

Abstract
Plasmacytomas are monoclonal plasma cells proliferations originating either in localized osseous tissue or in soft tissue (extramedullary plasmacytoma, EMP). Although many such lesions are found in the bone marrow, fewer arise in extramedullary tissue. A solitary EMP involving the adrenal gland is extremely rare, with only 7 cases having been reported in the literature thus far. Here, we describe a rare case of solitary EMP in the right adrenal gland of a 26-year-old man that was managed by retroperitoneal laparoscopic resection, with no recurrence during 6-year follow-up.
Keywords: Extramedullary plasmacytoma, adrenal, pathology
Introduction
Extramedullary plasmacytoma (EMP), a rare disorder characterized by a malignant plasma cell neoplasm, accounts for approximately 3% of all plasma cell malignancies [1]. Typically, 80% of EMP lesions are found in the head and neck region, particularly in the upper respiratory tract [2]. Adrenal EMP is a rare clinical entity, and a literature search by a professional librarian using MEDLINE and EMBASE from January 1996 to September 2014 revealed that reports of such lesions are extremely rare, with only 7 cases reported thus far [3-9]. Among the reported cases, the patients’ ages ranged from 47 to 77 years. Further, the treatment protocols varied, with 5 patients treated by adrenalectomy with or without radiotherapy and chemotherapy; and 1, by chemotherapy and autologous hematopoietic stem cell transplantation. The longest recorded follow-up among these cases was 47 months (Table 1). Here, we describe an additional case of solitary EMP in the adrenal gland in a young patient and discuss its clinical features, diagnosis, and treatment.
Table 1.
Characteristics of patients with adrenal extramedullary plasmacytoma
| Study | Years | Country | Age | Gender | Side | Tumor size (cm) | Function | Treatment | Follow-up (month) |
|---|---|---|---|---|---|---|---|---|---|
| Kahara, [3] | 2001 | Japan | 52 | Male | Right | 4 | No | LCA | 12 |
| Asahi, [4] | 2001 | Japan | 52 | Male | Right | 4 | No | LC A + C + R | NP |
| Fujikata, [5] | 2002 | Japan | 77 | Male | Right | 10 | Yes | OA + nephrectomy + R | 12 |
| Rogers, [6] | 2004 | American | 75 | Female | Right | 3.5 | No | LCA + R | NP |
| Li, [7] | 2007 | China | 64 | Female | Bilateral | 6 right/4 left | No | OA | NP |
| Ahmed, [8] | 2009 | Saudi Arabia | 47 | Male | Bilateral | 8 right/8 left | No | C + autologous hematopoietic stem cell transplantation | 47 |
| Antona, [9] | 2011 | Spain | 76 | Female | Left | 6 | No | Adrenalectomy + R | 40 |
LCA = laparoscopic adrenalectomy; C = chemotherapy; R= radiotherapy; OA = open adrenalectomy; NP = no report.
Case report
A 26-year-old man presented with a 1-month history of intermittent right flank pain. The patient had previously been in good health, and there was no relevant medical or family history. The findings of physical examination were unremarkable. Ultrasonography revealed a hypoechoic mass in the right adrenal gland area. Abdominal contrast-enhanced computerized tomography (CT) revealed a rounded, soft tissue density shadow (measuring 28 × 31 × 45 mm) without enhancement in the right adrenal gland area (Figure 1). The findings of routine blood tests, blood biochemical examination, and routine urinalysis tests were also normal. There was no indication of hormonally abnormalities in an endocrinologic survey that included determination of urinary metanephrine, normetanephrine and serumal aldosterone, hydrocortisone, angiotensin, rennin. Eventually, a clinical diagnosis of a nonfunctioning adrenal tumor was considered.
Figure 1.
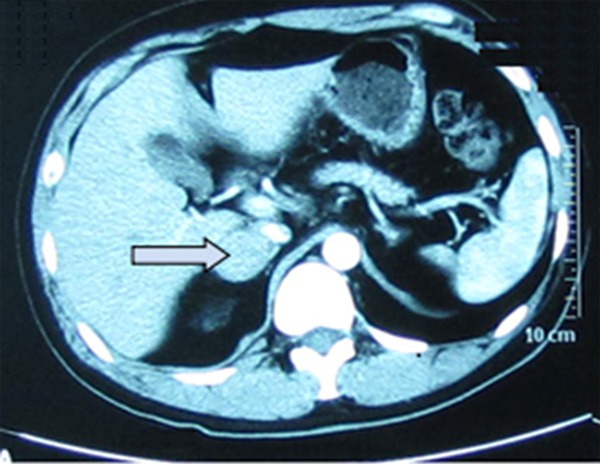
Contrast enhanced computerized tomography (CT) scan revealed an rounded, soft tissue density shadows (28 × 31 × 45 mm) without enhancing in the right adrenal gland (arrow).
