

Abstract
Tibial eminence avulsion fractures are rare injuries occurring mainly in adolescents and young adults. When necessary, regardless of patient age, anatomic reduction and stable internal fixation are mandatory for fracture healing and accurate restoration of normal knee biomechanics. Various arthroscopically assisted fixation methods with sutures, anchors, wires, or screws have been described but can be technically demanding, thus elongating operative times. The purpose of this article is to present a technical variation of arthroscopic suture fixation of anterior cruciate ligament avulsion fractures. Using thoracic drain needles over 2.4-mm anterior cruciate ligament tibial guidewires, we recommend the safe and easy creation of four 2.9-mm tibial tunnels at different angles and at specific points. This technique uses thoracic drain needles as suture passage cannulas and offers 4-point fixation stability, avoiding potential complications of bony bridge fracture and tunnel connection.
Avulsion fractures of the anterior cruciate ligament (ACL) from the tibial eminence are rare injuries occurring mainly in children and adolescents.1 In 1959, Meyers and McKeever2 proposed a classification system for these fractures, according to which type I fractures are nondisplaced; type II, or “bird-beak,” fractures produce displacement of the anterior margin while the posterior part is still seated onto the tibia; and type III fractures are completely displaced. Later, Zaricznyj3 added a fourth type with complete fragment comminution.1
Regardless of patient age, anatomic reduction and stable internal fixation are mandatory for fracture healing and accurate restoration of normal knee biomechanics, especially for type III and IV fractures or when concomitant chondral, meniscal, or other ligamentous injuries are present.4 Furthermore, the evolution of arthroscopic techniques and the possibility of extension loss after conservative treatment of type II fractures have increased the tendency toward operative treatment of these fractures.4,5
Various fixation methods using screws, wires, anchors, or even “buttons” have been extensively described in the English-language literature with very promising results.1,4,6-10 Among them, suture fixation techniques appear to be the most popular, as well as the most “user-friendly,” among orthopaedic surgeons.1 However, concerns have been raised regarding potential intraoperative complications, difficulties of suture passage, and prolonged operative times. The purpose of this article is to present a technical variation allowing for easy, stable, and safe all-arthroscopic 4-point suture fixation of ACL avulsion fractures.
Surgical Technique
The patient is positioned supine with a thigh tourniquet and the affected limb placed on a standard leg holder allowing full knee range of motion. By use of a 30°, 4.0-mm arthroscope, standard anteromedial (AM) and anterolateral portals are used. The knee joint is evaluated, hematoma is evacuated, and fracture debris or other interposed tissues are removed. Concomitant meniscal tears or other lesions are assessed and addressed before fracture treatment. In most cases the transverse intermeniscal ligament is interposed between the superior displaced fragment and the tibia, obstructing accurate reduction. By use of a probe from the AM portal, the ligament is pulled anteriorly and over the tibial eminence fragment, facilitating the achievement and maintenance of reduction.
A 2-cm anterior oblique incision is made over the AM aspect of the tibia about 4 cm distal to the joint line. Through the AM portal, the ACL tibial drill guide (Linvatec, Largo, FL) is set initially at 55°, and two 2.4-mm guidewires are placed medially and laterally at the posterior aspect of the fragment (posteromedial and posterolateral [PL] holes), 1 to 2 mm outside the perimeter of the fracture crater (Fig 1). The distance between the guidewire entry points at the AM cortex of the tibia is about 15 mm. Two 2.9-mm, 8-French thoracic drain needles (VYGON, Écouen, France) are slid over each guidewire and driven into the joint at specific points (Fig 1). The cutting edge of the thoracic drain needle is strong enough to easily penetrate the cancellous bone of the tibia, and there is no necessity for any additional cannulated drilling over the wires. One No. 5 nonabsorbable Ethibond suture (Ethicon, Somerville, NJ) is introduced through the AM working portal and passed through the posterior portion of the ACL ligament (PL bundle of ACL) using a curved arthroscopic rotator cuff hook grasper (Linvatec). The Ethibond suture is subsequently brought out from the AM portal. One No. 0 polydioxanone suture (PDS) loop (Ethicon) is introduced through each thoracic drain needle into the joint. By means of a probe, each end of the Ethibond suture is passed through the PDS loop and is sequentially withdrawn through the tibial tunnel (Fig 2). The thoracic drain needles are then removed.
Fig 1.
