

Abstract
Follicular dentritic cell sarcoma (FDCS) is an extremely rare malignant neoplasm arising from the accessory cells of the lymph nodes, the follicular dendritic cells. They commonly occur in the lymph nodes, but have also been reported at extranodal sites. Because of its rarity, FDCS is not easily to make a diagnosis by clinicians or pathologists. Herein, we report a soft palate tumor in a 59-year-old female, with a history of tonsillectomy. Pharynx MRI scan revealed a 4.7×3.0×3.5 cm mass at the right side of the parapharyngeal space. The pathology results returned as Follicular dentritic cell sarcoma. The patient underwent a tumorectomy and adjuvant postoperative radiotherapy. The patient was free of disease 1 year after the end of the treatment. The FDCS is an infrequent nonlymphoid malignant tumor accounting for less than 1% of all head and neck tumors. The immunohistochemical technique is essential for accurately identifying this class of tumour.
Keywords: Follicular dentritic cell sarcoma, softpalate, immunohistochemistry, CD21, CD23
Introduction
Follicular dendritic cell sarcoma (FDCS) is an uncommon tumor comprised within the spectrum of histiocytic and dendritic cell neoplasms. Besides being rare, these tumors are notoriously difficult to diagnose. Although most FDCS occur in lymph nodes, their involvement of extranodal sites throughout the body has been described. The tonsils are the most common extranodal site in the head and neck. Other sites include the nasopharynx, parapharyngeal space, maxillary alveolar ridge, hard and soft palate [1-4]. To date, no more than five FDCS of the soft palate have been reported in the English literature.
Follicular dendritic cell sarcoma (FDCS) is located primarily in the germinal centers of secondary lymphoid organs and the function is to present antigens to specialized lymphocytes. Surgery is the mainstay of treatment and should include diligent control of surgical margins. The role of adjuvant therapy remains undefined. The follicular dendritic cells known as reticular dendritic cells are identified histologically for their oval to triangular nuclei, delicate nuclear membrane, small central nucleoli and indistinct cytological borders. Some cells may be binucleated or multinucleated. In this article we present a case of the follicular dendritic cell tumor occuring in the soft palate and review the related literature.
Case report
A 59-year-old woman was referred to our otorhinolaryngology department for investigation of a mass in her oropharyngeal region. Her social history was notable for smoking 1 pack per day for the past 20 years, and a tonsillectomy was performed 10 years ago. The ENT examination revealed a swollen, indurate mass that featured necrotic ulcerative areas and compressed parapharyngeal space (Figure 1). Neck ultrasonography showed no enlarged lymph nodes. Pharynx MRI scan revealed a 4.7×3.0×3.5 cm mass at the right side of the parapharyngeal space (Figure 2). Microscopic examination of the biopsy specimen showed oval to spindle cells with an oval nucleus and empty cytoplasm, located in a fascicular sheet pattern beneath the stratified squamous epithelium. The patient underwent a tumorectomy, excision of the mass showed a 4.7cm solid tumor (Figure 3). Clinically, the tumor was directly connected to the right soft palate. Cytologically, tumor cells had a moderate amount of cytoplasm with indistinct cell borders and some had elongated cytoplasmic processes. Nuclei were variable in size, with irregular but delicate nuclear membranes, finely granular to vesicular chromatin and conspicuous nucleoli. Histologically, tumor cells were polygonal, oval to spindle-shaped, and arranged in solid sheets with focal fascicular and vague storiform patterns and diffusely sprinkled with small mature lymphocytes and plasma cells (Figures 4, 5 and 6). The pathology study included a battery of immunohistochemical tests that enabled inflammatory lesions, lymphomas or epithelial neoplasms to be ruled out; nevertheless, CD21 and CD23 markers characteristic of follicular dendritic cells were detected (Figure 7). No immunoreactivity was found for S-100 protein, AE1/AE3 keratin, SMA, CD68. The biopsy established a definitive diagnosis of follicular dendritic cell sarcoma. The patient was treated with a course of adjuvant postoperative radiotherapy. The patient was free of disease 1 year after the end of the treatment.
Figure 1.

A 4.7 cm×3.0 cm, hard, ulcerated mass involving the right lingual side and the soft palate.
Figure 2.

Pharynx MRI scan showed a 47×30×45 mm, low density lesion at the right side of the parapharyngeal space.
Figure 3.