Subsequently, the patient underwent retroperitoneal laparoscopic adrenalectomy, with no complications. On gross examination, the mass measured 3.4 cm in diameter; it was well circumscribed, with a black and yellow rugged surface with no evidence of necrosis or hemorrhage. However, the findings of the postoperative histopathological examination of the resected specimen suggested a plasmacytoma confined to the adrenal gland. Microscopy showed that the mass was composed of clusters of typical plasmacytoma cells with a spoke-wheel-like nucleus and eccentric nuclei (Figure 2A). Occasional bi- and multi-nucleation and 1-2 mitotic figures in the nuclei were observed in high-power field microscopy (Figure 2B). Immunohistochemical staining revealed the positive for CD45 and kappa light chain expression.
Figure 2.
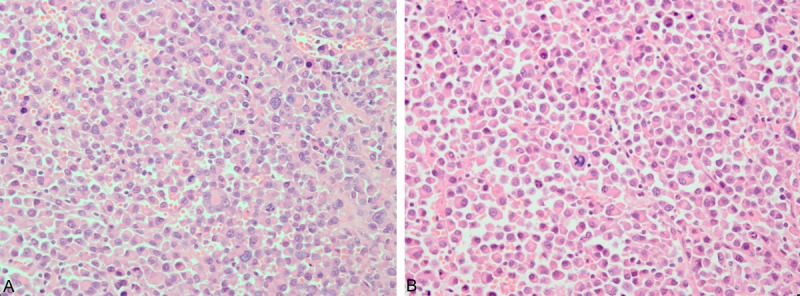
A. Microscopy showed that the mass was composed of atypical plasmacytoma cells with wheel-spoke-like nucleus, clusters of plasma cells with eccentric nuclei (Hematoxylin-eosin staining; original magnification, 400×). B. Occaslonal bi- and multi-nucleation and 1-2 mitotic figures in the nuclei were observed in high-power field microscopy (Hematoxylin-eosin staining; original magnification, 400×).
To confirm the diagnosis of EMP, further postoperative investigations were performed. Serum immunoglobulin (Ig) G levels were increased to 24.8 g/L (normal range, 8.0-15.5 g/L), while serum IgM and IgA levels were within the normal ranges. No Bence-Jones proteins were detected by urine electrophoresis or urine immunofixation. A skeletal survey showed no lesions. Bone marrow aspiration and biopsy showed no evidence of plasmacytic infiltration. Eventually, a diagnosis of solitary EMP was established. The patient’s postoperative recovery was uneventful. A follow-up skeletal survey at 6 years showed normal findings, and the patient remained alive and well.
Discussion
EMP is defined as an extraosseous proliferation of neoplastic plasma cells. Solitary EMP occurs in a male:female ratio of 3:1, and is typically found in patients aged 50-60 years, with a median age of 55 years [10]. However, a solitary EMP involving the adrenal gland is extremely uncommon. To the best of our knowledge, only 7 cases of adrenal EMP have been reported in the literature to date. All of these reports involved patients aged over 47 years. However, in the present case, the patient was considerably younger than the reported median patient age for adrenal EMP, and was only 26 years old at the time of presentation. Therefore, he is the youngest patient to have been diagnosed with an EMP arising from the adrenal gland.
While the exact pathogenesis of EMP remains unclear, trauma may act as the triggering stimulus for plasma cells to proliferate, eventually leading to clonal infiltration [11]. Although solitary EMP can involve any extraosseous organs, up to 80% of such lesions are found in the head and neck areas [2]. The next most common site is the gastrointestinal tract [10]. Less frequent sites of EMP include the central nervous system, breast, skin, spleen, liver, testes, and the thyroid or the lymph nodes [12-16].
