

Abstract
Intrauterine contraceptive devices (IUCD) have been associated with the multitude of complications. We present a rare case report of a 30-year-old female in whom the IUCD (Cu-T) migrated into the urinary bladder leading to calculus formation. The migrated IUCD encrusted with stones was successfully retrieved.
Keywords: Intrauterine contraceptive devices, uterine perforation, vesical calculus
Introduction
Intrauterine contraceptive devices (IUCD) are widely used reversible contraceptive method and are cost-effective and have low complication rates.[1,2] Uterine perforation during the insertion is an uncommon complication of IUCD and its incidence range from 0 to 1.6/1000 insertion.[3] Perforation of the uterus and intravesical migration is extremely rare. Once the IUCD has penetrated the bladder, it usually becomes encrusted with calculi and associated with lower urinary tract symptoms.[1,2,3,4,5] In this report, we present a case in which the IUCD perforated the uterus and migrated to the bladder, which was encrusted with calculi at the time of diagnosis, and the patient presented with severe dysuria.
Case Report
A 30-year-old female gravid 4, para 3 came to the gynaecology outpatient department with 11/2 months history of pain in suprapubic region with severe dysuria. She also gave a history of off and on suprapubic pain from last 4 years. Patient had amenorrhea of 11/2 months for which she had taken Medical Termination pill and now she had bleeding per vaginum. She had undergone ultrasonography to rule out retained products, which revealed dense acoustic shadows in the urinary bladder s/o? calculi [Figures 1 and 2]. Uterus and ovaries were unremarkable. Further X-ray kidneys, ureters, and bladder (KUB) was done, which revealed a Copper-T (Cu-T) in the pelvic region with fine radio opacities along the margins of Cu-T thereby suggesting an intravesical Cu-T (manufacturer detail not known) [Figure 3]. Magnetic resonance examination revealed Cu-T in the urinary bladder. There was no fistulous tract between the uterus and urinary bladder. Fat planes between the urinary bladder and uterus were maintained. Cervix and vagina were unremarkable [Figure 4a and b]. Her medical history revealed insertion of Cu-T 5 years back, but was not aware of its expulsion.
Figure 1.

Ultrasonography showing intravesical dense acoustic shadows s/o calculi
Figure 2.

Ultrasonography showing normal uterine cavity
Figure 3.

X-ray showing intrauterine contraceptive devices in the pelvis with fine opacities
Figure 4.
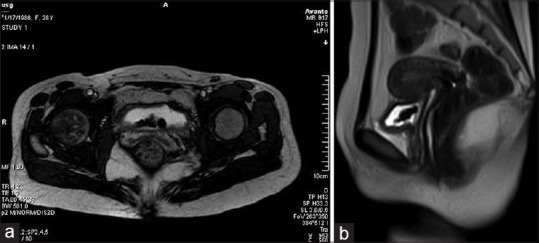
(a) T2-weighted axial image showing partially distended urinary bladder with hypo intense intrauterine contraceptive devices. (b) T2-weighted sagittal image showing uterus with normal morphology. No fistulous tract seen between uterine bleeding (UB) and uterus. Hypo intense intrauterine contraceptive devices seen in the UB
Cystoscopy revealed an impacted T-shaped device encrusted with yellowish material within the urinary bladder, which could not be removed cystoscopically. Hence, cystostomy was done and IUCD was removed [Figure 5]. Postoperative period was uneventful and the patient was discharged in a satisfactory condition.
Figure 5.