Surgical specimen shows irregular round mass measuring 4.7×3.0×3.5 cm in size beneath the epithelial tissue of the right soft palate.
Figure 4.
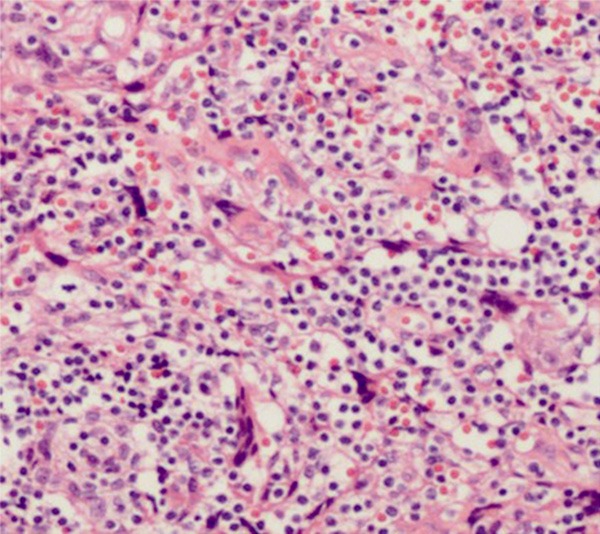
FDCS composed of ovoid cells with eosinophilic cytoplasm. Nuclei are vesicular with small nucleoli and occasional mitotic figures.
Figure 5.
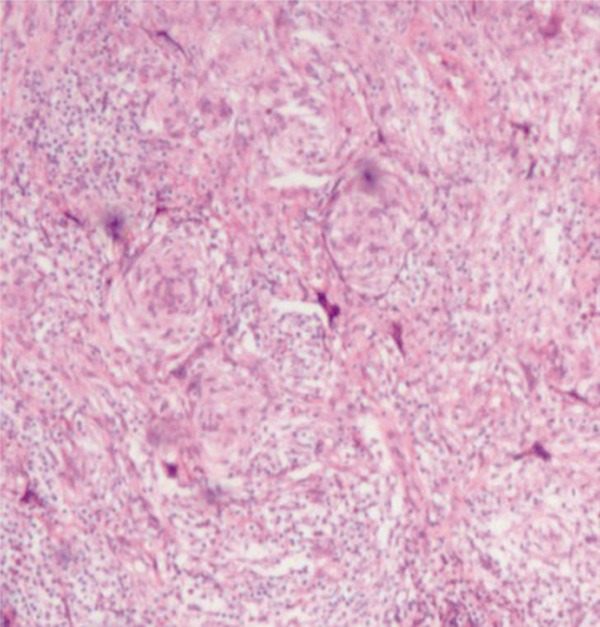
The tumor cells form whorled or storiform patterns.
Figure 6.
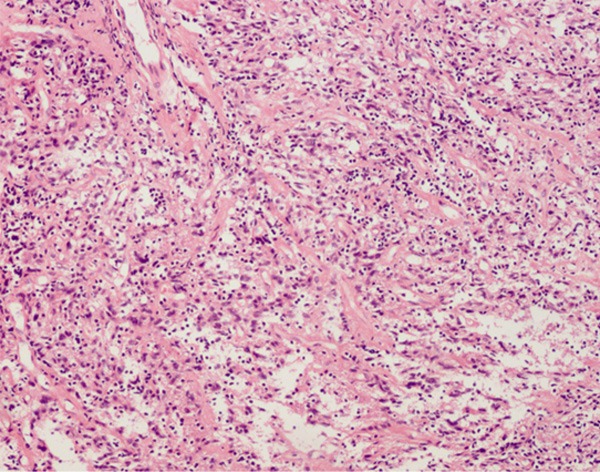
The spindle tumor cells showed vesicular nuclei, small nucleoli, and indistinct cytoplasmic borders.
Figure 7.
