

Abstract
Background:
Orthopedic injuries are among the most common causes of mortality, morbidity, hospitalization, and economic burden in societies.
Objectives:
In this research, we study the prevalence of different types of trauma requiring orthopedic surgery.
Patients and Methods:
We conducted a cross-sectional study on 2582 patients with acute orthopedic injuries admitted to the orthopedic emergency ward at the Poursina Hospital (a referral center in Guilan province (northern Iran), during December 2010 through September 2011. Patients were examined and the data collection form was filled for each patient. Data were analyzed by SPSS software version 19 and were listed in tables.
Results:
Of 2582 included cases, 1940 were male and 642 were female, with a mean age of 34.5 years. Most injuries were seen in the 25 to 44 year age group from rural areas. The highest frequency of trauma related to falls. On the other hand, bicycling and shooting had the lowest frequencies. There were 18 cases with limb amputation. Overall, 66.5% of patients had fractures, 5% had soft tissue lacerations, and 10% had dislocations.
Conclusions:
Identification of risk factors and methods of prevention is one of the most important duties of healthcare systems. Devising plans to minimize these risk factors and familiarizing people with them is prudent.
Keywords: Orthopedics; Wounds and Injuries; Fractures, Bone
1. Background
Injuries due to different kinds of trauma are one of the major causes of mortality and disability around the world (1). The World Health Organization (WHO) considered trauma an important issue that merits more attention (2). Injuries caused by traffic accidents in developing and developed countries are social problems that result in wasting of human and financial resources (3). Approximately five million people die annually (570 individuals per hour) in accidents that can be prevented (4). Orthopedic injuries (including soft tissue, muscle, or bone injuries) are the most common injuries in traffic accidents and other types of accidents (5). Today, orthopedic traumas needing surgery are significantly increasing and impose significant individual and social disabilities, loss of work days and less social activities (6, 7). Despite abundant epidemiologic data on the nature of such injuries, there are few studies focusing on specific age groups, different types of orthopedic injuries, and/or differences in age, gender and trauma etiology. Because of the geographical location of Guilan province, road situation, frequent rainfall, rural lifestyle, forest homes, mountainous terrain and excessive use of vehicles without safety gear such as motorcycle, tractor, etc., this region is one the most trauma predisposing provinces of Iran (8).
2. Objectives
In this study, we assessed the prevalence of different types of trauma needing orthopedic operations. Data relevant to the association of age, gender, place of living, occupation, and trauma mechanism with the injury severity were analyzed.
3. Patients and Methods
This cross-sectional study assessed patients with various age groups admitted to the orthopedic ward and who underwent emergency orthopedic surgery due to fractures, lacerations, and/or fractures with lacerations from December 2010 to September 2011. Patients with severe head trauma, cases who needed emergency neurosurgery or immediate abdominal surgery, those transferred to the intensive care unit, patients who died in emergency room, and cases who had bone fractures at least six months prior to the current trauma were excluded from the study. The orthopedic surgeons who were on-call during the study period examined the patients. Two general physicians who were involved in this study filled a special form consisting of clinical orthopedic and demographic data of the patients. In the demographic section, data about age group, gender, occupation, place of residence and education level were recorded. In the specialized orthopedic section, information regarding the time of injury, trauma mechanism, fracture or dislocation site, tendon injury, length and depth of the laceration, and any neural and vascular injury was recorded. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the institution's Human Research Committee. After data collection, information was organized using descriptive statistics, frequency tables, and diagrams. SPSS software version 19 was used in data analysis. Qualitative data were analyzed using chi-square and quantitative data with t-test. In all tests, P < 0.05 was considered statistically significant.
4. Results
During the study period, 2582 individuals were assessed (642 females and 1940 males). The mean age of subjects was 34.5 (from one year old to 90 years old). The number of patients from rural and urban areas was 77% and 23%, respectively. There were 103 visitors and others were local residents. Only 3.4% of patients had academic education. Seventy-eight patients were outpatients. Overall, 1925 and 579 patients were transferred to the hospital by car and ambulance, respectively. Most of the injuries were seen at rush hour traffic peaks (16 to 20 p.m.). The number of patients with fractures, lacerations, and dislocations were 1718, 1342, and 258, respectively. Many patients had several simultaneous complications. Limb amputation occurred in 18 patients (seven cases with fingertip amputation, one case with wrist amputation, four cases with distal phalanx amputation, two cases with through phalanx amputation, one case with foot amputation, two cases with toe amputation, and one case with thumb amputation from the proximal interphalangeal joint. In addition, vascular, tendon, and nerve injuries were seen in 98, 289, and 83 patients respectively. The majority of vascular injuries were managed with simple compressive dressing or ligation. Only six patients underwent vascular surgery for arterial repair. Figure 1 shows various complications in different age groups. According to this chart, the highest frequency of orthopedic trauma was in the 25-44 year of age group (n = 824). Chi square test showed that there was a significant association between open fracture and nerve (P < 0.05), vascular (P < 0.05), and tendon (P < 0.05) injuries. The frequency and distribution of injury mechanisms and related complications are shown in Figure 2. The highest frequency of injury related to falls (n = 982). Moreover, the most open fractures were observed among motorcyclists (n = 169). Open and closed fractures were observed in 532 and 1810 patients, respectively. In addition, 1154 patients had upper limb fracture, 512 patients had lower limb fractures, and 52 patients had both upper and lower limb injuries. Tables 1 and 2 show the frequency of fractures and dislocations in bones of the upper and lower limbs.