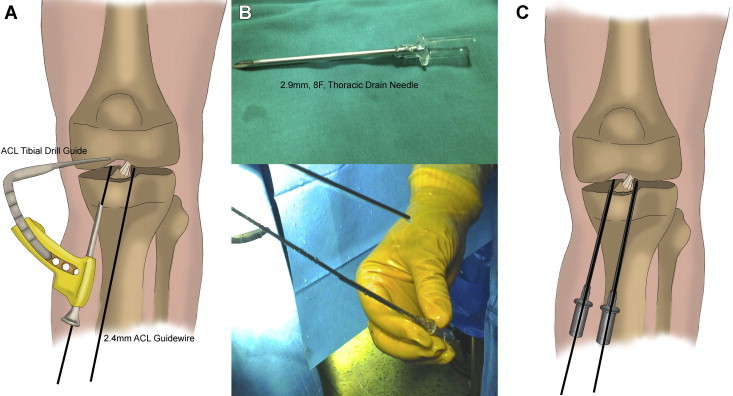
(A) Supine positioning of the patient with a thigh tourniquet and placement of the affected limb on a standard leg holder allowing full knee range of motion. The ACL tibial drill guide is set initially at 55°, and two 2.4-mm guidewires are placed medially and laterally at the posterior aspect of the fragment through the AM portal. (B) A 2.9-mm, 8-French thoracic drain needle. The thoracic drain needles are slid over each guidewire. The cutting edge of the thoracic drain needle is strong enough to easily penetrate the cancellous bone of the tibia. (C) Both needles are driven into the joint at specific points.
Fig 2.
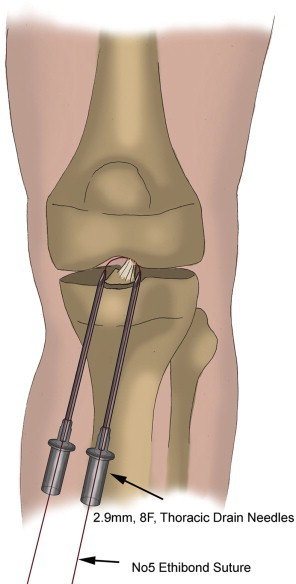
The No. 5 Ethibond sutures are passed through the ACL mass (PL bundle initially) and withdrawn through the thoracic drain needle cannulas at the AM aspect of the tibia using a PDS loop.
Subsequently, the ACL tibial drill guide (Linvatec) is set at 45° to avoid connection with the previously made bone tunnels. In a similar fashion, two 2.4-mm guidewires are placed medially and laterally at the anterior aspect of the ACL avulsion fragment (AM and anterolateral holes), 1 to 2 mm outside the perimeter of the fracture crater (Fig 3). The distance between the 2 guides at the AM cortex of the tibia is about 15 mm, and the guides are placed about 15 mm superior to the previous tunnels. The same sequence is followed, as previously described, to engage the anterior part of the ACL (AM bundle), and with the assistance of the 2 thoracic drain needles, one No. 5 Ethibond suture was pulled out through the anterior tibial tunnel (Fig 3). Finally, after anatomic reduction of the avulsed fragment that is achieved and held with the aid of the arthroscopic probe, the sutures from the posterior tunnels (PL bundle) are tied over the tibial cortex at 50° of knee flexion, and the same procedure is followed for the sutures from the anterior tunnels (AM bundle) at 20° of knee flexion (Video 1, Table 1).
Fig 3.
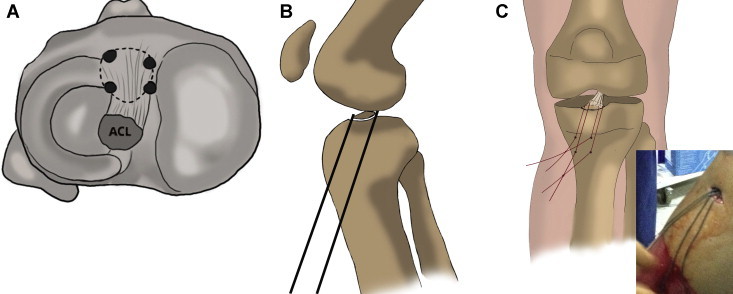
(A) Transverse section of tibia showing 4 tunnels in relation to ACL fragment. The technique provides 4-point fixation. (B) Sagittal section of knee joint showing position of posterior and anterior tunnels. (C) All the sutures are withdrawn at the AM part of the tibia and are ready to be tied. Approximately 15 mm of bony bridge is preserved among the 4 tibial tunnels. First, the sutures of the PL bundle are tied at 50° of knee flexion; then, the sutures of the AM bundle are tied at 20° of knee flexion.
Table 1.
