

Abstract
Bochdalek hernias are usually congenital in nature and normally present after birth. However, in rare cases, these hernias are present in adulthood. We report an unusual case of a posttraumatic right-sided Bochdalek hernia found incidentally in an adult and treated successfully with conservative management.
Keywords: Adult, atypical, Bochdalek hernia, right-sided
Introduction
In 1848, Vincent Alexander Bochdalek first described a congenital hernia resulting from the developmental failure of the diaphragmatic posterolateral foramina to fuse properly.[1] This type of fusion failure creates a defect through which viscera may herniate, resulting in what is known as a Bochdalek hernia. This is in contrast to a Morgagni's hernia, which is an anteromedial diaphragmatic defect. Bochdalek hernias can be a result of trauma but is normally congenital in nature (with an incidence of approximately one in 2,200 to 12,500 live births).[2] It may manifest as severe respiratory distress at birth requiring emergent surgical intervention. These hernias are normally left sided (70–90% of cases), hypothesized to be as a result of the location of the liver in the right chest and/or the timing of the fusion of pleuroperitoneal folds during development.[3,4,5,6] A Bochdalek hernia in adulthood is an unusual finding with fewer than 100 cases reported in the literature, as of 2007. It is even more atypical for these hernias to be right sided.[6,7]
Patients with right-sided Bochdalek hernia have a clinical presentation that varies from being asymptomatic to serious complications secondary to mechanical effect that might include strangulation of the intestinal tract, abdominal obstruction, abdominal pain, and respiratory distress. In the majority of the cases, Bochdalek hernias are seen on chest X-ray as a lung-based opacity that might have an air fluid level. Contrast-enhanced computerized tomographies (CT) have typical findings of fat or a soft tissue contour on the upper surface of the diaphragm or dilated bowel above the hemidiaphragm.[8]
The management is surgical and aims to reduce the abdominal contents and repair the defect, the approach of the left-sided hernias is controversial. Thoracotomy might improve the ability to separate adhesions between the thoracic viscera and the hernia sac some surgeons prefer laparotomy because they believe this technique is superior in the recognition and management of malrotation. It is also considered a more favorable approach when dealing with visceral complications such as obstruction or strangulation.[6] Right-sided defects are managed by a thoracic or thoracoabdominal approach because of the location of the liver. The mobilization of the right lobe of the liver produces an adequate view for surgical intervention.
Case Report
A 57-year-old African-American male with a past medical history significant for hypertension, type II diabetes mellitus, bilateral total hip replacements, and multiple motor vehicle accidents presented with complaints of diffuse abdominal discomfort, nausea, and generalized malaise 6 h prior to admission. His abdominal discomfort was diffuse, of moderate intensity, nonprovoked, nonradiating, and associated with nausea without vomiting. He noticed increased frequency, thirst, and decreased appetite for the past few days with a blood sugar of 500 on the morning of admission. He denied any other further symptoms of fevers/chills, diarrhea, constipation, chest pain, or shortness of breath. Vital signs on admission were mostly within normal limits with only an elevated blood pressure of 168/100. Physical exam was significant for decreased breath sounds in the lower-right lobe with no dullness to percussion or associated wheezing, rales, or rhonchi. His abdomen was slightly tender, but nondistended with normal bowel sounds. A PA/Lateral chest X-ray revealed a fluid-filled structure in the hemothorax interpreted to be a loculated right hydro-pneumothorax [Figure 1]. However, a CT scan of the chest showed the presence of viscera on his right lung, which was found to be a Bochdalek hernia [Figure 2]. The management of the patient's hernia was conservative, given that he was asymptomatic and the risks of any intervention outweighed the benefits. Symptoms of abdominal discomfort and nausea resolved with the correction of his blood glucose and the patient was subsequently discharged.
Figure 1.
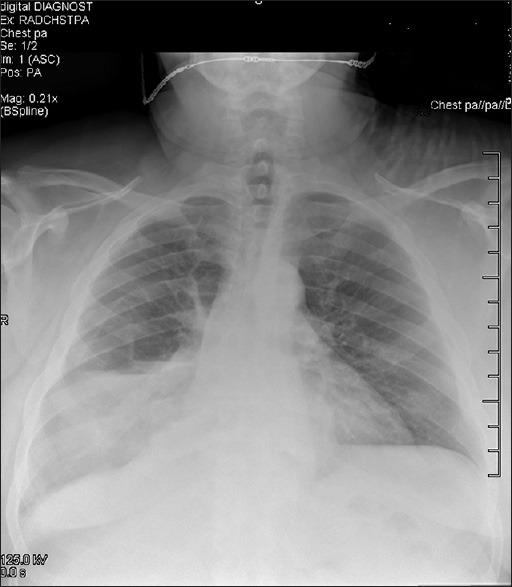
Chest X-ray PA/LT showing haziness of the right lower lobe and what appears to be an air/fluid level
Figure 2.
