

Abstract
Introduction:
This study was carried out at nine (9) special schools for disabled children in Albania. The aim of the study is to determine the caries prevalence and oral hygiene status of children with different disabilities attending different schools for disabled at Albania.
Methods:
Participants are grouped according disability Autistic Spectrum Disorder, Down syndrome, Cerebral Palsy, Mental Retarded, Blind, Deaf-Mute and age group (0-5, 6-10, 11-14, 15-18 years old children). Caries and oral health status were examined and assessed according WHO 1997 criteria.
Results:
Overall caries prevalence at permanent dentition for all groups is 85.3% and for primary dentition 72%. The mean deft index is 3.4 ± 3.5(p≤0.029), mean DMFT= 4.9±4.6 (p≤0.001) with significance difference across type of disability (Kruskal-Wallis test) for both dentition. The mean OHI-S of total population is 1.91; there is significant difference across disability type (p≤0.001, Anova test) for OHI-S index. In total 43.2 % have good, 49.4% fair and 7.4% bad oral hygiene.
Conclusions:
The subjects in this study had a high prevalence of dental caries, poor oral hygiene and need for restorative care.
Keywords: caries, oral health, disability, hygiene
1. INTRODUCTION
Dental caries remains today the most common infectious disease which affects most of the population regardless of age. Caries prevalence is high, and oral hygiene is not good, in poor and developing countries as well as Albania. Several studies have noted that children with disabilities have higher levels of caries, periodontal diseases, and much higher proportion of untreated lesions but less treatment than children without disabilities. Oral health of these children depends on age, type of disability, severity of impairment and living conditions. Other factors that cause high caries prevalence, poor oral hygiene and high proportion of untreated lesions are parents and caregivers lack of information, knowledge and care about oral health of disabled children (1), their socio-economic status and education level. Many individuals with special needs may have great limitations in oral hygiene performance due to their manual dexterity, sensory and intellectual disabilities (5), and so are prone to poor oral health. Different studies carried out for caries prevalence at disabled children comparing that without disabilities shows contradictory results. The aim of this study is to determine the caries prevalence and oral hygiene status at children with various types of disabilities attending different schools for disabled children in Albania.
2. MATERIAL AND METHODS
The study population consist of 638 children aged 3-18 years old form 9 special schools of Albania located at six (6) different cities, the survey sample comprise 599 (94%), six (6) percent were absent during the examination sessions. Informed consent of parents or guardians and school authorities was obtained before the subjects were included in the study. Children that were not cooperative or whose parents have not given consent are excluded from the study. Clinical examinations were carried out at schools, in a school medical room or classroom with natural light. Subjects were placed lying down supine on a desk or an examination couch. The examinations were carried out with the aid of an ordinary mouth mirror and a WHO ball and CPI- tip probe. The data for each subject were recorded on the standard WHO, however several changes were made and special survey form has developed. Children are divided in different groups according type of disability. For each individual dental caries and treatment need is assessed for primary and permanent dentition using deft, defs, DMFT, DMFS indices. Oral hygiene status is calculated using the Simplified Oral Hygiene Index (OHI-S) of Greene and Vermillion. The oral hygiene of each child was classified as ‘good’ when the OHI-S score was 0–1.2, ‘fair’ when it was 1.21–3.1 and ‘poor’ when it was 3.11 up to 6. Children are visually examined for dental hygiene and by passing CPI probe parallel to the buccal and lingual surfaces for the presence of plaque. Data analysis was conducted in SPSS, version 17.0. Chi square test and Fisher’s exact test were used to compare the proportions of categorical variables. On the other hand, ANOVA (analysis of variance) and Kruskal-Wallis test were used to compare mean values of numerical variables between disability groups.
3. RESULTS
Ninety-four percent (94%) or 599 of 638 subjects responded to the call for screening. The mean age of population is 12.00(6.00) years old (Table 1). According of type of disability 84 (1.8%) subject had autism specter disorder, 217 (36.2%) are mental retarded, 26 (4.3%) had cerebral palsy, 147 (24.5%) are deaf-mute, 34 (5.7%) have Down syndrome, 91 (15.2%) are blind (Table 1). Seventy-two (72%) had caries at primary dentition (Tab 2). Down syndrome group has the lowest caries prevalence (54.5%) and cerebral palsy group the highest (83.3%) at primary dentition (Table 2). The mean deft of total sample was 3.4±3.5 while the mean defs was 7.0 ±9.1 (Table 3). There is significant statistical difference between types of disability for deft index (deft p≤0.029, defs p≤0.066 Kruskal-Wallis test) (Tab3). Children with cerebral palsy has the highest deft = 4.5±4 and children with Down syndrome deft = 1.9±2.7 the lowest value (Table 3).
