

Abstract
The comma sign was described as an arthroscopic landmark to identify the torn subscapularis stump to mobilize and repair the tendon in anterosuperior rotator cuff tears. It was hypothesized that it is composed of the humeral attachments of the superior glenohumeral and coracohumeral ligaments. This arthroscopic finding has since become accepted orthopaedic nomenclature pathognomonic for subscapularis tears and a key component of subscapularis tear classification. We propose an alternative theory of the pathoanatomy of the comma sign in anterosuperior rotator cuff tears and present the technique of comma sign–directed repairs of combined subscapularis and supraspinatus lesions. After appropriate releases, tendon-to-tendon repair of the distal-superior aspect of the comma sign to the upper border of the remnant subscapularis results in anatomic re-creation of the intra-articular portion of the torn subscapularis with concomitant reduction of the anterior leading edge of the supraspinatus and reconstitution of the rotator cable complex. A tension-free, single-anchor subscapularis repair is then performed to secure the tendon to the lesser tuberosity. After subscapularis repair, the supraspinatus that was previously retracted to the glenoid rim takes the appearance of a crescent-type tear that is easily approximated to its anatomic insertion.
The leading edge of a torn subscapularis can be difficult to identify arthroscopically because of retraction and scarring in anterosuperior rotator cuff tears. In 2003 Lo and Burkhart1 described the comma sign as an arthroscopic landmark to identify the torn subscapularis stump to mobilize and repair the tendon. They described the comma sign as tissue composed of the humeral attachments of the superior glenohumeral and coracohumeral ligaments that concomitantly tear and remain attached to the superolateral corner of the subscapularis. This arthroscopic finding has since become accepted orthopaedic nomenclature pathognomonic for subscapularis tears and a key component of subscapularis tear classification.2,3 We propose an alternative theory of the pathoanatomy of the comma sign in anterosuperior rotator cuff tears and present the technique of comma sign–directed repairs of combined subscapularis and supraspinatus lesions.
Surgical Technique
Patient Positioning, Diagnostic Arthroscopy, and Initial Portal Placement
The patient is positioned in the beach-chair position with the shoulder in approximately 30° of forward flexion using 3 kg of suspended traction on a regular electric surgical table. It is vital to ensure adequate clearance of the posterior shoulder during positioning to perform the procedure. An interscalene block and general anesthesia are routinely used. We do not use any commercially available limb positioners for shoulder arthroscopy.
A standard posterior viewing portal is created approximately 2 cm inferior and 2 cm medial to the posterolateral border of the acromion. The arthroscope is atraumatically introduced into the glenohumeral joint, and a diagnostic arthroscopy is performed. A standard anterior portal is created with spinal needle localization just lateral to the tip of the coracoid, and a probe is introduced. A lateral portal is also created at the midglenoid level in the sagittal plane, which is approximately at the level of the posterior acromioclavicular joint. This portal allows excellent access to the anterior shoulder through the supraspinatus tear.
Any cartilage or labral pathology is noted. The biceps tendon is examined for both tendon disease and subluxation or dislocation. The tendon can be pulled into the joint for visualization of any tenosynovitis within the bicipital groove. Shoulder flexion and internal rotation can help to visualize the biceps more distally within the pulley. Full-thickness supraspinatus tears are documented by viewing the uncovered area of the greater tuberosity and communication with the subacromial space superiorly.
Visualization of Subscapularis Tear and Comma Sign From Posterior Portal
While the surgeon is viewing from the posterior portal, the retracted subscapularis and comma sign are seen as an abnormal vertical structure just anterior and lateral to the glenoid labrum, superior to the upper border of the remnant subscapularis (Video 1). In most cases there is still subscapularis tissue traversing the joint horizontally toward the lesser tuberosity (Fig 1). While the surgeon is working through both the anterior and lateral portals, the rotator interval is debrided medial to the comma sign tissue. Extreme care is taken to preserve the comma sign tissue. The superior, lateral, and inferior borders of the coracoid, as well as the deep surfaces of the conjoint tendon and coracoacromial ligament, are defined. The arthroscope is then placed in the subacromial space, and a routine bursectomy and acromioplasty are performed.
Fig 1.