Indications and Surgical Steps of Arthroscopic 4-Point Suture Fixation of ACL Tibial Avulsion Fractures Using Thoracic Drain Needles
| Indications |
| Mainly type III and IV fractures, as well as most type II fractures |
| All fracture types with concomitant ligamentous injuries, chondral lesions, meniscal tears, or meniscal root avulsions |
| Surgical steps and tips |
| Knee joint preparation |
| Create standard anterolateral and AM knee arthroscopic portals. |
| Perform arthroscopic knee joint evaluation. |
| Assess and address concomitant lesions initially. |
| Perform evacuation of hematoma. |
| Pull the intermeniscal ligament anteriorly, and provisionally reduce the fracture. |
| Tunnel placement and suture passage |
| Make a 2-cm incision over the AM aspect of the tibia (4 cm below the joint line). |
| Set the ACL tibial drill guide at 55°. |
| Place two 2.4-mm ACL guidewires medially and laterally at the posterior aspect of the fragment. |
| Slide 2 thoracic drain needles into the joint over each ACL guidewire. |
| Remove the guidewires. |
| Using a curved arthroscopic rotator cuff hook grasper, pass a No. 5 Ethibond suture through the PL bundle of the ACL. |
| Using a PDS loop, withdraw the Ethibond suture through each thoracic drain needle. |
| Remove the thoracic drain needles. |
| Set the ACL tibial drill guide at 45°. |
| Place two 2.4-mm ACL guidewires medially and laterally at the anterior aspect of fragment. |
| Repeat the procedure with the thoracic drain needles and Ethibond suture to engage the anterolateral bundle of the ACL. |
| Fragment fixation and knot tying |
| Hold fragment reduction with the arthroscopic probe. |
| Tie the sutures of the PL bundle at 50° of knee flexion. |
| Tie the sutures of the AM bundle at 20° of knee flexion. |
In cases with isolated ACL avulsion fractures, a standard postoperative rehabilitation protocol is followed. The knee is placed in a functional brace in extension while isometric strengthening exercises are initiated immediately. In addition, partial weight bearing is permitted. The brace is held in extension for 4 weeks, and then gradually increasing range-of-motion exercises are allowed. This protocol is modified when other concomitant injuries are present.
Discussion
Avulsion fractures of the ACL are uncommon injuries that occur mainly in adolescents or young adults during sporting activities or even bicycle or car accidents.1,11 As mentioned earlier, their management has evolved from traditional open or mini-open techniques to completely arthroscopic techniques using sutures, screws, wires, anchors, or even buttons.4,6-10 When all previous methods are compared, screw fixation seems to have the most equivocal outcomes. Biomechanical studies have shown divergent results regarding ultimate failure rates and fragment displacement, whereas reoperation for hardware removal, possible loss of extension, fracture fragmentation, and residual anteroposterior or rotational instability remain serious concerns.1,4,9
Arthroscopic suture fixation of tibial eminence fractures has been well documented as a technique leading to promising outcomes.4 Regarding the multiple shuttling, tunnel-creating, and suture-passing techniques, it is obvious that such fixation can be a technically demanding procedure.1 In addition, in an effort to achieve maximum stability, authors have supported suture passage through the fragment or the ACL substance and tibial tunnels into the fracture crater using suture passers (Hewson Suture Retrievers; Smith & Nephew, Andover, MA) or even eyed Steinmann pins.1 More recent studies have supported the creation of tunnels just outside the bony crater.12 However, all these solutions provide 2-point fixation, and this might explain the finding of slight postoperative laxity.1 Only 1 recently published study proposed 3-point fixation in cases with anterior-horn lateral meniscus lesions.7 Our study supports 4-point stabilization that allows the surgeon to secure small fragments or even some larger or slightly comminuted fragments in multiple planes. We also believe that it is very important to engage and stabilize the 2 bundles of the ACL (AM and PL bundles) separately, especially in type IV fractures.
Going through the literature, we found that little has been reported regarding the intraoperative difficulties of arthroscopic suture fixation of ACL avulsion fractures.1,6,7 These can include laborious anatomic reduction, inaccurate tunnel placement and breakage of the bony bridge between the tunnels, difficulty in confirming the small 2-mm tibial tunnels and insertion of the suture retrievers through the soft tissues, and finally, loss of reduction during suture tying because of incorrect tunnel orientation. By use of the four 2.4-mm guidewires and, consequently, the four 2.9-mm thoracic drain needles in different planes and in accurate positions, all these difficulties could be overridden and potential complications avoided. Furthermore, in addition to the aforementioned technical advantages, the use of four 2.9-mm tunnels is, in theory, safer regarding potential iatrogenic growth disturbances in skeletally immature patients than the use of 2 larger 5-mm tunnels6 (Table 2).
Table 2.