Table 1.
Number and percentage of participants by disability type and age group
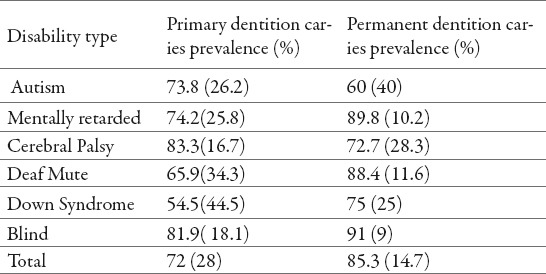
Table 2.
Caries prevalence at primary and permanent dentition by type of disability
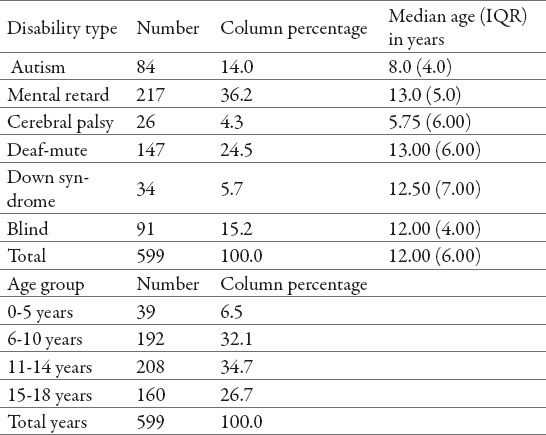
Table 3.
Mean values of DMF(T), DMF(S), def(t) and def(s) by disability type
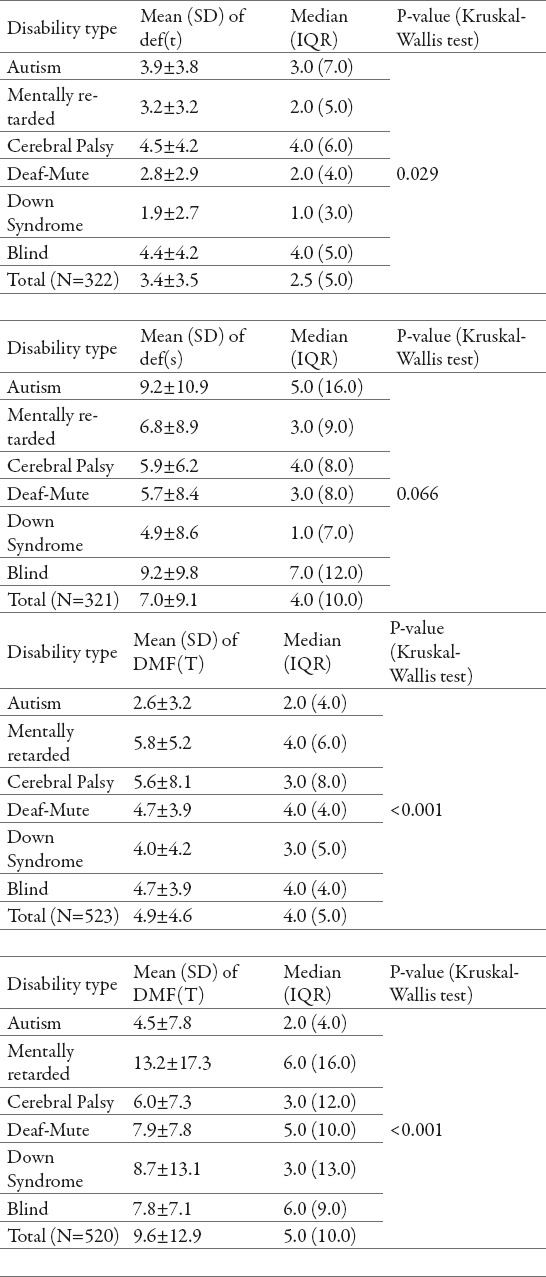
Caries prevalence at permanent dentition is 85.3 % (Tab 2), children with autism specter disorder has the lowest caries prevalence (60.0%) and blind children has the highest (91.0%) (Table 2). The mean DMFT for the total sample is 4.9±4.6 while the mean DMFS is 9.6±12.9 (Table 3). Mentally retarded children has the highest DMFT/ DMFS index (DMFT=5.8±5.2, DMFS=13.2±17.3) and children with autism specter disorder the lowest DMF/DMFS index (DMFT=2.6±3.2, DMFS=4.5±7.8) (Tab 3). There is significant statistical difference between disability types for both DMFT/DMFS index (p≤0.001, Kruskal-Wallis test) (Table 3). The mean OHI-S index of total population is 1.9 (Table 4), children with cerebral palsy has the best oral hygiene with mean OHI-S index and deaf-mute children the worst oral hygiene with mean OHI-S index 2.25 (Table 4).
