

Abstract
A case of complete bladder duplication with urethra duplication, diphallus, anorectal malformation and rightsided renal agensis with ipsilateral gonadal agenesisis was reported because of its rarity. Possible deranged embryology resulting in these anomalies has been reviewed with relevant hypothesis. The patient underwent several investigations and undergoing multistage surgical intervention.
Keywords: ARM, bladder duplication, diphallus
INTRODUCTION
Complete duplication of the urinary bladder is a rare anomaly. To the best of our knowledge only 50 cases have been reported in available literature.[1,2] Our case is the only one with associated right-sided renal agenesis with ipsilateral gonadal agenesis along with other multiple anomalies. The cause of duplication of the urinary bladder remains obscure although a few hypotheses have been proposed. All patients with bladder duplication must be carefully evaluated with respect to the high incidence of associated anomalies of other organ system. Due to paucity of cases in printed literature, there is no uniformity in the treatment plan. We report a case of complete bladder duplication with urethra duplication, diphallus,anorectal malformation, and right-sided renal agensis with ipsilateral gonadal agenesis. The patient is undergoing multistage surgical intervention.
CASE REPORT
A boy presented to us on 1st post-natal day with multiple congenital anomalies. On examination, there was no anal opening (ARM) and the boy had two phalluses, of which the larger one on the right had a meatal opening at the tip but was not passing urine. The smaller one on the left was passing urine, but was epispadiac and incontinent. Scrotum was bifid and the two hemiscrota and diphallus were separated widely by a soft mobile lump in the midline. The right hemiscrotum was empty and there was a palpable testis in the left hemiscrotum [Figures 1 and 2]. Beside these there were also the presence of scoliosis, spina bifida, and diastasis of symphysis pubis. He had undergone emergency sigmoid colostomy for the anorectal malformation.
Figure 1.

Photograph showing two phallus with bifid scrotum and intermittent soft tissue mass
Figure 2.

Photograph showing meatus at tip of right phallus and incontinent left phallus
Unfortunately, the boy lost to follow-up and come back after 3 years of age. For the evaluation of anomalies of the internal urogenital organs, various radiological investigations were performed.
Straight radiograph of the abdomen revealed scoliosis with convexity toward the left due to the presence of hemivertebra in the mid-lumbar spine. Spina bifida was noted at various lumbar vertebrae, along with diastasis of symphysis pubis. Distal colostogram demonstrated the column of rectal contrast ending at the level of ischial spines, suggesting an intermediate anorectal malformation [Figure 3].
Figure 3.
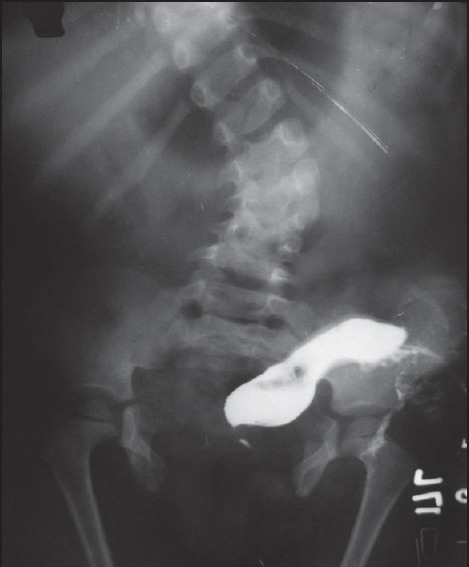
Distal colostogram showing intermediate ARM with scoliosis, spina bifida and diastasis of symphysis pubis
Intravenous urogram demonstrated a single left-sided functioning kidney draining via a ureter into a small urinary bladder positioned slightly to the left of midline. Contrast was freely coming out through the incontinent short urethra in the left phallus.
An ascending urogram was performed through the urethral opening at the right phallus, which demonstrated a small urinary bladder slightly to the right of midline. Contrast was shown to enter rectum [Figure 4]. Simultaneous ascending urogram performed through both the urethral meati demonstrated two non-communicating urinary bladders lying side-by-side and communicating to the exterior through two urethrae.
Figure 4.