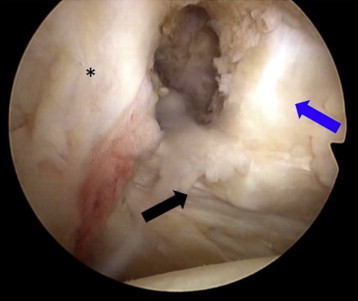
The comma sign tissue (blue arrow) is seen as a vertical structure parallel to the anterior glenoid labrum (asterisk) and attached to the remnant upper border of the subscapularis (black arrow) when viewed from the posterior portal of a right shoulder with the patient in the beach-chair position.
Optimal Visualization of Subscapularis Tear From Lateral Portal
The arthroscope is placed in the lateral portal, and an anterolateral portal is created just off the anterolateral aspect of the acromion midway between the anterior and lateral portals. Most of the diagnostic and therapeutic subscapularis maneuvers are performed from the anterolateral portal while the surgeon is viewing laterally. An initial coracoid dissection and interval debridement are performed while the surgeon is viewing posteriorly, but all releases are completed while viewing and working laterally. The coracohumeral ligament is released at the posterolateral aspect of the coracoid to mobilize the retracted subscapularis. The subscapularis is released along its superior border inferior to the coracoid, along its deep border anterior to the scapula, and along its anterior border deep to the conjoint tendon. The axillary nerve is identified and protected just medial to the medial border of the conjoint tendon, and the rest of the brachial plexus can be visualized as well. Axillary nerve dissection and protection are necessary to perform adequate subscapularis mobilization in retracted tears.
The medial biceps sling is examined. There is often a remnant attachment of the medial sling present, and the biceps is subluxated but not fully dislocated. Even at this point, most of the subscapularis may still appear intact. The remnant medial sling fibers are resected, and the severity of the subscapularis tear becomes evident because the bare lesser tuberosity can now be fully visualized. An arthroscopic biceps tenodesis is performed with a suture anchor within the upper portion of the bicipital groove (5.5-mm Insite FT PEEK [polyether ether ketone] Optima Suture Anchor; Tornier, Montbonnot Saint Martin, France). Removing the biceps from this area allows a thorough assessment to the subscapularis insertion.
The exposed lesser tuberosity and greater tuberosity are lightly debrided to a bleeding surface. The supraspinatus tear is also examined at this time, and a deep release is performed by debriding tissue from the base of the coracoid to the superior capsule deep to the supraspinatus tendon, working posteriorly to the infraspinatus. Care is taken to avoid dissection posteriorly in proximity to the suprascapular nerve in the spinoglenoid notch.
Optimal Visualization of Comma Sign Tissue From Lateral Portal
After the subscapularis and supraspinatus have been fully released, the comma sign tissue is examined from the lateral portal. While using a grasper from the anterolateral portal, the surgeon pulls the subscapularis and supraspinatus to their anatomic insertions. A traction suture is also placed through the upper border of the subscapularis to facilitate examination and reduction. When pulled through the anterior portal, the subscapularis is pulled away from the lesser tuberosity and the extent of the tear can be examined. Pulling through the anterolateral portal facilitates tear reduction. As the tear is examined, the comma tissue is grasped as well, and it becomes evident that the tissue may represent a horizontal cleavage tear of the subscapularis.
Comma Sign–Directed Repair
While working through the anterior portal, the surgeon uses a tissue penetrator (Clever Hook; DePuy Mitek, Raynham, Massachusetts) to pass a suture through the lateral aspect of the comma sign tissue (2.0 Force Fiber; Tornier). The suture is then retrieved within the glenohumeral joint with a suture penetrator through the lateral aspect of the upper border of the remnant subscapularis (Fig 2). The suture is tied using a sliding-locking knot, the comma sign tissue is reduced to the rest of the subscapularis, and the horizontal cleavage tear is repaired (Fig 3). A suture anchor is then placed in the lesser tuberosity and passed through the lateral subscapularis to anatomically reduce and stabilize the complete subscapularis (5.5-mm Insite FT PEEK Optima Suture Anchor). The supraspinatus tear is now examined, and it is evident that because of the incorporation of the horizontal cleavage tear, nearly complete reduction of the anterior leading edge of the supraspinatus is accomplished. The supraspinatus tendon is repaired according to our preferred technique.4 The arthroscope can then be placed back into the glenohumeral joint to visualize the repair from the posterior portal to confirm an anatomic reconstruction (Fig 4).
