

Abstract
The disadvantages of having orthodontic interventions both before and after orthognathic surgery include a long treatment time of 7–47 months and temporary worsening of facial appearance. Nowadays, the concept of surgery-first, followed by orthodontic treatment is applied to orthognathic surgery cases in different orthodontic centers in the world. This concept and technique is called “surgery-first-orthognathic-approach” or “surgery-first approach” (SFA) rigid fixation (skeletal anchorage system) of the bony segments and regional acceleratory phenomenon were keys to broad implementation of the SFA. This article is intended to provide an overview of SFA including indications, general and specific guidelines, different protocol variations, success rate and potential problems.
Keywords: Orthognathic surgery, skeletal anchorage system, surgery-first approach
INTRODUCTION
Presurgical orthodontic preparation was uncommon for patients requiring orthognathic surgery until the 1960's. The patients' and clinicians' desire for optimal esthetic and occlusal results led to the most common current treatment approach presurgical orthodontic decompensation of the occlusal relationships and attainment of normal dental alignment. The disadvantage of having orthodontic interventions both before and after orthognathic surgery include a long treatment time of 7–47 months, dental caries, gingival recession and root resorption.[1,2] Other complications associated with preoperative orthodontic treatment are temporary worsening of facial appearance and masticatory discomfort. When a patient refuses surgery after all the preparations have been made, the results can be catastrophic. Ever since the first orthognathic surgery procedure was performed by Hullihen in 1848, many new techniques and methods have been introduced.[3] As shown by Kondo and Aoba the limits of orthodontic treatment alone to severe malocclusions are broadening, but the underlying skeletal imbalances remain.[4,5] Brachvogel et al.[6] in 1991 proposed concept of “surgery-first and orthodontics second” with the goal of reducing some of the disadvantages and inconveniences of presurgical orthodontics. He claimed that the normalized surrounding soft tissues (lips, cheeks and tongue) settled teeth into better positions after surgery, facilitating remaining orthodontic tooth movement and reducing the total orthodontic treatment period.
Nowadays, the concept of surgery-first followed by orthodontic treatment is applied to orthognathic surgery cases in orthodontic centers in Korea, Japan and Taiwan. This concept and technique are called “surgery-first-orthognathic-approach” or “surgery-first approach” (SFA).
SURGERY-FIRST ORTHOGNATHICS
Rigid fixation of the bony segments was the key to broad implementation of the SFA. One such device is the skeletal anchorage system, which utilizes titanium miniplates to anchor orthodontic forces for three-dimensional movements in nongrowing patients.[7] A major driving motive for performing surgery-first orthognathics has been the reduced treatment time.[8,9,10] It has been shown that orthodontic treatment time decreases by using alveolar osteotomy procedures.[11,12] The proposed mechanism for this decrease in treatment time is the increase in cortical bone porosity that results in decreased resistance to tooth movement. It has been shown that during healing process after orthognathic surgery, there is an increase in blood flow above the presurgical levels which facilitates the healing process and stimulates bone turnover that can potentially speed up orthodontic tooth movement.[13,14] Treatment time as short as 7 months have been reported in the literature.[9] Bypassing presurgical orthodontics results in an overall shortened treatment time up to 1–1.5 years or less.[10]
Computer aided surgical simulation utilizing three-dimensional images obtained from multi-slice computed tomography/cone beam computer tomography has been successfully performed to plan craniofacial surgery.[15]
INDICATIONS
The criteria that are suggested for SFA[16] are:
Well-aligned to mild crowding
Flat to mild curve of Spee
Normal to mild proclination/retroclination of incisors
Minimal transverse discrepancy
This approach is also indicated in cases in which decompensation is needed.
Decompensation is done by positioning the jaw bones properly.
“Even though, the surgery-first technique can be applied to Class II as well as Class III malocclusions, the majority of cases treated using this approach have been cases with Class III malocclusion meeting the above criteria.”
GENERAL GUIDELINES OF SURGERY-FIRST APPROACH
The upper and lower dentitions are bonded and banded, but no arch wires are placed. Orthodontic arch wires are placed 1-week to 1-month postoperatively for the alignment, whereas the osteotomized jaw bones are held steadily by the rigid fixation
For the model surgery, the maxilla and mandible are set up in a proper molar relationship and with a positive overbite. The molar relationship could be set up in Class I in cases of nonextraction or bimaxillary first premolar extraction, Class III in cases of lower first premolar extraction, and Class II in cases of maxillary first premolar extraction. Once the molar relationship has been established, the overjet should also have been determined
The postsurgical orthodontic treatment could begin as early as 1-week to 1-month postoperatively by taking advantage of the phenomenon of postoperatively accelerated orthodontic tooth movement. Orthopedic appliances, such as a facemask or chin cap for Class III patients, could be applied for the maintenance of jaw bone position during the orthodontic tooth movement.
