

A previously fit 52-year-old man presented with severe progressive exertional dyspnea. He was in heart-failure with an elevated jugular-venous-pressure, edema and increased plasma-NTpro-BNP levels of 4,285 ρg/mL (upper limit of normal <900ρg/mL). His ECG demonstrated sinus-rhythm with low limb and chest lead voltages (Figure 1). He had significant proteinuria with renal and bone-marrow biopsies confirming Light-chain (AL) amyloidosis. Cardiac-Magnetic-Resonance (CMR) imaging revealed concentric left-ventricular-hypertrophy with an ejection-fraction of 65%, left-ventricular-end-diastolic-volume (LVEDV)=146mL, left-ventricular-endsystolic-volume (LVESV)=51mL, left-ventricular-mass=245g, and left-atrial-volume=144mL (Figure 2, Movie 1). Late-gadolinium-enhanced (LGE) imaging showed extensive diffuse subendocardial hyperenhancement in both ventricles (Figures 3 and 4, arrows) consistent with amyloid infiltration. He subsequently underwent successful autologous-stem-cell transplantation.
Figure 1.
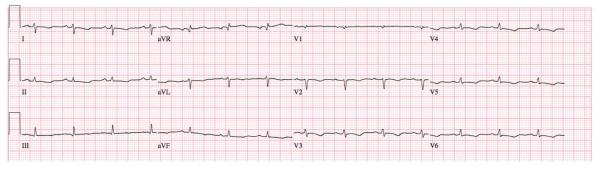
ECG showing sinus-rhythm with low QRS voltages (<5mm in the limb leads and <10mm in the chest leads).
Figure 2.

Cine imaging in the 4-chamber view, showing an ejection fraction of 65%, concentric left-ventricular hypertrophy, and an enlarged left atrium.
Figure 3.

Late Gadolinium Enhancement (LGE) imaging in the 4-chamber view, showing extensive diffuse subendocardial hyperenhancement involving both ventricles (arrows).
Figure 4.

Late Gadolinium Enhancement (LGE) imaging in the 3-chamber view, showing extensive diffuse subendocardial hyperenhancement (arrows).
At follow-up, 2.5 years later, his functional-status had markedly improved and he was exercising regularly. His cardiovascular examination and plasma-NTpro-BNP level (117ρg/mL) was normal. His ECG showed some recovery of voltages in the limb leads (Figure 5). Repeat CMR imaging showed minimal change in left-ventricular volumes, function and mass (LVEDV=138mL, LVESV=43mL, ejection fraction=69%, left-ventricular-mass=235g); although left-atrial volume was significantly reduced (105mL) (Figure 6, Movie 2). LGE imaging demonstrated marked regression of the subendocardial hyperenhacement (Figures 7 and 8).
Figure 5.
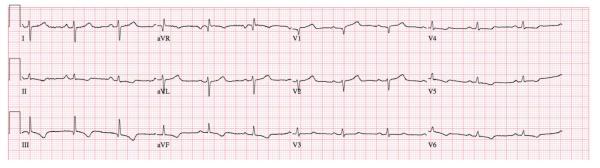
Post transplant ECG showing sinus-rhythm with some recovery of voltages in the limb leads (>5mm in leads I, III, aVR, aVL).
Figure 6.

Post stem cell transplant. Cine imaging in the 4-chamber view, showing an ejection fraction of 69% with concentric left-ventricular hypertrophy. The left atrium has reduced in size.
Figure 7.

Post stem cell transplant. Late Gadolinium Enhancement (LGE) imaging in the 4-chamber view, showing significant regression of the subendocardial hyperenhacement.
Figure 8.

Post stem cell transplant. Late Gadolinium Enhancement (LGE) imaging in the 3-chamber view, showing significant regression of the subendocardial hyperenhacement.
Prognosis for patients with AL-amyloid and cardiac-infiltration has historically been dismal and extensive cardiac-involvement has generally been regarded as a contraindication to stem-cell-transplantation1-3. This case suggests that stem-cell-transplantation can lead to regression of cardiac-amyloid and may be considered in selected patients.
Supplementary Material
Acknowledgments
Funding Sources: Dr Brahmanandam was supported by an NIH grant (T32HL072742).
Footnotes
Conflict of Interest Disclosures: None.
References
- 1.Banypersad SM, Moon JC, Whelan C, Hawkins PM, Wechalekar AD. J Am Heart Assoc. 2012;1:e000364. doi: 10.1161/JAHA.111.000364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Falk RH, Dubrey SW. Amyloid Heart Disease. Prog Card Dis. 2010;52:347–61. doi: 10.1016/j.pcad.2009.11.007. [DOI] [PubMed] [Google Scholar]
- 3.Falk RH. Diagnosis and Management of the Cardiac Amyloidoses. Circulation. 2005;112:2047–60. doi: 10.1161/CIRCULATIONAHA.104.489187. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.