Fig 2.
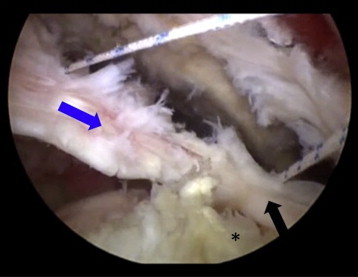
After appropriate releases, a free suture has been passed in a side-to-side fashion with a tissue penetrator through the comma sign tissue (blue arrow) and the remnant lateral upper border of the subscapularis (black arrow), with viewing from the lateral portal. An anchor will eventually be placed in the exposed lesser tuberosity (asterisk) to complete the subscapularis repair.
Fig 3.
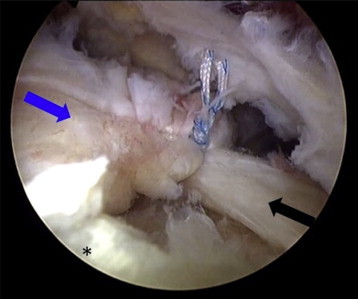
Tying the side-to-side stitch of the upper border of the subscapularis (black arrow) indirectly reduces the leading edge of the supraspinatus (blue arrow) to its insertion on the greater tuberosity (asterisk).
Fig 4.
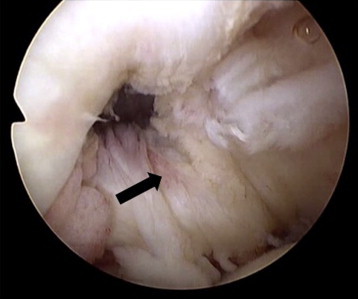
The reconstitution of the upper border of the subscapularis (arrow) is visualized from the posterior portal from an intra-articular view after the repair of the comma sign tissue to the remnant intact lateral subscapularis has been performed.
Postoperative Rehabilitation
The rehabilitation protocol is similar to that of a standard rotator cuff repair with a focus on early mobilization and self-directed stretching. The arm is initially placed in a 20° abduction brace for 1 month and then transitioned to a regular sling for an additional 14 days. A self-stretching program emphasizing passive and active-assisted motion is begun the day after surgery. Full active range of motion is allowed at 6 weeks, all activities of daily living are generally resumed by 12 weeks, and the patient is allowed to return to all activities at 6 months postoperatively. No specific strengthening exercises are used because resumption of normal activities usually adequately strengthens the shoulder while protecting the repair during the healing phase.4
Discussion
Walch et al.5 first defined subscapularis tears as “hidden lesions” in the era of open rotator cuff surgery in 1994. Unexpected subscapularis tears were identified in 16% of patients with alleged isolated supraspinatus tears after Walch et al. performed systematic rotator interval exploration. The subscapularis tears were described as hidden because the superficial fascia overlying the subscapularis insertion on the lesser tuberosity remained intact despite a tear. Shoulder arthroscopy has since revolutionized the treatment of rotator cuff pathology, and the intraoperative identification of subscapularis tears is now much easier with the arthroscope than with open surgery. However, defining normal and abnormal anatomy is often not intuitive even with the use of arthroscopy, which can be especially challenging in retracted subscapularis tears.2 Using pathoanatomic landmarks is pivotal for identification, mobilization, and anatomic repair of retracted rotator cuff tears, and the description of the comma sign by Lo and Burkhart1 is a significant contribution to our arthroscopic understanding and management of subscapularis tears.
