

Abstract
We explored a new method for simple and accurate control of shoulder movement for externally powered shoulder disarticulation prostheses using a two-axis joystick. Ten subjects with intact shoulders and arms were tested to determine the average amount of shoulder motion and force available for control of an electronic input device. This information was then applied to two different input strategies in order to examine their effectiveness: (1) a traditional strategy implemented with a rocker potentiometer and a pair of force-sensing resistors (FSRs), and (2) a strategy implemented with a two-axis joystick. Three able-bodied subjects and two subjects with shoulder disarticulation amputations attempted to control an experimental powered shoulder using both control strategies. Two powered arms were tested, one with powered flexion/extension and humeral rotation, and one with powered flexion/extension and adduction/abduction. Overwhelmingly, the subjects preferred the joystick control, as it was more intuitively linked with their shoulder movement. Additionally, two motions (one in each axis) could be controlled simultaneously. This pilot study provides valuable insight into an effective means of controlling high-level, externally powered prostheses via a two-axis joystick.
Keywords: control strategies, externally powered prosthesis, force-sensing resistor, joystick, proprioception, proportional control, rocker potentiometer, shoulder disarticulation, shoulder excursion, upper-limb amputation
1 Introduction
Fitting functional prostheses to individuals with shoulder disarticulation or humeral neck amputations is a major challenge. Cable-driven prostheses require precise fitting and harnessing in order to capture the required excursion from the user. Over 10 cm of excursion is required to operate a prosthesis, including 5 cm to open the terminal device and over 6 cm to flex the elbow3. The most commonly used motions, scapular and biscapular protraction, typically generate less than 10 cm of excursion. The required excursion of the prosthesis may be reduced to accommodate the limited excursion of the user by movement of the elbow flexion attachment or the inclusion of an excursion amplifier. A decrease in the required excursion comes with the associated cost of an increase in the force required to operate the prosthesis; many users find this force difficult to generate. The limited return in function and unphysiological control are important factors in the high rejection rate of high-level prostheses [1].
In an attempt to allow users with a shoulder disarticulation to control a prosthesis with less effort, prosthetists may use externally powered components or combinations of body-powered and externally powered components (hybrid prostheses). The use of externally powered components decreases the necessary excursion and force required of the user and may provide increased joint range of motion and/or grip strength. Commercially available powered components include terminal devices, elbows, and electronic wrist rotators. With the exception of one body-powered design, humeral rotators are either fixed or use passive friction turntables. Likewise, all commercially available shoulder joints are passive or lockable after manual positioning.
Externally powered components may be controlled using a variety of sensors, both digital and analog. Digital sensors include momentary contact switches and pull switches, and will not be dealt with in this article. Analog (proportional) sensors include force-sensing resistors (FSRs), motion tracking sensors such as linear potentiometers or potentiometer-based joysticks, and electromyographic (EMG) sensors. Vodovnik and Rebersek [2] found that motion-tracking sensors provide the best control of a single degree of freedom (DOF), followed by pressure sensors (such as FSRs), with EMG sensors ranking last. At the transradial level, EMG sensors have the advantage of providing intuitive control of the wrist and hand, but at the shoulder level, all sensors are equally unintuitive in controlling the hand, wrist, or elbow. Doubler and Childress [3, 4] have found that movement control (e.g. residual shoulder movement) provides good simultaneous control of 2 DOFs, but have not compared their results to FSR or myoelectric control.
Subjects with externally powered shoulder disarticulation prostheses need to control multiple motors, and would benefit substantially from control sources that allow precise, simultaneous control. Towards this end, we have turned our attention to clinically appropriate ways of using the residual shoulder as a control source. Specifically, we have looked at the conventional method of combining FSRs with a rocker potentiometer, and the promising option of capturing shoulder motion using a two-axis joystick. Use of residual shoulder motion to control prosthetic components has been proposed for several decades. Several studies have used shoulder control on able-bodied subjects [3–5] or on subjects with an amputation controlling a remote prosthesis [6], and a few studies have looked at combined ipsilateral/contralateral shoulder control of an integrated prosthesis [7–10]. This paper looked specifically at ipsilateral shoulder control sensors for use in a clinical setting, as well as the interfaces connecting the sensors to the subject.
2 Methods
All tests were performed with written, informed consent and Institutional Review Board (IRB) approval.