Plasma cell neoplasia or EMP is rarely observed in the adrenal gland, and these lesions have no characteristic clinical manifestations. Patients with adrenal EMP can present with back pain [5,7], abdominal pain [6,9], or remain asymptomatic [3,8]. In the present case, the patient presented with intermittent right flank pain and no other symptoms.
Preoperative laboratory examination and image examination does not contribute to the differential diagnosis of adrenal EMP from other tumors, since no specific imaging characteristics are present; however, fine-needle aspiration and pathological examination of tissue biopsy can indicate a diagnosis for this uncommon neoplasm. Ahmed et al. [8] reported the single known case of adrenal EMP with a preoperative diagnosis based on fine needle aspiration biopsy of the adrenal mass. In our case as well as in the remaining 6 previously reported cases, adrenal EMP was definitively diagnosed based on the histopathological examination of the resected specimens. In addition, the diagnosis of solitary EMP can be confirmed after excluding systemic disease by serum and urine protein electrophoresis, immunoelectrophoresis, skeletal imaging survey, and bone marrow biopsy. Our patient was considered to have a solitary adrenal EMP without any evidence of myeloma elsewhere, including no monoclonal proteins in serum and urine tests.
Although there are currently no clear treatment guidelines for solitary EMP, most patients with these lesions have been treated with radiotherapy, surgical excision, or combined radiotherapy and surgery [17,18]. Additionally, the use of chemotherapy has been reported for the treatment of EMP in the literature [19]. In localized cases, the tumor mass can be completed removed by surgical excision, which may be a better choice [11,20]. Fujikata et al. [5] have reported no tumor recurrence after a year of follow-up following combined surgical excision and radiotherapy. Li et al. [7] reported a case of bilateral adrenal EMP, wherein both tumor masses were simultaneously removed via laparotomy. In 3 other cases reported by Kahara et al. [3], Rogers et al. [6], and Asahi et al. [4], treatments included laparoscopic adrenalectomy (LCA) alone; combined LCA and radiotherapy; and combined LCA, radiotherapy, and chemotherapy, respectively. In the report by Ahmed et al. [8], bilateral adrenal EMP was treated by chemotherapy and autologous hematopoietic stem cell transplantation, with no recurrence until 47 months of follow-up. Antona et al. [9] treated a case of adrenal EMP with adrenalectomy and radiotherapy, with no evidence of recurrence until 40 months of follow-up. In our patient, we successfully performed retroperitoneal laparoscopic removal of the adrenal EMP, and the patient experienced uneventful recovery and stable rehabilitation. However, the patient refused to undergo postoperative radiotherapy or chemotherapy; fortunately, he has not experienced a recurrence for 6 years of follow-up at the time of writing.
In summary, we have described the 8th documented case of adrenal EMP in a 26-year-old patient, with the longest follow-up reported thus far. This confirmed that this rare type of adrenal EMP can occur in young patients. In addition, we consider retroperitoneal laparoscopic adrenalectomy to be the preferred treatment option since this approach provides magnified images that facilitate the complete removal of the tumor much easier. Although very rare, solitary EMP should be considered in the differential diagnosis of an adrenal mass.
Acknowledgements
This work was supported by the National Natural Science Foundation of China (Grant No. 81200551 and 81270841).
Disclosure of conflict of interest
None.