In our experience the presence of the comma sign is pathognomonic for combined retracted subscapularis and supraspinatus tears. However, our definition of the comma sign pathoanatomy differs from the original description by Lo and Burkhart.1 There are no anatomic studies, to our knowledge, that validate the original comma sign pathoanatomic theory, and it is unclear why the coracohumeral and superior glenohumeral ligament would take a vertical orientation that represents the comma sign. We believe that it is more likely that the comma sign represents a subscapularis horizontal cleavage tear that assumes its vertical orientation because of the resultant superomedial vector on the tissue from the retracted supraspinatus tear. Therefore we routinely repair the comma sign tissue with a side-to-side stitch to the remaining upper border of the subscapularis before repairing back to the lesser tuberosity. In our experience this effectively reduces the anterior leading edge of the supraspinatus through the lateral connection between the supraspinatus and subscapularis at the top of the intertubercular groove. Retracted, combined subscapularis and supraspinatus tears can be challenging to repair, but understanding the comma sign pathoanatomy and comma sign–directed repair sequence can simplify the management of these tears significantly (Table 1).
Table 1.
Surgical Pearls
| The presence of the comma sign is pathognomonic for combined, retracted subscapularis and supraspinatus tears. |
| The comma sign tissue may represent a horizontal cleavage tear of the subscapularis that assumes its vertical orientation because of the resultant superomedial vector on the tissue from the retracted supraspinatus tear. |
| Optimal visualization of subscapularis tears and the comma sign tissue is achieved by viewing through the lateral portal. |
| After appropriate releases, a side-to-side repair of the comma sign tissue to the remnant upper border of the subscapularis effectively reduces the anterior leading edge of the supraspinatus through the lateral connection between the supraspinatus and subscapularis at the top of the intertubercular groove. |
| After repair of the subscapularis, the supraspinatus tendon that was previously retracted to the glenoid rim takes the appearance of a crescent-type tear that is easily approximated to its anatomic insertion. |
| Retracted, combined subscapularis and supraspinatus tears can be challenging to repair, but understanding the comma sign pathoanatomy and comma sign–directed repair sequence can simplify the management of these tears significantly. |
The comma sign tissue may represent a horizontal cleavage of the upper border of the subscapularis in retracted, combined supraspinatus and subscapularis tears. Initial reduction of the comma sign tissue to the upper border of the remnant subscapularis results in concomitant reduction of the supraspinatus from its retracted position and facilitates anatomic repair of anterosuperior rotator cuff tears.
Footnotes
The authors report the following potential conflict of interest or source of funding: L.N. receives support from Tornier.
Supplementary Data
Technique for comma sign–directed repair of combined supraspinatus and subscapularis tears. The comma sign tissue is identified and then repaired to the remnant upper border of the subscapularis in a side-to-side fashion. This not only anatomically reduces the horizontal cleavage tear in the subscapularis but also reapproximates the retracted leading edge of the supraspinatus.
References
- 1.Lo I.K., Burkhart S.S. The comma sign: An arthroscopic guide to the torn subscapularis tendon. Arthroscopy. 2003;19:334–337. doi: 10.1053/jars.2003.50080. [DOI] [PubMed] [Google Scholar]
- 2.Burkhart S.S., Brady P.C. Arthroscopic subscapularis repair: Surgical tips and pearls A to Z. Arthroscopy. 2006;22:1014–1027. doi: 10.1016/j.arthro.2006.07.020. [DOI] [PubMed] [Google Scholar]
- 3.Toussaint B., Barth J., Charousset C. New endoscopic classification for subscapularis lesions. Orthop Traumatol Surg Res. 2012;98:S186–S192. doi: 10.1016/j.otsr.2012.10.003. (suppl) [DOI] [PubMed] [Google Scholar]
- 4.Neyton L., Godenèche A., Nové-Josserand L., Carrillon Y., Cléchet J., Hardy M.B. Arthroscopic suture-bridge repair for small to medium size supraspinatus tear: Healing rate and retear pattern. Arthroscopy. 2013;29:10–17. doi: 10.1016/j.arthro.2012.06.020. [DOI] [PubMed] [Google Scholar]
- 5.Walch G., Nove-Josserand L., Levigne C., Renaud E. Tears of the supraspinatus tendon associated with “hidden” lesions of the rotator interval. J Shoulder Elbow Surg. 1994;3:353–360. doi: 10.1016/S1058-2746(09)80020-7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Technique for comma sign–directed repair of combined supraspinatus and subscapularis tears. The comma sign tissue is identified and then repaired to the remnant upper border of the subscapularis in a side-to-side fashion. This not only anatomically reduces the horizontal cleavage tear in the subscapularis but also reapproximates the retracted leading edge of the supraspinatus.