SPECIFIC GUIDELINES
Anteroposterior and Vertical Decompensation in Class III Cases
Incisors are positioned either surgically or orthodontically in proper inclination after surgery.
The anteroposterior decompensation for proclined maxillary incisors in a Class III case could be achieved by extraction of the maxillary first premolars and anterior segmental osteotomy or by clockwise rotation of the maxilla by Le Fort I osteotomy to upright the upper incisor inclination (preferred approach)
The anteroposterior decompensation for moderately retroclined and crowded lower incisors in a Class III case could be achieved by setting up the molars in a Class I relationship with an excessive incisor overjet, and then the lower incisors could be aligned postoperatively to obtain a normal overjet
The anteroposterior decompensation for severely retroclined and crowded lower incisors in a Class III case could be achieved by extraction of the lower first premolars and anterior segmental osteotomy, setting up the molars in a Class III molar relationship with an excessive incisor overjet, and then the lower incisors could be aligned postoperatively to obtain a normal overjet
A moderate to deep mandibular curve of Spee in a Class III case is better leveled either preoperatively or surgically by anterior segmental osteotomy to avoid the upward and forward rotation of the mandible postoperatively. A forward and upward rotation of the mandible improves the chin projection in the case of Class II mandibular retrognathism. However, it worsens the chin projection in the case of Class III mandibular prognathism. To avoid the upward and forward rotation of the mandible postoperatively, alternatively, the lower incisors could be intruded and the upper incisors at the same time could be extruded postoperatively.
Anteroposterior and Vertical Decompensation in Class II Cases
For a moderate to deep mandibular curve of Spee and proclined lower incisors in Class II mandibular retrognathism, the anterior segment of the mandible could be levelled and intruded surgically through anterior segmental osteotomy so that the mandible could be advanced properly
Alternatively, the mandible could be surgically advanced to an edge-to-edge incisor relationship and without occlusal contact in the posterior teeth, and then postoperatively, the mandibular anterior teeth could be orthodontically intruded and hence that the mandible rotates upward and forward for posterior occlusal contact and a better chin projection.
Transverse Arch Co-ordination
The intercanine and intermolar widths of the upper and lower dentitions are co-ordinated either by surgery or postoperative orthodontic tooth movement.
For a wide maxilla with a transverse discrepancy more than a molar width on each side could be coordinated surgically by a three-piece Le Fort I osteotomy of the maxilla
For a wide maxilla with a transverse discrepancy less than a molar width on each side could be co-ordinated by postoperative orthodontic tooth movement. This can be done by setting up the buccal slope of the palatal cusps of the maxillary molars occluding on the lingual slope of the buccal cusps of the mandibular molars on both sides. The excessive buccal overjet would be solved postoperatively by the occlusal force or vertical chin cap or orthodontically by constricted transpalatal arch in a short period of time
For a narrow maxilla, surgically assisted rapid palatal expansion could be the treatment of choice.
REDUCED TREATMENT TIME IN SURGERY-FIRST APPROACH: REGIONAL ACCELERATORY PHENOMENON
The regional acceleratory phenomenon was well described by Frost in 1993. After an osteotomy, bone remodeling around the healing tissue facilitates the healing process.[17] Alkaline phosphatase (ALP) and C-terminal telopeptide of type I collagen (ICTP) are two bone markers which have been studied using 22 patients of SFA. The former is associated with osteoblastic activity while the latter is a by-product of osteoclastic breakdown of bone. The results of such study show that orthognathic surgery triggers 3–4 months of higher osteoclastic activities and metabolic changes in the dentoalveolus.[10]
The postoperative transient increase in ICTP and ALP indicates a transient burst of bone remodeling and turnover activities after orthognathic surgery.
TREATMENT PLANNING CONSIDERATIONS
The molar relationship can be utilized as a starting point to come up with a temporary occlusion
The inclination of upper incisors is important in determining the need for possible extractions. If the upper incisor to occlusal plane angulation is <53-55°, extraction must be considered.[7] Another possibility involves changing the position of the whole maxilla, so that the occlusal plane become steeper and producing more upright maxillary incisors. One might distalize the maxillary posterior segments using zygomatic plates as shown by Nagasaka et al.[18] and Villegas et al.[9] thus opening the space to retract maxillary incisors
The midlines must be coincident or close to it after surgery, and proper buccal overjet must be established bilaterally
Most challenging and time consuming step is the prediction of the final occlusion based on the current position of teeth. The term intended transitional malocclusion is used to describe the occlusion that is used to fabricate the surgical splint and surgeon's guide during surgery.[19] At least a three-point contact must be established between the upper and lower models when deciding ITM. In cases where such temporary occlusion cannot be established, it is advisable to initiate some orthodontic movement in order to relieve some of the interferences.