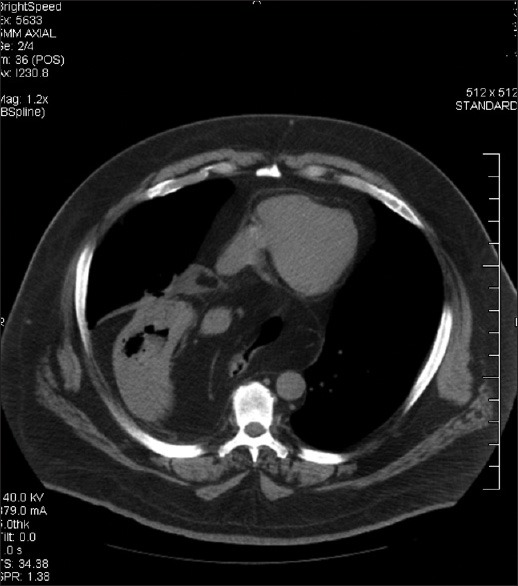
CT scan w/o contrast showing a herniated stomach with omental fat and colon on the right lung
Discussion
A Bochdalek hernia is normally thought of as a congenital anomaly occurring in approximately one in 2,200 to 12,500 live births[2] and is extremely rare in the adult population. Children with this type of hernia usually present with acute pulmonary symptoms. The incidence of asymptomatic Bochdalek hernias is unknown but is estimated to range from 1/2000 to 1/7,000. A study by Kocakusak et al. estimated an incidence of 0.17% to have an asymptomatic right-sided hernia.[1] Asymptomatic Bochdalek hernias are usually discovered unexpectedly on chest X-ray with confirmation via CT scan. On chest X-ray the hernia shows up as gas or fluid-filled structure. CT scan is normally the most useful imaging study for diagnosis with the typical findings of a fat or soft tissue contour on the upper surface of the diaphragm.[2] Another modality that can be utilized to help make the diagnosis, is an upper gastrointestinal contrast series, which can help exclude malrotation. The hernia found in our patient appeared to be large based on Gale's classification (on CT scans of 1-cm-thick sections, a large hernia will extend 5 cm or more). The majority of Bochdalek hernias is small and obtains only a modest amount of fat with a prevalence of 0.2% for large hernia's found in Gale's study.[5]
The patient described here presented with an asymptomatic Bochdalek hernia. Upon further questioning the patient admitted to a motorcycle accident approximately 10 years ago. This accident is a possible etiology to the formation of the hernia, likely secondary to trauma. However, the incidence of post-traumatic diaphragmatic hernia remains uncertain.[5,6,7] The majority of trauma induced injures are left-sided diaphragmatic ruptures as opposed to right sided, which was seen in the patient presented earlier. The right diaphragm appears to be partially protected by the liver, thereby decreasing the incidence of right-sided diaphragmatic ruptures[4] and adding to the rarity our case.
Conclusion
Bochdalek hernia presents at birth as a result of a congenital malformation in the majority of cases but can be rarely in adults. We present a case of an asymptomatic adult with a right-sided Bochdalek hernia incidentally found on CT scan. This case demonstrates the importance of further investigation in findings of gas and/or fluid-filled structures in the hemithorax, in order to rule out various etiologies other than a hydro-pneumothorax. A Bochdalek hernia should be included in the differential of such findings.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Kocakusak A, Arikan S, Senturk O, Ycel AF. Bochdalek's hernia in an adult with colon necrosis. Hernia. 2005;9:284–7. doi: 10.1007/s10029-004-0302-x. [DOI] [PubMed] [Google Scholar]
- 2.Laaksonen E, Silvasti S, Hakala T. Right-sided Bochdalek hernia in an adult: A case report. J Med Case Rep. 2009;3:9291. doi: 10.1186/1752-1947-3-9291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Patti M, Fisichella P. Esophagus and Diaphragm. Current Diagnosis and Treatment: Surgery 13e. (Chapter 20) [Google Scholar]
- 4.Reber PU, Schmied B, Seiler CA, Baer HU, Patel AG, Büchler MW. Missed diaphragmatic injuries and their long-term sequelae. J Trauma. 1998;44:183–8. doi: 10.1097/00005373-199801000-00026. [DOI] [PubMed] [Google Scholar]
- 5.Jeyarajah RD, Feldman HW., Jr . Chapter 24-Abdominal Hernias and Gastric Volvulus. 9th ed. Philadelphia, Pennsylvania, USA: Saunders, An Imprint of Elsevier; 2010. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. [Google Scholar]
- 6.Rout S, Foo FJ, Hayden JD, Guthrie A, Smith AM. Right-sided Bochdalek hernia obstructing in an adult: Case report and review of the literature. Hernia. 2007;11:359–62. doi: 10.1007/s10029-007-0188-5. [DOI] [PubMed] [Google Scholar]
- 7.Sener RN, Tugran C, Yorulmaz I, Dagdeviren A, Orguc S. Bilateral large Bochdalek hernia in an adult: CT demonstration. Clin Imaging. 1995;19:40–2. doi: 10.1016/0899-7071(94)00023-6. [DOI] [PubMed] [Google Scholar]
- 8.Zenda T, Kaizaki C, Mori Y, Miyamoto S, Horichi Y, Nakashima A. Adult right-sided Bochdalek hernia facilitated by coexistent hepatic hypoplasia. Abdom Imaging. 2000;25:394–6. doi: 10.1007/s002610000021. [DOI] [PubMed] [Google Scholar]