Maximum Shoulder Force & Excursion
An initial investigation looked at typical shoulder excursion (linear displacement) and force in able-bodied subjects. Two series of tests were performed on five men and five women. The first test involved utilizing an oversized transparent socket with a telescoping rod/sheave apparatus that could be mounted superiorly, anteriorly, or posteriorly. The subjects were required to relax as the rod was positioned in contact with their shoulder (one position at a time in each of the three locations). The subjects were then asked to move their shoulder complex through four different motions: elevation, depression, protraction, and retraction. Displacements during these four motions were measured as the change in translation of the telescoping rod at three locations (the superior position was used to measure both elevation and depression). Five trials were performed for each motion. Pressure measurements were also recorded from the same subjects, utilizing a 0.786 cm2 point of contact. Data were only collected for three motions, as depression of the shoulder would pull away from the pressure gauge. Pressure data were then converted to force in Newtons.
Shoulder-Control Techniques
Three able-bodied subjects and two subjects with shoulder disarticulation amputations participated in the subsequent study. A certified prosthetist1 made custom bypass sockets for each able-bodied subject, consisting of clear thermoplastic sockets with an opening for their sound arm to exit. A large four-spoke mounting plate attached to the socket created a pass-through for the sound arm and permitted mounting of the prosthetic arm. Subjects with shoulder disarticulation amputations were fit with conventional perimeter-frame-style sockets for mounting control inputs and electronic hardware. Subjects controlled a powered shoulder flexor and a powered humeral rotator. One subject with a shoulder disarticulation amputation also used the joystick strategy to control shoulder adduction/abduction and shoulder flexion/extension Both shoulder disarticulation patients had undergone targeted muscle reinnervation surgery [11, 12], and used muscles in their chest to control elbow and hand movements simultaneously with shoulder movements. While the powered shoulder components used in this study are not commercially available, this control illustrates the potential control of commercially available devices such as elbows, wrists, and terminal devices.
Custom software, developed by the University of New Brunswick, was used to provide real-time control of the prosthesis. Proportional (velocity) control was used as the control paradigm. Proportional control increases the speed of the motion as the magnitude of the command signal increases. It is the control paradigm used by Otto Bock, Motion Control, and Liberating Technologies. Gains were individually tuned by a certified prosthetist for each sensor system. Two strategies for controlling two DOFs were tested: one using a traditional FSR/rocker potentiometer setup and the other using a two-axis joystick.
FSR/Rocker Potentiometer Control
The FSR and rocker potentiometer setup allowed for sequential control of humeral rotation and shoulder flexion/extension. For control of humeral rotation, two FSRs were placed on the lateral portion of the socket (Figure 1). One FSR was mounted anteriorly for operation of internal rotation and one FSR was mounted posteriorly for operation of external rotation. The velocity of humeral rotation was proportional to the force applied to the FSRs. This control strategy had the potential to provide the subjects with cutaneous force feedback when pressing on the FSRs. For control of shoulder flexion/extension, a proportional rocker potentiometer was mounted above the shoulder on the superior aspect of the socket (Figure 1). This electromechanical component is a single-axis, center-zero rocking potentiometer2. The benefit of this device is that it can provide a proportional output, while traditional rocker “switches” used in externally powered prostheses only allow a single output level. The velocity of shoulder flexion/extension was proportional to the position of the rocker potentiometer.
Figure 1.

Sagittal view of FSRs and a rocker potentiometer in a shoulder disarticulation prosthesis.
Joystick Control
A design with a two-axis joystick was used to provide control of two DOFs while enabling simple fabrication and calibration. The joystick consisted of two potentiometers aligned in orthogonal directions to measure shoulder displacements in two dimensions. Utilization of joysticks to control a powered hand, wrist, and elbow were described by Davalli and Sacchetti [13], although the linkage to the body was unclear. In this study, the joystick was used to provide input to motors that controlled anatomical shoulder movements. At first, the joystick was mounted medially on the socket, on the distal portion of the shoulder segment (Figure 2). A shoulder cap was modified with an eyelet mounted superiorly to accept the extended rod of the joystick and was attached to the socket with three elastic-webbing straps. The design of the eyelet permitted the rod to slide and therefore prevented binding and inadvertent signals. Shoulder movements were tracked by the shoulder cap and resulted in corresponding movements of the rod via the eyelet. When used without the shoulder cap, the distal end of the rod was fed through a cylindrical sleeve. In one version of this design, the sleeve was bonded to a snap that attached it to a tight-fitting shirt (Figure 3, video available in online feature). In the other version, the sleeve was bonded to a thin elastic strap secured to the socket (Figure 4, video available in online feature). Both of these designs used a hollow sheave, similar in size to a portion of a straw, in order to minimize the profile of the eyelet. A custom low-profile two-axis joystick was used with the spandex shirt, and a commercially available miniature two-axis joystick3 was used with the elastic strap.