Advantages of This Technique
| Superior 4-point fixation |
| No additional drilling |
| Bony bridge integrity among the four 2.9-mm tunnels |
| Accurate tunnel placement |
| Easy suture shuttling through the ACL substance |
| Easy suture retrieval through the tunnels |
| Preservation of fracture fragment integrity |
| Securing of large, small, or even comminuted fragments |
| Separate AM and PL bundle stabilization |
| No loss of reduction during suture tying |
| Avoidance of iatrogenic growth plate disturbances in skeletally immature patients |
| Reduced operative time |
We acknowledge that our technique has only been used in a clinical setting. Further biomechanical studies to confirm the superiority of the 4-point fixation method are required, and inevitably, conclusions should be reviewed in light of the aforementioned limitations. We conclude that using the proposed technical modifications, 4-point anatomic and accurate reduction and superior fixation can be safely and reproducibly achieved, minimizing potential complications, as well as reducing operative times.
Acknowledgment
The authors thank Christina Eleftheriadou, graphic designer, for designing the professional-quality drawings.
Supplementary Data
Case of a 27-year-old female patient with a type III ACL avulsion fracture. The whole technique is described in detail.
References
- 1.LaFrance R.M., Giordano B., Goldblatt J., Voloshin I., Maloney M. Pediatric tibial eminence fractures: Evaluation and management. J Am Acad Orthop Surg. 2010;18:395–405. doi: 10.5435/00124635-201007000-00002. [DOI] [PubMed] [Google Scholar]
- 2.Meyers M.H., McKeever F.M. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1970;52:1677–1684. [PubMed] [Google Scholar]
- 3.Zaricznyj B. Avulsion fracture of the tibial eminence: Treatment by open reduction and pinning. J Bone Joint Surg Am. 1977;59:1111–1114. [PubMed] [Google Scholar]
- 4.Lubowitz J.H., Elson W.S., Guttmann D. Part II: Arthroscopic treatment of tibial plateau fractures: Intercondylar eminence avulsion fractures. Arthroscopy. 2005;21:86–92. doi: 10.1016/j.arthro.2004.09.031. [DOI] [PubMed] [Google Scholar]
- 5.Shelbourne K.D., Urch S.E., Freeman H. Outcomes after arthroscopic excision of the bony prominence in the treatment of tibial spine avulsion fractures. Arthroscopy. 2011;27:784–791. doi: 10.1016/j.arthro.2011.01.011. [DOI] [PubMed] [Google Scholar]
- 6.Koukoulias N.E., Germanou E., Lola D., Papavasiliou A.V., Papastergiou S.G. Clinical outcome of arthroscopic suture fixation for tibial eminence fractures in adults. Arthroscopy. 2012;28:1472–1480. doi: 10.1016/j.arthro.2012.03.014. [DOI] [PubMed] [Google Scholar]
- 7.Jang K.-M., Bae J.-H., Kim J.G., Wang J.H. Novel arthroscopic fixation method for anterior cruciate ligament tibial avulsion fracture with accompanying detachment of the anterior horn of the lateral meniscus: Three-point suture fixation. Injury. 2013;44:1028–1032. doi: 10.1016/j.injury.2012.12.008. [DOI] [PubMed] [Google Scholar]
- 8.White E.A., Patel D.B., Matcuk G.R. Cruciate ligament avulsion fractures: Anatomy, biomechanics, injury patterns, and approach to management. Emerg Radiol. 2013;20:429–440. doi: 10.1007/s10140-013-1121-0. [DOI] [PubMed] [Google Scholar]
- 9.Ezechieli M., Schafer M., Becher C. Biomechanical comparison of different fixation techniques for reconstruction of tibial avulsion fractures of the anterior cruciate ligament. Int Orthop. 2013;37:919–923. doi: 10.1007/s00264-013-1835-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lu X.-W., Hu X.-P., Jin C., Zhu T., Ding Y., Dai L.-Y. Reduction and fixation of the avulsion fracture of the tibial eminence using mini-open technique. Knee Surg Sports Traumatol Arthrosc. 2010;18:1476–1480. doi: 10.1007/s00167-010-1045-0. [DOI] [PubMed] [Google Scholar]
- 11.Pan R.-Y., Yang J.-J., Chang J.-H., Shen H.-C., Lin L.-C., Lian Y.-T. Clinical outcome of arthroscopic fixation of anterior tibial eminence avulsion fractures in skeletally mature patients: A comparison of suture and screw fixation technique. J Trauma Acute Care Surg. 2012;72:E88–E93. doi: 10.1097/TA.0b013e3182319d5a. [DOI] [PubMed] [Google Scholar]
- 12.Ahn J.H., Yoo J.C. Clinical outcome of arthroscopic reduction and suture for displaced acute and chronic tibial spine fractures. Knee Surg Sports Traumatol Arthrosc. 2005;13:116–121. doi: 10.1007/s00167-004-0540-6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Case of a 27-year-old female patient with a type III ACL avulsion fracture. The whole technique is described in detail.