Ascending urogram through right urethra showing patency to bladder
An ultrasonogram of the abdomen could demonstrate a single left-sided kidney.
MRI of the abdomen and pelvis was undertaken for detailed assessment of the anatomy. The right kidney and ureter were absent. Two urinary bladders separated in the midline by a sagital muscular septum were demonstrated. The right urinary bladder was collapsed and was connected by a urethra opening at the tip of the right phallus. The left kidney and ureter were demonstrated. The left urinary bladder was distended and communicating with the urethra in the left phallus. The right testis was not visualized but the left testis was present in the left hemiscrotum. The mass in the midline was hyperintense in both T1 and T2 weighted images, suggesting a lipoma. Axial sections of the right phallus showed corpus spongiosum with urethra in the middle surrounded by corpora cavernosa all around [Figure 5].
Figure 5.
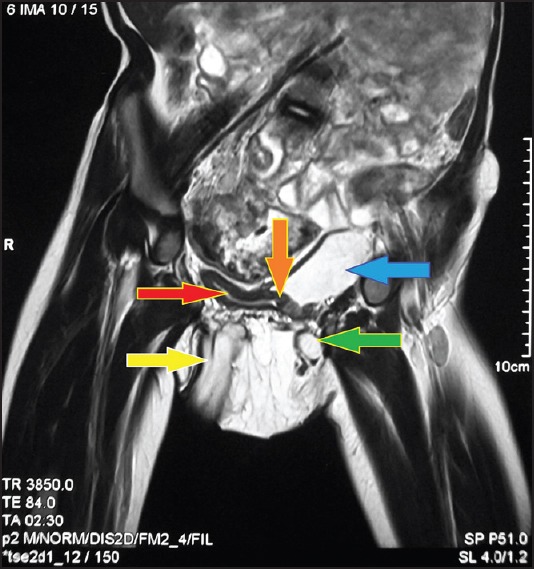
Showing MRI of abdomen and pelvis showing collapsed right bladder{red arrow},right phallus{yellow arrow},distended left bladder{blue arrow} and left phallus{green arrow} and midline septum{orange arrow}
DISCUSSION
Complete duplication of the urinary bladder is a rare anomaly with only about 50 reported cases.[1] The cause of complete duplication of the urinary bladder remains obscure although a few hypotheses have been proposed. Abrahamson[2] offers two explanations:
Excessive constriction between the urogenital and vesicourethral portions of the ventral cloaca.
A supernumerary cloacal septum that indents the epithelial of the urinary bladder.
Duplication of the urinary bladder may occur in the sagittal or coronal plane. In the coronal plane duplication of 2 urinary bladders lies one in front of the other and are separated by a fibromuscular septum that runs obliquely in a posterosuperior to anteroinferior plane. Each urethra originates from a separate urinary bladder.
In sagittal duplication two urinary bladders lie side-by-side and are separated by a muscular wall, as in our case. In this type, each urinary bladder receives the ureter of the ipsilateral kidney and is drained by its own urethra, with the ureter and urethra lying side-by-side.[3] In our case although each bladder have their own urethra but there is no kidney and ureter on right side and also right testes and vas are absent which make our case further rare.
Although the exact etiology of renal agenesis is unknown, there are various theories put forward to explain it.[4] Embryologically, male genitourinary system is derived from the mesonephric (Wolffian) duct and is under the influence of testosterone from fetal testis. Ureteric buds, derived from the mesonephric ducts, fuse with the metanephros at 32 days to begin nephrogenesis. Therefore, unilateral renal agenesis could be due to the absence of metanephricblastema, ureteral bud maldevelopment, or lack of induction of the metanephros by the ureteral bud. Since the development of urinary and genital systems is closely interlinked, renal agenesis may be associated with ipsilateral urogenital anomalies.[4]
Associated congenital anomalies with duplication of bladder include some type of duplication of the external genitalia; duplication of the vagina and urethra, as well as duplication of the lower gastrointestinal tract and fistulas between the rectum, vagina, and urethra.[5] Associated skeletal anomalies are diastasis of symphysis pubis, complete duplication of the lower lumbar vertebral column, spina bifida, and meningocele.[6] Many of these anomalies are also associated with our case.
Due to paucity of cases in printed literature, there is no uniformity in the treatment plan. Mirshemirani et al, in their articale suggested various treatment options depending on the clinical situation and associated anomalies.[7] We have planned to manage the case in staged manner. In neonatal period boy underwent emergency colostomy for ARM. Unfortunately, after that he lost to follow-up and came back again after 3 years. Now he has underwent PSARP with rectovesical fistula closure. In next stage, we are planning to reconstruct genitourinary structures (cysto-urethra-phalloplasty and scrotoplasty) with excision of lipomatous mass and colostomy closure.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Berrocal T, Novak S, Arjonilla A, Gutiérrez J, Prieto C, Urrutia MJ. Complete duplication of bladder and urethra in the coronal plane in a girl: Case report and review of the literature. PediatrRadiol. 1999;29:171–3. doi: 10.1007/s002470050564. [DOI] [PubMed] [Google Scholar]
- 2.Abrahamson J. Double bladder and related anomalies: Clinical and embryological aspects and a case report. Br J Urol. 1961;33:195–8. doi: 10.1111/j.1464-410x.1961.tb11606.x. [DOI] [PubMed] [Google Scholar]
- 3.Hoffman AD, Leroy AJ. Uroradiology: Procedures and anatomy. In: Kelalis PP, King LR, Belman AB, editors. Clinical pediatric urology. 3rd ed. Philadelphia, PA: Saunders; 1992. pp. 66–116. [Google Scholar]
- 4.Kumar KV, Rao BS, Shiradhonkar S, Jha R, Narayan G, Modi KD. The right sided syndrome, congenital absence of kidney and testis. Saudi J Kidney Dis Transpl. 2011;22:315–8. [PubMed] [Google Scholar]
- 5.Ciftci AO, Senocak ME, Büyükpamukçu N, Hiçsönmez A. Complete duplication of the bladder and urethra: A case report and review of the literature. J Pediatr Surg. 1995;30:1605–6. doi: 10.1016/0022-3468(95)90168-x. [DOI] [PubMed] [Google Scholar]
- 6.Ravitch MM. Hindgut duplication-Doubling of colon and Genital Urinary tracts. Ann Surg. 1953;137:588–601. doi: 10.1097/00000658-195305000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mirshemirani AR, Sadeghyian N, Mohajerzadeh L, Molayee H, Ghaffari P. Diphallus: Report on six cases and review of the literature. Iran J Pediatr. 2010;20:353–7. [PMC free article] [PubMed] [Google Scholar]