

Diabetes mellitus is a serious metabolic disease, affecting people of all geographic, ethnic or racial origin and its prevalence is increasing globally1. Burden from this costly disease is high on the low and middle income countries (LMIC) where the impacts of modernization and urbanization have caused marked adverse changes in lifestyle parameters.
In 2013, of the estimated 382 million people with diabetes globally, more than 80 per cent lived in LMIC. It was estimated that India had 65.1 million adults with diabetes in 2013, and had the 2nd position among the top 10 countries with the largest number of diabetes. This number is predicted to increase to 109 million by 2035 unless steps are taken to prevent new cases of diabetes1. Primary prevention of diabetes is feasible and strategies such as lifestyle modification are shown to be effective in populations of varied ethnicity2,3. However, for implementation of the strategies at the population level, national programmes which are culturally and socially acceptable and practical have to be formulated which are currently lacking in most of the developed and developing countries. Early diagnosis and institution of appropriate therapeutic measures yield the desired glycaemic outcomes and prevent the vascular complications4.
Type 2 diabetes which accounts for 85-95 per cent of all diabetes has a latent, asymptomatic period of sub-clinical stages which often remains undiagnosed for several years1. As a result, in many patients the vascular complications are already present at the time of diagnosis of diabetes, which is often detected by an opportunistic testing. Asian populations in general, particularly Asian Indians have a high risk of developing diabetes at a younger age when compared with the western populations5. Therefore, it is essential that efforts are made to diagnose diabetes early so that the long term sufferings by the patients and the societal burden can be considerably mitigated.
Risk factors for diabetes
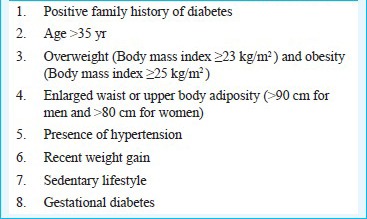
Many studies have shown that awareness about the diabetes and its complications is poor among the general population specially in the rural areas6,7. There is an urgent need to create awareness among the population regarding diabetes and about the serious consequences of this chronic disorder. Epidemiological data from India have shown the presence of a number of risk factors which can be easily identified by simple non-invasive risk scores8,9. The major risk factors are listed in Box 1.
Box 1.
Major risk factors for type 2 diabetes in Indians
Signs and symptoms of diabetes
The signs and symptoms of diabetes are disregarded by many because of the chronic progression of the disease. People do not consider this as a serious problem because unlike many other diseases the consequences of hyperglycaemia are not manifested immediately. People are not aware that damage can start several years before symptoms become noticeable. This is unfortunate because recognition of early symptoms can help to get the disease under control immediately and to prevent vascular complications.
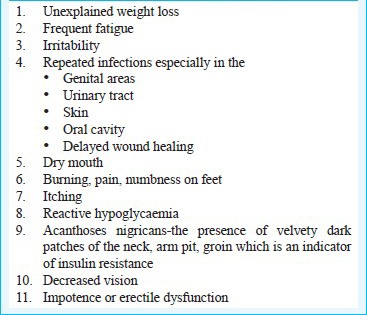
Warning signs & classic symptoms of diabetes
Considering the asymptomatic nature of type 2 diabetes in the early stages, it is essential that the people are educated on its warning signs (Box 2).
Box 2.
Warning signs of diabetes
The classic symptoms of diabetes such as polyuria, polydypsia and polyphagia occur commonly in type 1 diabetes, which has a rapid development of severe hyperglycaemia and also in type 2 diabetes with very high levels of hyperglycaemia. Severe weight loss is common only in type 1 diabetes or if type 2 diabetes remains undetected for a long period. Unexplained weight loss, fatigue and restlessness and body pain are also common signs of undetected diabetes. Symptoms that are mild or have gradual development could also remain unnoticed.
Screening test for diabetes
A person of Asian origin aged 35 yr or more with two or more of the above risk factors, should undergo a screening test for diabetes. An oral glucose tolerance test (OGTT) is commonly used as the screening test10. Fasting and 2 h post glucose tests can identify impaired fasting glucose (IFG) (fasting glucose >110 - <125 mg/dl), impaired glucose tolerance (IGT) (2 h glucose >140-<200 mg/dl) and presence of diabetes (fasting > 126 and 2 h glucose >200 mg/dl). If a random blood glucose value is > 150 mg/dl, further confirmation by an OGTT is warranted. Recently, glycosylated haemoglobin (HbA1c) has been recommended as the test for diagnosis of diabetes (>6.5%). Presence of pre-diabetes is indicated by HbA1c values between 5.7 - 6.4 per cent11.