References
- 1.Hazarika P, Balakrishnan R, Singh R, Pujary K, Aziz B. Solitary extramedullary plasmacytoma of the sinonasal region. Indian J Otolaryngol Head Neck Surg. 2011;63:S33–S35. doi: 10.1007/s12070-011-0181-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Husarić S, Pašić J, Alić E, Kuljanin M. Solitary extramedullary plasmocytoma of the liver. Acta Medica Academica. 2013;42:85–6. doi: 10.5644/ama2006-124.76. [DOI] [PubMed] [Google Scholar]
- 3.Kahara T, Nagai Y, Yamashita H, Nohara E, Kobayashi K, Takamura T. Extramedullary plasmacytoma in the adrenal incidentaloma. Clin Endocrinol (Oxf) 2001;55:267–270. doi: 10.1046/j.1365-2265.2001.01191.x. [DOI] [PubMed] [Google Scholar]
- 4.Asahi H, Iwasa Y, Komatsu K, Hirata A, Koshida K, Namiki M. A case of plasmacytoma involving adrenal gland. Hinyokika Kiyo. 2001;47:629–631. [PubMed] [Google Scholar]
- 5.Fujikata S, Tanji N, Aoki K, Ohoka H, Hojo N, Yokoyama M. Extramedullary plasmacytoma arising from an adrenal gland. Urology. 2002;60:514v–514viii. doi: 10.1016/s0090-4295(02)01833-2. [DOI] [PubMed] [Google Scholar]
- 6.Rogers CG, Pinto PA, Weir EG. Extraosseous (extramedullary) plasmacytoma of the adrenal gland. Arch Pathol Lab Med. 2004;128:e86–e88. doi: 10.5858/2004-128-e86-EEPOTA. [DOI] [PubMed] [Google Scholar]
- 7.Li Y, Guo YK, Yang ZG, Ma ES, Min PQ. Extramedullary plasmacytoma involving the bilateral adrenal gland on MRI imaging. Korean J Radiol. 2007;8:246–248. doi: 10.3348/kjr.2007.8.3.246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ahmed M, Al-ghamdi A, Al-omari M, Aljurf M, Al-kadhi Y. Autologous bone marrow transplanation for extramedullary plasmacytoma presenting as adrenal incidentaloma. Ann Saudi Med. 2009;29:219–222. doi: 10.4103/0256-4947.51785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Blanco AF, Bahamonde CS, Blanco AL, Marín Pérez-Tabernero A. Adrenal extramedullary plasmacytoma. Cir Esp. 2011;89:690–691. doi: 10.1016/j.ciresp.2010.06.013. [DOI] [PubMed] [Google Scholar]
- 10.Soutar R, Lucraft H, Jackson G, Reece A, Bird J, Low E, Samson D. Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma. Clin Oncol. 2004;16:405–413. doi: 10.1016/j.clon.2004.02.007. [DOI] [PubMed] [Google Scholar]
- 11.Pasch W, Zhao XH, Pezk SA. Solitary plasmacytoma of the bone involving young individuals, is there a role for preceding trauma? Int J Clin Exp Pathol. 2012;5:463–7. [PMC free article] [PubMed] [Google Scholar]
- 12.Wu W, Pasch W, Zhao X, Rezk SA. Extraosseous plasmacytoma with an aggressive course occurring solely in the CNS. Neuropathology. 2013;33:320–333. doi: 10.1111/j.1440-1789.2012.01352.x. [DOI] [PubMed] [Google Scholar]
- 13.Neuhaus T, Hess T. Bilateral extramedullary plasmacytoma of the breast. Breast J. 2014;20:315–318. doi: 10.1111/tbj.12266. [DOI] [PubMed] [Google Scholar]
- 14.Bangerter M, Hildebrand A, Waidmann O, Griesshammer M. Fine needle aspiration cytology in extramedullary plasmacytoma. Acta Cytol. 2000;44:287–191. doi: 10.1159/000328466. [DOI] [PubMed] [Google Scholar]
- 15.Berrondo C, Gorman TE, Yap RL. Primary plasmacytoma of the testicle: a case report. J Med Case Rep. 2011;5:494–496. doi: 10.1186/1752-1947-5-494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bhat V, Shariff S, Reddy RA. Extramedullary plasmacytoma of thyroid- a mimicker of medullary carcinoma at fine needle aspiration cytology: a case report. J Cytol. 2014;31:53–56. doi: 10.4103/0970-9371.130710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Alexiou C, Kau RJ, Dietzfelbinger H, Kremer M, Spiess JC, Schratzenstaller B, Arnold W. Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts. Cancer. 1999;85:2305–2314. [PubMed] [Google Scholar]
- 18.Schmaus MC, Neuhof D. Radiotherapy for solitary plasmacytoma and multiple myeloma. Radiologe. 2014;54:551–555. doi: 10.1007/s00117-013-2630-2. [DOI] [PubMed] [Google Scholar]
- 19.Hazarika P, Balakrishnan R, Singh R, Pujary K, Aziz B. Solitary extramedullary plasmacytoma of the sinonasal region. Indian J Otolaryngol Head Neck Surg. 2011;63:33–35. doi: 10.1007/s12070-011-0181-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bhattacharya AK, Han K, Baredes S. Extramedullary plasmacytoma of the head and neck associated with the human immunodeficiency virus. Ear Nose Throat J. 1998;77:61–62. [PubMed] [Google Scholar]