

Sir,
Scrub typhus is an infectious disease caused by Orienta tsutsugamoshi, widespread in South East Asia and Western Pacific region. The trombiculid mites, Leptotromidium diliense are known vectors of the disease. More often scrub typhus is characterized by focal or disseminated vasculitis and perivasculitis which may involve lungs, liver, heart, spleen and the central nervous system1. The severity of the symptoms varies widely depending on the susceptibility of the host, virulence of the strain or both1. The clinical profile among patients is non-specific, especially in endemic areas2,3. An estimated one million cases occur annually and one billion people may be at risk4,5.
The incidence of scrub typhus is especially high during the cooler months of the year6. However, the occurrence of scrub typhus in southern India has been reported during summer months also (April and May)7. Due to the wide prevalence of scrub typhus in this area, the need for its consideration in the differential diagnosis has been emphasized8,9. Hence this study was conducted among 80 consecutive patients with fever of unknown aetiology and recent history of febrile illness attending the outpatient and inpatient departments of Medical College Hospital at Vellore in Tamil Nadu during April to June 2012 for serological diagnosis of scrub typhus. The serum samples were analysed for scrub typhus using IgM ELISA (InBios International; Inc., Netherlands) in the microbiology department. The absorbance was read at 450 nm. The cut-off value was calculated by determining the average of optical density (OD) plus three times of the standard deviation (SD) of normal human serum. Samples with OD > 0.400 were considered as positive. Chi-square test was used to compare the difference in occurrence of scrub typhus between male and female patients.
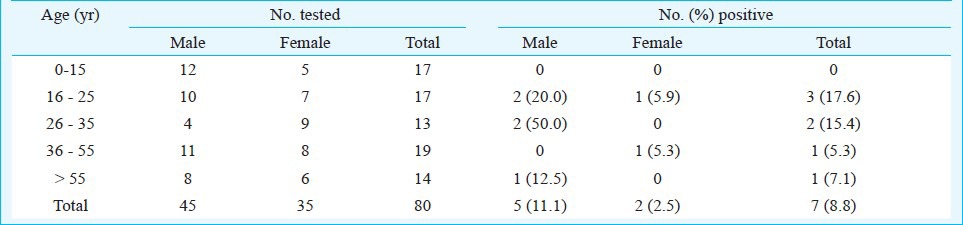
Overall, seven (8.8%) of the 80 samples tested were positive for scrub typhus. The percentage of samples positive among males (n=45) and females (n=35) were 11.1 and 2.5 per cent, respectively. The gender difference was not significant. The age profile data suggested that while none among the age group of 0-15 yr was positive, the percentage of people positive for scrub typhus was highest (17.6%) in the age group 16-25 yr followed by (15.4%) in 26-35 yr (Table).
Table.
Seropositivity for scrub typhus among samples tested
The present study documented the detection of scrub typhus among patients reporting with febrile illness at the hospital. It also provided evidence on its occurance in and around Vellore during summer months as reported earlier10. Fever and body pain predominated in majority (6 of 7) of positive cases with duration of fever ranging from 5 to 25 days. Classical eschar associated with scrub typhus is usually found on Caucasian & East Asian patients but it is seen less frequently in south Asians especially those who are dark skinned11. In the present study, none of the patients had history of a characteristic eschar.
The government hospitals and medical college hospitals attract large number of patients from both rural and urban areas. Routine serological diagnosis would not only fecilitate prompt and early detection but also help prevent and manage complications due to scrub typhus.
Acknowledgment
The authors acknowledge the assistance rendered by the Institute of Vector Control and Zoonoses, Hosur, in serological diagnosis of samples for scrub typhus.
References
- 1.Saah AJ. Orietia tsutasugamushi. In: Mandall GL, Bennett JE, Dolin R, editors. Principles and practice of infectious disease’. 5th ed. philadelphia, PA: churchill livingstone; 2000. pp. 2056–7. [Google Scholar]
- 2.Krishnan KV, Smith RO. clinical features and laboratory diagnosis of XK or mites borne typhus as observed in 102 cases in Barrackpure area. Indian Med Gazett. 1946;78:33–8. [PMC free article] [PubMed] [Google Scholar]
- 3.Kalra SL. Natural history of typhus fevers in India. Indian J Med Sci. 1952;6:569–74. [Google Scholar]
- 4.Mahajan SK. Scrub typhus. J Assoc Physicians India. 2005;53:954–8. [PubMed] [Google Scholar]
- 5.Watt G, Jongsakul K, Suttinont C. Possible scrub typhus coinfection in Thai agriculture worker hospitalised with leptospirosis. Am J Trop Med Hyg. 2003;68:89–91. [PubMed] [Google Scholar]
- 6.Mathai E, Rolain JM, Verghese GM, Abraham OC, Mathai M, Raoult D, et al. Outbreak of scrub typhus in southern India during the cooler months. Ann ny Acad Sci. 2003;990:59–364. doi: 10.1111/j.1749-6632.2003.tb07391.x. [DOI] [PubMed] [Google Scholar]
- 7.Varghese GM, Abraham DC, Mathai D, Thomas K, Aaron R, Kavita ML, et al. Scrub typhus among hospitalized patients with febrile illness in South India. Magnitude & clinical predictors. J Infect. 2006;52:56–60. doi: 10.1016/j.jinf.2005.02.001. [DOI] [PubMed] [Google Scholar]
- 8.Kamarasu K, Malathi M, Rajagopal V, Subramani K, Jagadeeshramasamy D, Mathai E. Serological evidence for wide distribution of spotted fevers & typhus fever in Tamil Nadu. Indian J Med Res. 2007;126:128–30. [PubMed] [Google Scholar]
- 9.Murali N, Pillai S, Cherian T, Raghupathy P, Padmini V, Matha E. Rickettsial infections in South India-how to spot the spotted fever. Indian Pediatr. 2001;38:1393–6. [PubMed] [Google Scholar]
- 10.Mathai E, Lloyd G, Cherian T, Abraham OC, Cherian AM. Serological evidence for the continued presence of human rickettsioses in southern India. Ann Trop Med Parasitol. 2001;95:395–8. doi: 10.1080/00034980120065804. [DOI] [PubMed] [Google Scholar]
- 11.Sharma A, Mahajan S, Gupta ML, Kanga A, Sharma V. Investigation of an outbreak of scrub typhus in the Himalayan Region of India. Jpn J Infect Dis. 2005;58:208–10. [PubMed] [Google Scholar]