Screening for undiagnosed T2DM is recommended at the first prenatal visit in women with above risk factors, using standard diagnostic method criteria. Screening for gestational diabetes (GDM) at 24-28 wk of gestation is recommended in women who do not have previous history of diabetes, as GDM remains asymptomatic11. A history of GDM carries a high risk for developing diabetes.
Significance of identifying prediabetes
Even prediabetic stages such as IFG and IGT carry high risk for vascular complications such as cardiovascular diseases. The recent estimates by the International Diabetes Federation (IDF)1 indicate that globally there are more than 316 million people (6.9%) with IGT. Among them, more than 70 per cent live in LMIC1.
It is also important to note that currently one third of those who have IGT are in the productive age between 20-39 yr and, therefore, are likely to spend many years at high risk of developing diabetes and/or complications of diabetes1. Some persons with prediabetes experience reactive hypoglycaemia 2-3 hours after a meal. This is a sign of impaired insulin metabolism indicative of impending occurrence of diabetes. Therefore, periodic medical check-up in people with such signs or risk factors for diabetes would reduce the hazards involved in having undiagnosed diabetes. It would help improve the health status of a large number of people who otherwise would be silent sufferers from the metabolic aberrations associated with diabetes.
Conclusions
Awareness about the signs and symptoms and periodic screening especially in the presence of risk factors and warning signs of diabetes, would go a long way in preventing new cases of diabetes by providing an opportunity to intervene at the stage of prediabetes. It is evident that diabetes can be prevented among prediabetic individuals by improvements in physical activity and diet habits. Such strategies will also prevent development of diabetic complications to a great extent. Patient empowerment is vital in diabetes management. This can be done through patient education and sharing information on management and preventive aspects of diabetes.
References
- 1.IDF Diabetes Atlas. International Diabetes Federation. 6th ed. 2013. [accessed on January 6, 2014]. Available from: www. idf.org/diabetesatlas .
- 2.Alberti KGMM, Zimmet P, Shaw J. International Diabetes Federation: a consensus on type 2 diabetes prevention. Diabet Med. 2007;24:451–63. doi: 10.1111/j.1464-5491.2007.02157.x. [DOI] [PubMed] [Google Scholar]
- 3.Ramachandran A, Snehalatha A, Samith Shetty A, Nanditha A. Primary prevention of type 2 diabetes in South Asians-challenges and the way forward. Diabet Med. 2013;30:26–34. doi: 10.1111/j.1464-5491.2012.03753.x. [DOI] [PubMed] [Google Scholar]
- 4.Abdul-Ghani MA, DeFronzo RA. Pathophysiology of prediabetes. Curr Diab Rep. 2009;9:193–9. doi: 10.1007/s11892-009-0032-7. [DOI] [PubMed] [Google Scholar]
- 5.Ramachandran A, Ma RC, Snehalatha C. Diabetes in Asia. Lancet. 2010;375:408–18. doi: 10.1016/S0140-6736(09)60937-5. [DOI] [PubMed] [Google Scholar]
- 6.Murugesan N, Snehalatha C, Shobhana R, Roglic G, Ramachandran A. Awareness about diabetes and its complications in the general and diabetic population in a city in southern India. Diabetes Res Clin Pract. 2007;77:433–7. doi: 10.1016/j.diabres.2007.01.004. [DOI] [PubMed] [Google Scholar]
- 7.Mohan D, Raj D, Shanthirani CS, Datta M, Unwin NC, Kapur A, et al. Awareness and knowledge of diabetes in Chennai - the Chennai urban rural epidemiology study (CURES-9) J Assoc Physicians India. 2005;53:283–7. [PubMed] [Google Scholar]
- 8.Ramachandran A, Snehalatha C, Vijay V, Wareham NJ, Colagiuri S. Derivation and validation of diabetes risk score for urban Asian Indians. Diabetes Res Clin Pract. 2005;70:63–70. doi: 10.1016/j.diabres.2005.02.016. [DOI] [PubMed] [Google Scholar]
- 9.Mohan V, Anbalagan VP. Expanding role of the Madras Diabetes Research Foundation - Indian Diabetes Risk Score in clinical practice. Indian J Endocrinol Metab. 2013;17:31–6. doi: 10.4103/2230-8210.107825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.World Health Oorganization. Part 1: Diagnosis and classification of diabetes mellitus. Geneva: World Health Oorganization; 1999. Definition, diagnosis and classification of diabetes mellitus and its complications. Report of a WHOo Consultation. [Google Scholar]
- 11.American Diabetes Association. Standards of medical care in diabetes. Diabetes Care. 2011;34:S11–61. doi: 10.2337/dc11-S011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359:1577–89. doi: 10.1056/NEJMoa0806470. [DOI] [PubMed] [Google Scholar]