Figure 2.

(a) Diagram of setup for capturing shoulder movement using a 2-axis joystick and a shoulder cap. (b) Close-up of joystick and shoulder cap attached to a prosthetic socket.
Figure 3.

Custom low-profile two-axis joystick with distal end of sheave affixed to a spandex shirt.
Figure 4.
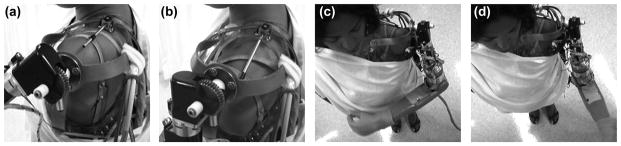
Commercially available miniature two-axis joystick with distal end connected to an elastic strap to capture shoulder movement and control a powered shoulder and humeral rotator. (a) Shoulder elevation produces shoulder flexion. (b) Shoulder depression produces shoulder extension. (c) Shoulder protraction produces internal humeral rotation. (d) Shoulder retraction produces external humeral rotation.
All five subjects tested a system in which shoulder elevation/depression controlled shoulder flexion/extension, and shoulder protraction/retraction controlled internal/external humeral rotation. One subject also tested a system in which internal/external humeral rotation were replaced by shoulder abduction/adduction.
3 Results
Maximum Shoulder Force & Excursion
The maximum displacements and forces generated in the scapulothoracic joints of 10 able-bodied subjects are displayed in Table 1. Significant differences were present between measured maximum displacements in elevation and depression, with substantial differences also present between maximum displacements in protraction and retraction. There were no significant differences between maximum forces generated via shoulder protraction, retraction, or elevation; or between male and female subjects for either excursion or force measurements.
Shoulder-Control Techniques
Both able-bodied subjects and subjects with a shoulder disarticulation were able to use the FSR/rocker potentiometer strategy, but had difficulty locating the appropriate sensor without occasionally hitting a different sensor. While they were all able to locate the sensors, the added delay of cautiously hunting for the appropriate sensor substantially inhibited their ability to control the prosthetic device. Although the subjects were able to feel the sensors, they could not appreciate significant cutaneous feedback from pressing on them.
For able-bodied subjects, control using the two-axis joystick worked much better than the FSR/rocker potentiometer strategy. Shoulder movements and humeral rotations were noticeably smoother and more fluid. There were also fewer pauses in operation, as the subjects were not required to search for the appropriate sensor; subjects reported that this made the control faster. They also reported that control with this strategy was easier and more intuitive, and that it seemed more accurate.
4 Discussion
Both strategies examined in this study were clinically viable for subjects with a shoulder disarticulation. Control with a joystick had clear advantages over control with the FSRs and rocker potentiometer: it provided fast, accurate, and intuitive control in a large workspace without the need to hunt for the sensors. It also provided simultaneous control of two DOFs.
The results of this study were somewhat surprising in that we expected the FSRs and rocker potentiometer to be easier for the subjects to find and to provide the subjects with important cutaneous feedback that improved control. However, the joystick control system was clearly preferred by all of our subjects, both able-bodied and amputees. The difference in performance of the two systems could be due to the type and amount of feedback they provided to the patients. The joystick system provided the subjects with continuous control and proprioceptive feedback throughout their entire workspace, whereas the FSRs and rocker potentiometer only operated when touched (i.e. in a very small work space). The FSRs and rocker potentiometer clearly provided some cutaneous feedback when touched, while the joystick provided no cutaneous feedback as there was no resistance in the system. Thus, the superior proprioceptive feedback of the joystick appeared to offer more of a benefit than the limited cutaneous and proprioceptive feedback of the FSR and rocker potentiometer system.