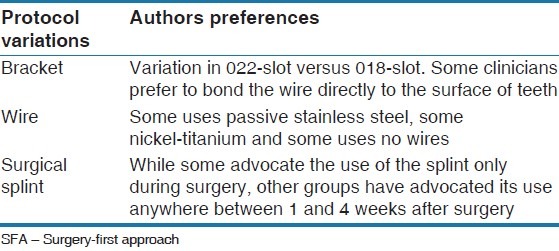
PROTOCOL VARIATIONS
In most cases, there are variations among authors regarding use of bracket types, wires and surgical splint [Table 1]. It is advisable to wait for about 4–6 weeks for teeth movement after surgery for better stability.
Table 1.
Different protocol variations in SFA
USE OF SKELETAL ANCHORAGE IN CONJUNCTION WITH SURGERY-FIRST APPROACH
The SFA requires meticulous treatment planning and collaboration between the orthodontist and the orthognathic surgeon. Many uncertainties remain at the time, patient is sent to surgery. By utilizing the temporary anchorage devices, many orthodontists try to have a “back-up” system, which can be used to help in postsurgical orthodontic phase. These devices are anywhere from single mini-implants to titanium plates which can be placed at the time of surgery.[18,20,21]
The use of temporary anchorage devices becomes more crucial in more complicated cases that are attempted with the SFA. When extractions or segmented osteotomies are planned, prediction of the final occlusion is far more challenging, and placement of mini-implants during the surgery allows for efficient mechanics postsurgically.
POTENTIAL PROBLEMS
Apart from certain advantages, some potential problems associated with SFA are the following:
Predicting the final occlusion is the hardest challenge with SFA due to multiple dental interferences
Cases requiring extractions are especially very difficult to plan when performing surgery-first
Any minor surgical error can compromise the final occlusion
The planning process is very time consuming in contrast to the total treatment time
The increase in the number and complexity of osteotomy procedures poses a greater risk to the patient.
STABILITY AFTER SURGERY-FIRST APPROACH
There are various studies done to compare stability of SFA with a conventional technique and found no significant difference.[7,22,23] Comparison for transverse changes has also been made, and no significant difference is found with and without presurgical orthodontics.[24]
Recently, study was carried out to identify parameters for instability in SFA and concluded that factors for instability are large overjet, a deeper curve of Spee, a greater negative overjet and greater mandibular setback.[25]
CONCLUSION
Even if SFA for correcting skeletal malocclusions has the advantages of shortened total treatment time and early response to a patient's need, there are limitations particularly relating to careful case selection, adequate diagnosis, prediction and simulating correction with the model setup is required. Experience of surgeon and orthodontist are important factors in applying the appropriate treatment method taking account of patient's need and goals.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Luther F, Morris DO, Hart C. Orthodontic preparation for orthognathic surgery: How long does it take and why. A retrospective study? Br J Oral Maxillofac Surg. 2003;41:401–6. doi: 10.1016/s0266-4356(03)00163-3. [DOI] [PubMed] [Google Scholar]
- 2.O'Brien K, Wright J, Conboy F, Appelbe P, Bearn D, Caldwell S, et al. Prospective, multi-center study of the effectiveness of orthodontic/orthognathic surgery care in the United Kingdom. Am J Orthod Dentofacial Orthop. 2009;135:709–14. doi: 10.1016/j.ajodo.2007.10.043. [DOI] [PubMed] [Google Scholar]
- 3.Hullihen S, Aziz S. The origin of orthognathic surgery. J Oral Maxillofac Surg. 2004;62:1303–7. doi: 10.1016/j.joms.2003.08.044. [DOI] [PubMed] [Google Scholar]
- 4.Kondo E, Aoba TJ. Nonsurgical and nonextraction treatment of skeletal class III open bite: Its long-term stability. Am J Orthod Dentofacial Orthop. 2000;117:267–87. doi: 10.1016/s0889-5406(00)70232-0. [DOI] [PubMed] [Google Scholar]
