

Sir,
Since intravenous urography is not performed as often as it used to, medullary sponge kidney can be missed easily. Hereby, we present a 66-year-old female with kidney stones. The analysis of the passed stones was 90% calcium oxalate monohydrate and 10% calcium phosphate. Abdomen CT without contrast showed numerous small bilateral nonobstructive renal calculi at papillary tips suggestive of medullary sponge kidneys. Dual energy CT characterization blue color coding indicated that the stone material was nonuric acid in composition. It is very crucial to recognize the characteristic of medullary sponge kidney in CT scan.
A 66-year-old female presented for evaluation for kidney stones. She did not pass her first kidney stone until the age of 62, at which time she passed 13 stones at once. She denied family history of kidney stones. Her medical history was significant for irritable bowel syndrome, but she denied diarrhea. The analysis of the passed stones was 90% calcium oxalate monohydrate and 10% calcium phosphate. Her blood tests revealed normal creatinine of 0.8 mg/dL. Her urine pH was 6.6. A 24-h urine was supersaturated with hydroxyapatite, otherwise unremarkable. Abdomen CT without contrast demonstrated numerous small bilateral nonobstructive renal calculi at papillary tips suggestive of medullary sponge kidneys [Figure 1]. Dual energy CT characterization blue color coding indicated that the stone material was nonuric acid in composition [Figure 2]. Her kidney stones were not amenable to surgical removal. The patient was informed about her diagnosis and encouraged to keep herself adequately hydrated.
Figure 1.
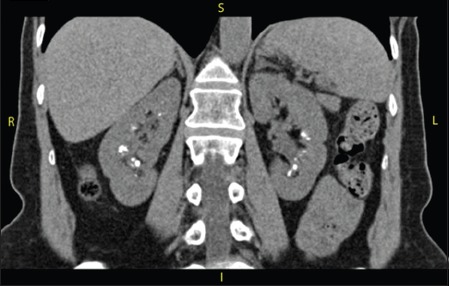
Abdomen CT without contrast demonstrated numerous small bilateral nonobstructive renal calculi at papillary tips suggestive of medullary sponge kidneys
Figure 2.
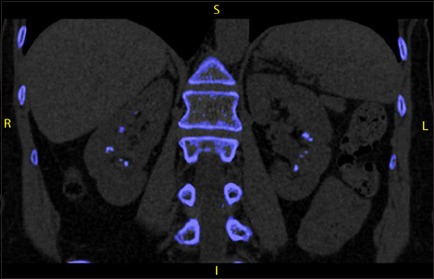
Dual energy CT characterization blue color coding indicated that the stone material was nonuric acid in composition
Patients with medullary sponge kidney usually form apatite (calcium phosphate) in their stones due to their increased urinary pH from incomplete distal renal tubular acidosis (RTA).[1,2] Calcium oxalate stones can also be developed[3] as in our case presentation. Since intravenous urography is not performed as often as it used to, medullary sponge kidney can be missed easily. For this reason, it is very crucial to recognize the characteristic of medullary sponge kidney in CT scan.
REFERENCES
- 1.Goldman SH, Walker SR, Merigan TC, Jr, Gardner KD, Jr, Bull JM. Hereditary occurrence of cystic disease of the renal medulla. N Engl J Med. 1966;274:984–92. doi: 10.1056/NEJM196605052741802. [DOI] [PubMed] [Google Scholar]
- 2.Morris RC, Yamauchi H, Palubinskas AJ, Howenstine J. Medullary sponge kidney. Am J Med. 1965;38:883–92. doi: 10.1016/0002-9343(65)90007-0. [DOI] [PubMed] [Google Scholar]
- 3.Baggio B, Priante G, Brunati AM, Clari G, Bordin L. Specific modulatory effect of arachidonic acid on human red blood cell oxalate transport: Clinical implications in calcium oxalate nephrolithiasis. J Am Soc Nephrol. 1999;10(Suppl 14):S381–4. [PubMed] [Google Scholar]