A spandex shirt or elastic strap provided substantially better joystick control than a shoulder cap in subjects with an amputation. Initially, joystick control did not work optimally for these subjects. The limited range of shoulder motion, coupled with the tendency of the shoulder cap to become displaced, prevented the subjects from having accurate control of the prosthesis. Custom shoulder caps did not capture shoulder movement with sufficient precision, as the elastic webbing held the cap in place too firmly, causing the shoulder to slip out of the cap if it moved too far. This effect was amplified when the subjects’ movements were limited by joint restrictions. Spandex shirts and elastic straps were able to provide better control because they more accurately captured the motion of the shoulder, which is an essential element in any motion capture device.
Commercially available control software commonly uses proportional velocity control, and many research studies set the position, rather than the speed, of the prosthesis proportional to FSR strength or joint movement. Such a control paradigm is termed proportional position control or servo control. Previous studies have shown that proportional position control provides better control of the prosthetic joints than proportional velocity control when shoulder motion is used as the input signal [3, 4]. Due to software limitations, this study was only able to test proportional velocity control. The implications for sensor design still apply, however, and the use of proportional position control should only further highlight the benefits of using a two-axis joystick in clinical applications.
Several practical considerations contributed to the success of the two-axis joystick design. We initially placed the joystick on the medial side of the eyelet or sheath. In later designs, we moved the joystick to the lateral aspect of the socket. Lateral placement had two benefits: It shortened the length of the rod between the joystick and the sheath, which in turn amplified the rotational movement of the joystick. This amplification provided a greater range of joystick motion to be used, resulting in better control of the prosthesis. In addition, lateral placement allowed for integration of the joystick with the shoulder joint cosmesis, keeping an unobtrusive socket outline in the medial aspect where it is more noticeable in collarless shirts.
One potential drawback of the joystick design was that it required a two-part socket, superior cut-out, elastic strap, or spandex shirt. The need to provide two separate elements and have them joined by the joystick rod not only introduces some complexity to fabrication, but may be difficult for a shoulder disarticulation amputee to don and doff. In addition, parts and circuitry for the two-axis joystick are not currently commercially available for implementation on prosthetic devices.
Both of the subjects with shoulder disarticulations tested in this study had undergone targeted muscle reinnervation (TMR) [11, 12] and thus had independent myoelectric control of elbow flexion/extension and terminal device open/close. The shoulder controller was added in order to provide inputs for externally powered shoulders and humeral rotators. These subjects both voiced the opinion that shoulder control using the joystick provided higher fidelity control than their EMG sites. This being said, these subjects would opt to use both EMG and joystick control together to increase the number of simultaneously controlled prosthetic components, while they continue to prefer their targeted reinnervation EMG sites to control the elbow and hand, due to the intuitive, physiologically appropriate portal they provide. Subjects who have not undergone TMR could still benefit from shoulder control using a two-axis joystick to control more distal joints such as terminal devices, wrists, and elbows.
These TMR subjects used both EMG sensors and a motion-capture sensor. The FSR/rocker potentiometer paradigm did not work as well in parallel with TMR EMG. When using a shoulder cap rigidly affixed to the main socket and FSR sensors, pressure applied against the socket to activate the FSRs frequently caused the EMG sensors to lose contact with the skin. A free-floating two-axis joystick allowed for simultaneous control of the EMG sensors and the joystick, since shoulder movement did not come in contact with the socket and push away the EMG electrodes. This observation is generally not applicable to non-TMR amputees because most patients are unlikely to use both EMG sensors and a motion capture sensor.
5 Conclusion
A two-axis joystick may be implemented by prosthetists using commercially available components. The design takes less time to fabricate than proper placement of FSRs and rocker potentiometer, which require iterative adjustment to allow proper operation. As a result, prosthetists should consider using a joystick to improve control for subjects with a shoulder disarticulation. Assurance must be made that shoulder motion does not cause the entire socket to move, and close attention should be paid to providing minimal resistance to shoulder movement. This can be accomplished using a free-floating interface such as an elastic strap coupled to a freely moving potentiometer.
Table I.