Figure 1. The Distribution of Various Types of Injuries in Different Age Groups.
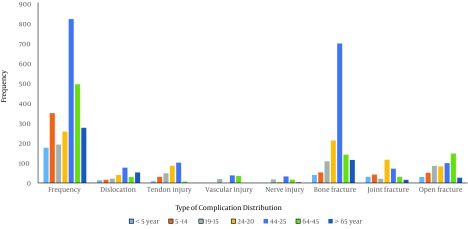
Figure 2. The Frequency of Different Injuries and Etiological Distribution.
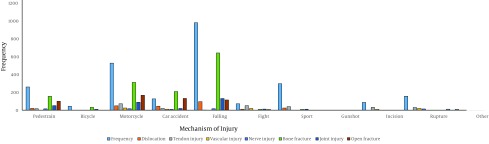
Table 1. Location of Fractures in Upper Limbs.
| Location | No. |
|---|---|
| Clavicle | |
| Medial End | 6 |
| Body | 26 |
| Lateral End | 14 |
| Scapula | 5 |
| Humerus | |
| Proximal | 40 |
| Shaft | 67 |
| Distal | 58 |
| Elbow | 28 |
| Isolated Radius | |
| Head | 8 |
| Trunk | 83 |
| Distal | 473 |
| Isolated Ulna | |
| Proximal | 6 |
| Trunk | 86 |
| Distal | 57 |
| Double Fracture of Radius and Ulna | 168 |
| Hand | |
| Metacarpals | 145 |
| Fingers | 77 |
Table 2. Location of Fractures in Lower Limb.
| Location | No. |
|---|---|
| Pelvic | |
| Pubis | 6 |
| Coccyx | 0 |
| Sacrum | 2 |
| Acetabulum | 29 |
| Ilium | 10 |
| Femur | |
| Neck | 44 |
| Trochanteric | 99 |
| Shaft | 131 |
| Distal | 19 |
| Knee | |
| Patella | 36 |
| Hemarthrosis | 12 |
| Joint Instability | 1 |
| Isolated Tibia | |
| Proximal | 12 |
| Body | 44 |
| Distal | 9 |
| Isolated Fibula | |
| Head | 1 |
| Body | 6 |
| Distal | 5 |
| Double Fracture of Tibia and Fibula | 86 |
| Ankle | |
| Medial | 12 |
| Lateral | 26 |
| Bimalleolar | 19 |
| Trimalleolar | 14 |
| Foot | |
| Talus/Calcaneus | 23 |
| Tarsometatarsal Dislocation/Tarsometatarsal dislocation | 3 |
| Metatarsal | 97 |
| Fingers | 25 |
5. Discussion
In this study, most orthopedic traumas were observed in the 25 to 44 year age group (31.9%). The frequency of injuries in males was more than in females (75.1% male vs. 24.9% female) which was similar to the results obtained in other studies (8-10). The main reason may be the greater tendency of males toward taking risks and more participation in outdoor activities. The main etiology relate to manual activities and labor, as well as domestic violence and sometimes firearms (all more common among males). In addition, cars and motorcycles are more common among males than females in the society. Despite our assumption that most orthopedic traumas are related to accidents, especially motorcyclists, results of this study indicated that the highest frequency was related to traumas caused by falling (38.03%). Motorcycle trauma had the second highest frequency (18.5%). In addition, the lowest frequency was related to gunshot trauma (0.5%) and bicyclists (0.8%). Falls were due to foothills and terrains of Guilan where most villages are located and the rural residents live on agriculture, gardening and labor. The wet climate and slippery roads increase the risk of falling. On the other hand, using motorcycles is prevalent in this province. In order to improve the safety conditions at work and reduce these risks, appropriate strategies must be employed. Television and national media can play a role in the preventing injury. In addition, the government can reduce many of these financial losses and fatalities by improving road conditions, reducing manual work, and substituting it with modern machinery. Moreover, statistics indicate that from 100000 individuals, 237 are hospitalized and 38 die annually (11). The statistics show that motorcyclists’ safety and public awareness is not well established. The necessity of using motorcycle helmets, not traveling on highways, reducing traffic in streets especially in rush hours, and strict supervision of traffic regulations are important issues that should be implemented widely in the society in order to reduce the number of accidents.