Table 4.
OHI-S index by type of disability. * P-values from ANOVA (analysis of variance). * Row percentages. ** Chi-square test.
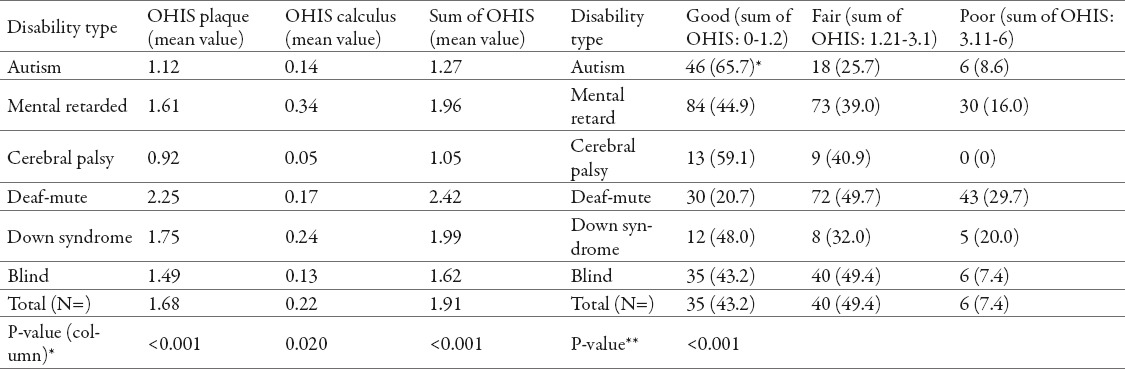
There is statistical significance difference among types of disability (p≤0.001, Chi square test) for OHI-S index (Tab 4). Forty- three (43.2%) of total sample has good oral hygiene, 49.4% fair and 7.4% bad oral hygiene (Table 4).
4. DISCUSSION
According to recent literature, individuals with disability have poor oral health and high treatment need in comparison with people without disability. In our study dental caries prevalence according dentition is 85.3% (n=446) for permanent dentition (Table 2) and 72% (n=232) for primary dentition (Table 2). Our data show high caries prevalence for disabled children, comparing to other studies we find that our values are higher than values showed by (7,8,13,14), similar with (15,16,17) and lower than (18,19,20). Our results are similar to those found by (21) at a study conducted at Tirana, Albania with 12 years old children without disabilities and higher than values find by (22) for caries prevalence at children without disabilities aged 7-15 at Tirana, Albania. Mean and detailed caries prevalence and indices are higher than results found at children without disability (21,22), lower than that reported by (7,8, 14, 17, 23), and similar (13, 19,24,25). The reasons why we have such a variance of results is because of different types of disability, age group and geographical extension selected by authors. According of type of disability our results are similar with those found by (7,11,13,14,20) for permanent dentition. At primary dentition our results are similar with those found by (14) and contrary to those found by (13,17,20,26). There is significant statistic difference for DMFT and deft index according of type of disability, these result are confirmed by (13, 19, 20, 28) but contrary to other authors such as (13,17,25) which didn’t find statistical significance difference between types of disability.
Oral hygiene status of children with disability is not good and this is in accordance with other studies (7,8,11,14,15,19,22). Our mean OHI-S index is 1.91 (Table 4) which is lower than that found by (19, 22). According of type of disability cerebral palsy and autistic specter disorder has the best oral hygiene and deaf-mute group the worst These results are similar with those found by (11, 20) although our values are higher and contrary to those found by (14). “Fair” oral hygiene is the biggest group (49.4%) followed by “good” (43.2%) and “bad” (7.4%) (Tab 4), these results are similar with that found by (7) but contrary to that found by (8,28). There is statistical significance difference among types of disability (p≤0.001, ANOVA test, Tab 4) which is in accordance of study carried out by (28), other authors such as (17). A very high caries experience and poor oral hygiene status demands immediate attention to increase efforts for prevention and treatment of oral diseases in these special groups of children.
5. CONCLUSIONS
From the study result that children with disability has high caries prevalence and bad oral hygiene.