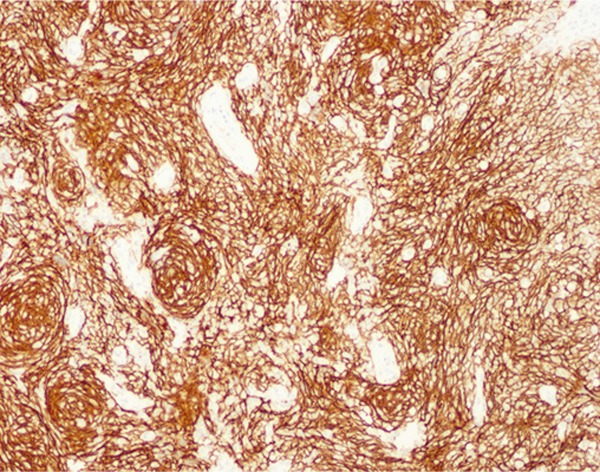
The tumor cells show intense staining with the CD21. The whorled arrangement of tumor cells is well highlighted.
Discussion
The FDCS is an infrequent nonlymphoid malignant tumor accounting for less than 1% of all head and neck tumors which participate in the immune system by presenting and retaining antigens for B cells and stimulating B-cell proliferation and differentiation [5,6]. It causes lymphadenopathy of the cervical and axillary regions and of extranodal sites such as tonsils, palate, pharynx, soft tissues, pancreas, and mesocolon [7]. The most frequently involved extranodal sites are the intraabdominal organs and tonsils. Extranodal FDCS of the pharyngeal region is often misdiagnosed because the FDCS markers are not routinely applied in the immunohistochemical evaluation of poorly differentiated neoplasms, despite it has the characteristic histopathologic features and the distinctive immunophenotype [5]. The FDCS is frequently misdiagnosed as leiomyosarcoma Hodgkin’s disease, meningioma and inflammatory pseudotumor. Duan et al reported approximately 58% of the cases were misdiagnosed initially in previously published reports [8].
The follicular dendritic cell tumor is a lesion commonly seen in young adults and middle-aged adults. The average age of occurrence is 46 years [9]. Although, there is no predilection for gender. It was first described in 1986 by Monda [10], and there are no more than 80 cases reported in the head and neck [5]. Some cases indicated that EBV particles are found in the nuclei of the tumor cells [11], but we have been unable to detect any of these factors in our case.
In the head and neck region, the correct diagnosis of FDCS depends on the imaging studies and clinical history; if it is not conclusive, a broader biopsy or complete resection of the tumor should be performed. Follicular dendritic cell sarcoma is a rare neoplasm which is generally been considered an intermediate-grade malignancy. Aydin et al reported that the overall rates of recurrence, metastasis, and mortality for cases of FDCS are 43%, 24% and 17%, respectively [2]. Metastases to the liver, lung, and lymph nodes has been reported [12].
The immunohistochemical technique is essential for accurately identifying this class of tumors. Appropriate immunohistochemical studies, specifically with CD21 and CD35 markers, should be done on tissue specimens that have a sarcomatoid histological pattern. Markers such as CD21 and CD35, or CD23 are considered to be a distinctive feature of this tumor. Some literatures suggest that when the neoplastic cells are immunoreactive for one or more of the FDC markers, including CD21, CD23, CD35. It may be the consensus that the diagnosis of FDCS is established [1,5]. The current case was immunoreactive for CD21 and for CD23 but not for CD35. FDCS also stain positive for vimentin, desmoplakin and epithelial membrane antigen (EMA). Variability for S-100 should also be taken into account in making a differential diagnosis with some melanomas.
Wide excision of the tumor is the primary treatment of FDCS, postoperative radiotherapy and polychemotherapy are mainly reserved for cases of incomplete resection or poor prognosis, but both have not been shown to increase long-term survival [12,13]. Some authors advocate surgical removal of the regional lymphatic drainage system is necessary if you find evidence of metastasis from an imaging test [3]. Because of the limited number of postoperative follow-up, it is difficult to define the role of radiation therapy and chemotherapy. We opted for postoperative radiotherapy, owing to the size of the neoformation resected, despite the surgical margins were free of tumor infiltration.
Conclusion
The FDCS is a very rare tumor that can occur in either nodal or extranodal sites, most commonly presents as a single mass in the head and neck region. Since the first reported cases in 1986, the more relevant reports of this tumor have increased our ability to diagnose these rare malignancies. Surgical removal of the tumor is the primary treatment in most patients. The accumulation of cases in the literature and study about these patients’ clinical course will probably provide greater recognition of this rather uncommon type of sarcoma.
Disclosure of conflict of interest
None.
