP, Drake B, Boorer J, Gillatt D, Persad R, Fawcett D. A three-centre experience of orthotopic neobladder reconstruction after radical cystectomy: Initial results. BJU Int. 2004;94:1317–21. doi: 10.1111/j.1464-410X.2004.05164.x. [DOI] [PubMed] [Google Scholar]
- 15.Novara G, Ficarra V, Minja A, De Marco V, Artibani W. Functional results following vescica ileale Padovana (VIP) neobladder: Midterm follow-up analysis with validated questionnaires. Eur Urol. 2010;57:1045–51. doi: 10.1016/j.eururo.2010.01.007. [DOI] [PubMed] [Google Scholar]
- 16.Girgin C, Sezer A, Ozer K, Tarhan H, Bolukbasi A, Gurel G. Comparison of three types of continent urinary diversions in a single center. Scientific World Journal. 2004;4(Suppl 1):135–41. doi: 10.1100/tsw.2004.59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Studer UE, Burkhard FC, Schumacher M, Kessler TM, Thoeny H, Fleischmann A, et al. 20-years experience with an ileal orthotopic low pressure bladder substitute – Lessons to be learned. J Urol. 2006;176:161–6. doi: 10.1016/S0022-5347(06)00573-8. [DOI] [PubMed] [Google Scholar]
- 18.Deliveliotis C, Alargoff E, Skolarikos A, Varkarakis I, Argyropoulos V, Dimopoulos C. Modified ileal neobladder for continent urinary diversion: Experience and results. Urology. 2001;58:712–6. doi: 10.1016/s0090-4295(01)01362-0. [DOI] [PubMed] [Google Scholar]
- 19.Sevin G, Soyupek S, Armagan A, Hoscan MB, Oksay T. Ileal orthotopic Neobladder (modified Hautmann) via a shorter detubularized ileal segment: experience and results. BJU Int. 2004;94:355–9. doi: 10.1111/j.1464-410X.2004.04933.x. [DOI] [PubMed] [Google Scholar]
- 20.Protogerou V, Moschou M, Antoniou N, Varkarakis J, Bamias A, Deliveliotis C. Modified S-pouch neobladder vs ileal conduit and a matched control population: A quality-of-life survey. BJU Int. 2004;94:350–4. doi: 10.1111/j.1464-410X.2004.04932.x. [DOI] [PubMed] [Google Scholar]
- 21.Thulin H, Kreicbergs U, Wijkström H, Steineck G, Henningsohn L. Sleep disturbances decrease self-assessed QoL in individuals who have undergone cystectomy. J Urol. 2010;184:198–202. doi: 10.1016/j.juro.2010.03.009. [DOI] [PubMed] [Google Scholar]
- 22.Steers WD. Voiding dysfunction in the orthotopic neobladder. World J Urol. 2000;18:330–7. doi: 10.1007/s003450000146. [DOI] [PubMed] [Google Scholar]
- 23.El Bahnasawy MS, Osman Y, Gomha MA, Shaaban AA, Ashamallah A, Ghoneim MA. Nocturnal enuresis in men with an orthotopic ileal reservoir: Urodynamic evaluation. J Urol. 2000;164:10–3. doi: 10.1097/00005392-200007000-00003. [DOI] [PubMed] [Google Scholar]
- 24.El-Bahnasawy MS, Shaaban H, Gomha MA, Nabeeh A. Clinical and urodynamic efficacy of oxybutynin and verapamil in the treatment of nocturnal enuresis after formation of orthotopic ileal neobladders. A prospective, randomized, crossover study. Scand J Urol Nephrol. 2008;42:344–51. doi: 10.1080/00365590701832726. [DOI] [PubMed] [Google Scholar]
- 25.Kessler TM, Burkhard FC, Perimenis P, Danuser H, Thalmann GN, Hochreiter WW, et al. Attempted nerve sparing surgery and age have a significant effect on urinary continence and erectile function after radical cystoprostatectomy and ileal orthotopic bladder substitution. J Urol. 2004;172:1323–7. doi: 10.1097/01.ju.0000138249.31644.ec. [DOI] [PubMed] [Google Scholar]
- 26.Asgari MA, Safarinejad MR, Shakhssalim N, Soleimani M, Shahabi A, Amini E. Sexual function after nonnerve-sparing radical cystoprostatectomy: A comparison between ileal conduit urinary diversion and orthotopic ileal neobladder substitution. Int Braz J Urol. 2013;39:474–83. doi: 10.1590/S1677-5538.IBJU.2013.04.04. [DOI] [PubMed] [Google Scholar]
- 27.Asgari MA, Safarinejad MR, Shakhssalim N, Soleimani M, Shahabi A, Amini E. QoL after radical cystectomy for BC in men with an ileal conduit or continent urinary diversion: A comparative study. Urol Ann. 2013;5:190–6. doi: 10.4103/0974-7796.115747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Frich PS, Kvestad CA, Angelsen A. Outcome and QoL in patients operated on with radical cystectomy and three different urinary diversion techniques. Scand J Urol Nephrol. 2009;43:37–41. doi: 10.1080/00365590802473198. [DOI] [PubMed] [Google Scholar]
- 29.Fujisawa M, Isotani S, Gotoh A, Okada H, Arakawa S, Kamidono S. Health-related QoL with orthotopic neobladder versus ileal conduit according to the SF-36 survey. Urology. 2000;55:862–5. doi: 10.1016/s0090-4295(00)00483-0. [DOI] [PubMed] [Google Scholar]
- 30.Autorino R, Quarto G, Di Lorenzo G, De Sio M, Perdonà S, Giannarini G, et al. Health related QoL after radical cystectomy: Comparison of ileal conduit to continent orthotopic neobladder. Eur J Surg Oncol. 2009;35:858–64. doi: 10.1016/j.ejso.2008.08.002. [DOI] [PubMed] [Google Scholar]
- 31.Sogni F, Brausi M, Frea B, Martinengo C, Faggiano F, Tizzani A, et al. Morbidity and QoL in elderly patients receiving ileal conduit or orthotopic neobladder after radical cystectomy for invasive BC. Urology. 2008;71:919–23. doi: 10.1016/j.urology.2007.11.125. [DOI] [PubMed] [Google Scholar]
- 32.Singh V, Yadav R, Sinha RJ, Gupta DK. Prospective comparison of quality-of-life outcomes between ileal conduit urinary diversion and orthotopic neobladder reconstruction after radical cystectomy: A statistical model. BJU Int. 2014;113:726–32. doi: 10.1111/bju.12440. [DOI] [PubMed] [Google Scholar]
- 33.Gacci M, Saleh O, Cai T, Gore JL, D’Elia C, Minervini A, et al. QoL in women undergoing urinary diversion for BC: Results of a multicenter study among long-term disease-free survivors. Health Qual Life Outcomes. 2013;11:43. doi: 10.1186/1477-7525-11-43. [DOI] [PMC free article] [PubMed] [Google Scholar]