T-shaped intrauterine contraceptive devices removed after cystostomy encrusted with yellowish material suggestive of calculi
Discussion
Intrauterine contraceptive devices is the most popular method of reversible contraception due to its high efficacy for fertility regulation, low-risk, and low-cost.[5] Complications with IUCDs remain rare. These include spontaneous abortion, pelvic inflammatory disease (PID), uterine perforation, heavy bleeding, dysmenorrhea, and unplanned pregnancy. The rate of spontaneous abortion is doubled. The risk of PID is increased 10-13% with IUCD in situ.
The rate of uterine perforation has been estimated between 0 and 1.60/10,000 insertions. The pathogenesis of uterine perforation of IUCD may occur by two mechanisms. First, uterine perforation can occur at the time of insertion, especially when associated with severe abdominal pain.[3,6,7] Second, proposed mechanism of perforation is by a gradual pressure necrosis of the uterine wall by IUCD (likely at its lead point) with essential migration out of the uterus. Migration and perforation may or may not be facilitated by uterine contractions.[3,7] About 80% of uterine perforation are free in the peritoneal cavity. IUCD migration into adjacent organs leads to bowel obstruction, perforation peritoneal, appendicitis, vesical calculus formation, obstructive nephropathy, fistula formation, menouria and intra peritoneal adhesions leading to infertility.[3,8,9]
In 1992, Dietrich reported eight cases of intravesical IUCD migration with development of urinary symptoms as early as 3 months to as late as 5 years after insertion.[1] Our patient was also having off and on suprapubic pain with dysuria for last 4 years. These urinary symptoms are related to migration of IUCD into the urinary bladder. The presence of IUCD in bladder leads to calculus formation overtime. The degree of stone formation is variable and independent of the duration in the bladder.[2,6]
The device can either be partially or completely encrusted with calculi.[5] In our patient, there was complete encrustation of the device. It has also been suggested that pregnancy helps in erosion of the uterine wall with IUCD and therefore secondary perforation is considered to be the most likelihood mechanism.[5] Our data supports this hypothesis as pregnancy had occurred after insertion of IUCD.
Sonography with transabdominal and transvaginal is a useful method to detect IUCD migration as well as encrustation of calculi, which can be well-diagnosed by the presence of calculus in plain X-ray KUB. In our case also the IUCD showed encrustation which was seen as fine calcification on plain X-ray. Computed tomography scan is also a very effective imaging modality in demonstrating IUCD relation with adjacent structures. Magnetic resonance image further delineates fistulous tracts between the uterine and urinary bladder.
Treatment option for IUCD removal varies. Cystoscopic extraction of the device and stones is preferred as there is less morbidity with high success rate.[2] However, in our case, the removal was not possible cystoscopically, and cystostomy was performed for removal of IUCD. Lithotripsy of bladder stones may be required preceding the extractions in large stones.[6]
Conclusion
Chronic pelvic pain and dysfunctional voiding symptoms with a history of an unretrieved IUCD must be carefully researched for possible perforation of the uterus with intravesical migration of IUCD. Any displaced IUCD should be removed due to potential complications.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Dietrick DD, Issa MM, Kabalin JN, Bassett JB. Intravesical migration of intrauterine device. J Urol. 1992;147:132–4. doi: 10.1016/s0022-5347(17)37159-8. [DOI] [PubMed] [Google Scholar]
- 2.Ghanem MA, Sultan SM, Ghanem AA, Zantay FM. Double Intravesical Migration of Intrauterine Device: Presented With Vesical Stone Formation [Google Scholar]
- 3.Gillis E, Chhiv N, Kang S, Sayegh R, Lotfipour S. Case of urethral foreign body: IUD perforation of the bladder with calculus formation. Cal J Emerg Med. 2006;7:47–53. [PMC free article] [PubMed] [Google Scholar]
- 4.Ozgür A, Sismanoglu A, Yazici C, Cosar E, Tezen D, Ilker Y. Intravesical stone formation on intrauterine contraceptive device. Int Urol Nephrol. 2004;36:345–8. doi: 10.1007/s11255-004-0747-y. [DOI] [PubMed] [Google Scholar]
- 5.Sataa S, Sami BR, Sabeur R, Karim C, Ali H. Bladder calculus resulting from the migration of an intrauterine contraceptive device: A report of ten cases. Int J Nephrol Urol. 2011;3:54–61. [Google Scholar]
- 6.Tosun M, Celik H, Yavuz E, Cetinkaya MB. Intravesical migration of an intrauterine device detected in a pregnant woman. Can Urol Assoc J. 2010;4:E141–3. doi: 10.5489/cuaj.938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Caspi B, Rabinerson D, Appelman Z, Kaplan B. Penetration of the bladder by a perforating intrauterine contraceptive device: A sonographic diagnosis. Ultrasound Obstet Gynecol. 1996;7:458–60. doi: 10.1046/j.1469-0705.1996.07060458.x. [DOI] [PubMed] [Google Scholar]
- 8.Zakin D, Stern WZ, Rosenblatt R. Complete and partial uterine perforation and embedding following insertion of intrauterine devices. I. Classification, complications, mechanism, incidence, and missing string. Obstet Gynecol Surv. 1981;36:335–53. doi: 10.1097/00006254-198107000-00001. [DOI] [PubMed] [Google Scholar]
- 9.Timonen H, Kurppa K. IUD perforation leading to obstructive nephropathy necessitating nephrectomy: A rare complication. Adv Contracept. 1987;3:71–5. doi: 10.1007/BF01849255. [DOI] [PubMed] [Google Scholar]