References
- 1.Biddle DA, Ro JY, Yoon GS, Yong YW, Ayala AG, Ordonez NG, Ro J. Extranodal follicular dendritic cell sarcoma of the head and neck region: three new cases, with a review of the literature. Mod Pathol. 2002;15:50–58. doi: 10.1038/modpathol.3880489. [DOI] [PubMed] [Google Scholar]
- 2.Aydin E, Ozluoglu LN, Demirhan B, Arikan U. Follicular dendritic cell sarcoma of the tonsil: case report. Eur Arch Otorhinolaryngol. 2006;263:1155–1157. doi: 10.1007/s00405-006-0124-9. [DOI] [PubMed] [Google Scholar]
- 3.Clement P, Saint-Blancard P, Minvielle F, Le Page P, Kossowski M. Follicular dendritic cell sarcoma of the tonsil: a case report. Am J Otolaryngol. 2006;27:207–210. doi: 10.1016/j.amjoto.2005.09.003. [DOI] [PubMed] [Google Scholar]
- 4.Mondal SK, Bera H, Bhattacharya B, Dewan K. Follicular dendritic cell sarcoma of the tonsil. Natl J Maxillofac Surg. 2012;3:62–64. doi: 10.4103/0975-5950.102165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Satoh K, Hibi G, Yamamoto Y, Urano M, Kuroda M, Nakamura S. Follicular dendritic cell tumor in the oro-pharyngeal region: report of a case and a review of the literature. Oral Oncol. 2003;39:415–419. doi: 10.1016/s1368-8375(02)00138-0. [DOI] [PubMed] [Google Scholar]
- 6.Fonseca R, Yamakawa M, Nakamura S, van Heerde P, Miettinen M, Shek TW, Myhre Jensen O, Rousselet MC, Tefferi A. Follicular dendritic cell sarcoma and interdigitating reticulum cell sarcoma: a review. Am J Hematol. 1998;59:161–167. doi: 10.1002/(sici)1096-8652(199810)59:2<161::aid-ajh10>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 7.Romero-Guadarrama MB, Reyes-Posada O, Hernandez-Gonzalez MM, Duran-Padilla MA. Follicular dendritic cell sarcoma/tumor: 2 cases of a rare tumor of difficult clinical and pathological diagnosis. Ann Diagn Pathol. 2009;13:257–262. doi: 10.1016/j.anndiagpath.2008.02.013. [DOI] [PubMed] [Google Scholar]
- 8.Duan GJ, Wu F, Zhu J, Guo DY, Zhang R, Shen LL, Wang SH, Li Q, Xiao HL, Mou JH, Yan XC. Extranodal follicular dendritic cell sarcoma of the pharyngeal region: a potential diagnostic pitfall, with literature review. Am J Clin Pathol. 2010;133:49–58. doi: 10.1309/AJCP7U8YISBUAVNW. [DOI] [PubMed] [Google Scholar]
- 9.Chan JK, Fletcher CD, Nayler SJ, Cooper K. Follicular dendritic cell sarcoma. Clinicopathologic analysis of 17 cases suggesting a malignant potential higher than currently recognized. Cancer. 1997;79:294–313. [PubMed] [Google Scholar]
- 10.Monda L, Warnke R, Rosai J. A primary lymph node malignancy with features suggestive of dendritic reticulum cell differentiation. A report of 4 cases. Am J Pathol. 1986;122:562–572. [PMC free article] [PubMed] [Google Scholar]
- 11.Bai LY, Kwang WK, Chiang IP, Chen PM. Follicular dendritic cell tumor of the liver associated with Epstein-Barr virus. Jpn J Clin Oncol. 2006;36:249–253. doi: 10.1093/jjco/hyl001. [DOI] [PubMed] [Google Scholar]
- 12.Saygin C, Uzunaslan D, Ozguroglu M, Senocak M, Tuzuner N. Dendritic cell sarcoma: a pooled analysis including 462 cases with presentation of our case series. Crit Rev Oncol Hematol. 2013;88:253–271. doi: 10.1016/j.critrevonc.2013.05.006. [DOI] [PubMed] [Google Scholar]
- 13.Hu T, Wang X, Yu C, Yan J, Zhang X, Li L, Li X, Zhang L, Wu J, Ma W, Li W, Wang G, Zhao W, Gao X, Zhang D, Zhang M. Follicular dendritic cell sarcoma of the pharyngeal region. Oncol Lett. 2013;5:1467–1476. doi: 10.3892/ol.2013.1224. [DOI] [PMC free article] [PubMed] [Google Scholar]