Maximum Shoulder Displacements and Forces
| Displacement (cm) | Force (N) | |||
|---|---|---|---|---|
| Movement | Avg. | SD | Avg. | SD |
| Protraction | 3.7 | 1.3 | 21.5 | 6.2 |
| Retraction | 2.8 | 0.9 | 25.2 | 5.9 |
| Elevation | 4.2 | 1.1 | 25.7 | 6.2 |
| Depression | 2.2 | 0.8 | ||
Acknowledgments
Funding Sources: DEKA Research and Development Corporation, Contract No. W911NF-06-C-0001; Johns Hopkins University Applied Physics Laboratory, Contract No. 908090; NIH/NICHD, Contract No. R01 HD044798-01; NIH/NICHD, Contract No. HHSN275200503402C/N01-HD-5-3402
The authors thank Joseph E. Barton, PhD for his participation in the planning and data collection phases of the preliminary shoulder excursion and force experiments. This work was supported by National Institutes of Health Grant N01-HD-5-3402.
Abbreviations
- FSR
Force-sensing resistor
- DOF
degree of freedom
- EMG
electromyographic
- TMR
targeted muscle reinnervation
Footnotes
American Board for Certification in Orthotics, Prosthetics & Pedorthics
J3R Rocker Potentiometer, ETI Systems, Carlsbad, California
CTS 252, CTS Corporation, Elkhart, Indiana
Note: No clinical trial registration is required
References
- 1.Biddiss EA, Chau TT. Upper limb prosthesis use and abandonment: A survey of the last 25 years. Prosthet Orthot Int. 2007;31(3):236–57. doi: 10.1080/03093640600994581. [DOI] [PubMed] [Google Scholar]
- 2.Vodovnik L, Rebersek S. Information-content of myo-control signals for orthotic and prosthetic systems. Archives of Physical Medicine and Rehabilitation. 1974;55(2):52–6. [PubMed] [Google Scholar]
- 3.Doubler J, Childress DS. Design and evaluation of a prosthesis control system based on the concept of extended physiological proprioception. Journal of Rehabilitation Restorative Devices. 1984;21(1):19–31. [PubMed] [Google Scholar]
- 4.Doubler J, Childress DS. An analysis of extended physiological proprioception as a prosthesis-control technique. Journal of Rehabilitation Restorative Devices. 1984;21(1):5–18. [PubMed] [Google Scholar]
- 5.Durfee WK, Mariano TR, Zahradnik JL. Simulator for evaluating shoulder motion as a command source for fes grasp restoration systems. Archives of Physical Medicine and Rehabilitation. 1991;72(13):1088–94. [PubMed] [Google Scholar]
- 6.Kyberd PJ, Poulton A, Sandsjo L, Jonsson S, Jones B, Gow D. The tompaw modular prosthesis: A platform for research in upper-limb prosthetics. Journal of Prosthetics and Orthotics. 2007;19(1):15–21. [Google Scholar]
- 7.Simpson DC. Externally powered prosthesis for complete arm replacement. Physics in Medicine and Biology. 1972;17(1):110. [Google Scholar]
- 8.Simpson DC, Kenworth G. Design of a complete arm prosthesis. Biomedical Engineering. 1973;8(2):56–9. [PubMed] [Google Scholar]
- 9.Simpson DC, Smith JG. Externally powered controlled complete arm prosthesis. Journal of Medical Engineering & Technology. 1977;1(5):275–7. doi: 10.3109/03091907709162194. [DOI] [PubMed] [Google Scholar]
- 10.Simpson DC. The choice of control system for the multimovement prosthesis: Extended physiological proprioception (e.P.P) In: Herberts P, Kadefors R, Magnusson R, Petersen I, editors. The control of upper-extremity prostheses and orthoses. Springfield, IL: Charles Thomas; 1974. pp. 146–50. [Google Scholar]
- 11.Kuiken TA, Miller LA, Lipschutz RD, Lock BA, Stubblefield K, Marasco PD, et al. Targeted reinnervation for enhanced prosthetic arm function in a woman with a proximal amputation: A case study. Lancet. 2007;369(9559):371–80. doi: 10.1016/S0140-6736(07)60193-7. [DOI] [PubMed] [Google Scholar]
- 12.Kuiken TA, Dumanian GA, Lipschutz RD, Miller LA, Stubblefield KA. The use of targeted muscle reinnervation for improved myoelectric prosthesis control in a bilateral shoulder disarticulation amputee. Prosthetics and Orthotics International. 2004;28(3):245–53. doi: 10.3109/03093640409167756. [DOI] [PubMed] [Google Scholar]
- 13.Davalli A, Sacchetti R, editors. Mini joystick for upper limbs prostheses. MyoElectric Controls Symposium; 2002; New Brunswick, Fredericton. [Google Scholar]