Despite the fact that in different studies the most prevalent fractures were femur and hip injuries (8, 12, 13), the most prevalent injury in our study was the fracture of distal radius. Double fracture (Tibia and Fibula fractures or Radius and Ulna fractures at the same time) is an injury that only occurs following high-energy traumas and in most cases, it is accompanied by severe soft tissue injuries. This kind of fracture in our study, Double fracture of the Radius and Ulna was 6.5%; Double fracture of Tibia and Fibula was 3.33%. In addition, the frequency of distal radius fracture is due to fact that it relates to falling. Most of tendon, vascular, and nerve injuries occurred in the 25 to 44-year age group in males with open fractures and lacerations. These results show the importance of precise examination of patients after trauma and during hospitalization. Some of these associated injuries in patients referred to the emergency ward remained undiagnosed due to the lack of precise history taking and incomplete examinations. This may result in numerous complication in the future. On time presence and precise diagnosis of injuries by interns and residents in the emergency ward can be very beneficial. Mortality rate is higher in patients with several simultaneous fractures and soft tissue injuries. After the completion of the treatment period in these patients, it was seen that their life quality was decreased for different reasons such as joint stiffness and osteoarthritis following trauma. This indicates that identification of risk factors and preventive measures in traumas is one of the most important priorities to consider by the healthcare system of each country.
Acknowledgments
The authors express their gratitude to Mr. Haghiri-Limudahi for critical reading of the manuscript and for the insightful suggestions.
Footnotes
Authors’ Contributions:Author: Mehran Soleymanha; data collection: Mohammadreza Mobayen and Alborz Adeli; draft: Kamran Asadi; analysis: Zahra Haghparast-Ghadim-Limudahi.
Funding/Support:This study was supported by the Orthopedic Research Center of Poursina Hospital in Rasht.
References
- 1.Harrington DT, Connolly M, Biffl WL, Majercik SD, Cioffi WG. Transfer times to definitive care facilities are too long: a consequence of an immature trauma system. Ann Surg. 2005;241(6):961–6. doi: 10.1097/01.sla.0000164178.62726.f1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Toroyan T, Peden MM, Iaych K. WHO launches second global status report on road safety. Inj Prev. 2013;19(2):150. doi: 10.1136/injuryprev-2013-040775. [DOI] [PubMed] [Google Scholar]
- 3.Sankaran-Kutty M, Bener A, Muralikuttan KP, Sebastian M. Road traffic accident admissions in the United Arab Emirates. Ann Saudi Med. 1998;18(4):349–51. doi: 10.5144/0256-4947.1998.349. [DOI] [PubMed] [Google Scholar]
- 4.Celso B, Tepas J, Langland-Orban B, Pracht E, Papa L, Lottenberg L, et al. A systematic review and meta-analysis comparing outcome of severely injured patients treated in trauma centers following the establishment of trauma systems. J Trauma. 2006;60(2):371–8. doi: 10.1097/01.ta.0000197916.99629.eb. [DOI] [PubMed] [Google Scholar]
- 5.Regel G, Lobenhoffer P, Grotz M, Pape HC, Lehmann U, Tscherne H. Treatment results of patients with multiple trauma: an analysis of 3406 cases treated between 1972 and 1991 at a German Level I Trauma Center. J Trauma. 1995;38(1):70–8. doi: 10.1097/00005373-199501000-00020. [DOI] [PubMed] [Google Scholar]
- 6.Gomberg BFC, Gruen GS, Smith WR, Spott MA. Outcomes in acute orthopaedic trauma: a review of 130,506 patients by age. Injury. 1999;30(6):431–7. doi: 10.1016/s0020-1383(99)00138-2. [DOI] [PubMed] [Google Scholar]
- 7.Urquhart DM, Edwards ER, Graves SE, Williamson OD, McNeil JJ, Kossmann T, et al. Characterisation of orthopaedic trauma admitted to adult level 1 trauma centres. Injury. 2006;37(2):120–7. doi: 10.1016/j.injury.2005.10.016. [DOI] [PubMed] [Google Scholar]
- 8.Hemmati H, Chabok S, Dehnadimoghadam A, Melksari H, Dafchahi M, Shabani S. Trauma in Guilan (North of Iran): An Epidemiologic Study. Acta Med Iran. 2009;47(5):403–8. [Google Scholar]
- 9.Brinker MR, O'Connor DP. The incidence of fractures and dislocations referred for orthopaedic services in a capitated population. J Bone Joint. 2004;86(2):290–7. [PubMed] [Google Scholar]
- 10.Karbakhsh M, Zandi NS, Rouzrokh M, Zarei MR. Injury epidemiology in Kermanshah: the National Trauma Project in Islamic Republic of Iran. East Mediterr Health J. 2009;15(1):57–64. [PubMed] [Google Scholar]
- 11.Carr BG, Branas CC. Time, distance, and access to emergency care in the United States. LDI Issue Brief. 2009;14(4):1–4. [PubMed] [Google Scholar]
- 12.Elmi A, Ganjpour Sales J, Tabrizi A, Soleimanpour J, Mohseni MA. Orthopedic injuries following the East azerbaijan earthquake. Trauma Mon. 2013;18(1):3–7. doi: 10.5812/traumamon.8322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dehghani M, Teimouri M, Eshaghi MA, Sohrabi F. [Accuracy of the Preoperative Examination of Glass Injury to the Forearm and Wrist]. J Isfahan Med School. 2010;28(110):467–71. [Google Scholar]