Children’s with disability needs more dental treatment and care from their parents and caregivers.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Isman B, Newton R, Bujold C, Baer MT. Los Angeles, CA: University of Southern California University Affiliated Program, Children's Hospital; 2000. Planning guide for dental professionals serving children with special health care needs. [Google Scholar]
- 2.Brown JP. The efficacy and economy of comprehensive dental care for the handicapped children. Int Dent J. 1980;30:14–27. [PubMed] [Google Scholar]
- 3.Ajami, et al. Dental treatment needs of children with disabilities. JODDD. 2007;1(2):93–98. doi: 10.5681/joddd.2007.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Oredugba FA, Akindayomi Y. Oral health status and treatment needs of children and young adults attending a day centre for individuals with special health care needs. BMC Oral Health. 2008;8:30. doi: 10.1186/1472-6831-8-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Vigild M. Dental Canes experience among children with Down's syndrome. J Ment Deflc Res. 1986;30(3):271–276. [PubMed] [Google Scholar]
- 6.Rao DB, Hegde AM, Munshl AK. MangaloreCaries prevalence amongst handicapped children of South Canara district, Karnataka. J Indian Soc Pedod Prev Dent. 2001;19(2):67–73. [PubMed] [Google Scholar]
- 7.Mitsea AG, Karidis AG, Donta-Bakoyianni C, Spyropoulos ND. J Clin Pediatr Dent Fall. 2001;26(1):111–118. doi: 10.17796/jcpd.26.1.705x15693372k1g7. [DOI] [PubMed] [Google Scholar]
- 8.Vignesha H, Soh G, Loe GL, Chellappah NK. Dental health of disabled children In Singapore Aust Den. 1991;36(2):151–156. doi: 10.1111/j.1834-7819.1991.tb01345.x. [DOI] [PubMed] [Google Scholar]
- 9.Shankar B, Tewarl A, Jam RL, Verma SK. A study of prevalence of severity of dental caries in children of different mtelligence quotient levels. J Ind Dent Assoc. 1983;55:413–417. [PubMed] [Google Scholar]
- 10.Altun, et al. Eur J Dent. 2010;4(4):361–366. [PMC free article] [PubMed] [Google Scholar]
- 11.Khadem P, Karami M, Salehinia R. J Mash Dent Sc. 2012;35(4):253–262. [Google Scholar]
- 12.Acharya J, Chansatitporn N, Narkasawat K. 2. Vol. 5. Nepal: Webmed Central Dentistry; 2014. Dental Caries Status And Oral Health Needs among Disabled Children Living In Care Centers In Kathmandu Valley; p. WMC004539. [Google Scholar]
- 13.Al Qahtani Z, Wyne AH. 105. Vol. 27. Saudi Arabia: Odontostomatol Trop; 2004. Caries experience and oral hygiene status of blind, deaf and mentally retarded female children in Riyadh; pp. 37–40. [PubMed] [Google Scholar]
- 14.Hysi, et al. 4. Vol. 9. Albania: OHDMBSC; 2010. Dental Caries Experience and Oral Health Behaviour Among 12-Year-Olds in the City of Tirana; pp. 229–233. [Google Scholar]
- 15.Lagana, et al. Caries prevalence in a 7- to 15-year-old Albanian schoolchildren population. Ann Stomatol (Roma) 2012;3(2):38–43. [PMC free article] [PubMed] [Google Scholar]
- 16.Totolici, et al. 1. Vol. 3. OHDMBSC; 2004. Study regarding the oral health in children from the Constanta city School for the disabled; pp. 12–15. [Google Scholar]
- 17.Vellappally, et al. The prevalence of malocclusion and its association with dental caries among 12-18-year-old disabled adolescents. BMC Oral Health. 2014;14:12. doi: 10.1186/1472-6831-14-123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jokic, et al. Dental Caries in Disabled Children. Coll. Antropo. 2007;1:321–324. [PubMed] [Google Scholar]
- 19.Simon ENM, Matee MI, Scheutz F. Oral Health Status of Handicapped Primary School Pupils in Dar Es Salaam, Tanzania. East African Medical Journal. 2008;85(3):113–117. [PubMed] [Google Scholar]
- 20.Desai M, Messer LB, Calahce H. 1. Vol. 46. Australia: Australian Dental Journal; 2010. A study of dental treatment needs of children with disabilities in Melbourne; pp. 41–50. [DOI] [PubMed] [Google Scholar]
- 21.Jain, et al. Oral health status of mentally disabled subjects in India. Journal of Oral Science. 2009;51(3):333–340. doi: 10.2334/josnusd.51.333. [DOI] [PubMed] [Google Scholar]