- 5.Kondo E, Arai S. Nonsurgical and nonextraction treatment of a skeletal class III adult patient with severe prognathic mandible. World J Orthod. 2005;6:233–47. [PubMed] [Google Scholar]
- 6.Brachvogel P, Berten JL, Hausamen JE. Surgery before orthodontic treatment: A concept for timing the combined therapy of skeletal dysgnathias. Dtsch Zahn Mund Kieferheilkd Zentralbl. 1991;79:557–63. [PubMed] [Google Scholar]
- 7.Liao YF, Chiu YT, Huang CS, Ko EW, Chen YR. Presurgical orthodontics versus no presurgical orthodontics: Treatment outcome of surgical-orthodontic correction for skeletal class III open bite. Plast Reconstr Surg. 2010;126:2074–83. doi: 10.1097/PRS.0b013e3181f52710. [DOI] [PubMed] [Google Scholar]
- 8.Yu CC, Chen PH, Liou EJ, Huang CS, Chen YR. A Surgery-first approach in surgical-orthodontic treatment of mandibular prognathism - A case report. Chang Gung Med J. 2010;33:699–705. [PubMed] [Google Scholar]
- 9.Villegas C, Uribe F, Sugawara J, Nanda R. Expedited correction of significant dentofacial asymmetry using a “surgery first” approach. J Clin Orthod. 2010;44:97–103. [PubMed] [Google Scholar]
- 10.Liou EJ, Chen PH, Wang YC, Yu CC, Huang CS, Chen YR. Surgery-first accelerated orthognathic surgery: Postoperative rapid orthodontic tooth movement. J Oral Maxillofac Surg. 2011;69:781–5. doi: 10.1016/j.joms.2010.10.035. [DOI] [PubMed] [Google Scholar]
- 11.Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: Two case reports of decrowding. Int J Periodontics Restorative Dent. 2001;21:9–19. [PubMed] [Google Scholar]
- 12.Wilcko MT, Wilcko WM, Pulver JJ, Bissada NF, Bouquot JE. Accelerated osteogenic orthodontics technique: A 1-stage surgically facilitated rapid orthodontic technique with alveolar augmentation. J Oral Maxillofac Surg. 2009;67:2149–59. doi: 10.1016/j.joms.2009.04.095. [DOI] [PubMed] [Google Scholar]
- 13.Justus T, Chang BL, Bloomquist D, Ramsay DS. Human gingival and pulpal blood flow during healing after Le Fort I osteotomy. J Oral Maxillofac Surg. 2001;59:2–7. doi: 10.1053/joms.2001.19251. [DOI] [PubMed] [Google Scholar]
- 14.Iliopoulos Ch, Zouloumis L, Lazaridou M. Physiology of bone turnover and its application in contemporary maxillofacial surgery. A review. Hippokratia. 2010;14:244–8. [PMC free article] [PubMed] [Google Scholar]
- 15.Hsu S, Singhal D, Xia J, Gateno J, Lin CH, Huang CS, et al. Planning the surgery-first approach in surgical-orthodontic treatment with a computer aided surgical simulation (CASS) planning protocol. J Taiwan Assoc Orthod. 2012;24:24–37. [Google Scholar]
- 16.Liou EJ, Chen PH, Wang YC, Yu CC, Huang CS, Chen YR. Surgery-first accelerated orthognathic surgery: Orthodontic guidelines and setup for model surgery. J Oral Maxillofac Surg. 2011;69:771–80. doi: 10.1016/j.joms.2010.11.011. [DOI] [PubMed] [Google Scholar]
- 17.Frost HM. The regional acceleratory phenomenon: A review. Henry Ford Hosp Med J. 1983;31:3–9. [PubMed] [Google Scholar]
- 18.Nagasaka H, Sugawara J, Kawamura H, Nanda R. "Surgery first" skeletal class III correction using the Skeletal Anchorage System. J Clin Orthod. 2009;43:97–105. [PubMed] [Google Scholar]
- 19.Park KR, Kim SY, Park HS, Jung YS. Surgery-first approach on patients with temporomandibular joint disease by intraoral vertical ramus osteotomy. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116:e429–36. doi: 10.1016/j.oooo.2011.11.038. [DOI] [PubMed] [Google Scholar]
- 20.Sugawara J, Nishimura M. Minibone plates: The skeletal anchorage system. Semin Orthod. 2005;11:47–56. [Google Scholar]
- 21.Sugawara J. A bioefficient skeletal anchorage system. In: Nanda R, editor. Biomechanics and Esthetic Strategies in Clinical Orthodontics. St. Louis: Elsevier Saunders; 2005. pp. 295–309. [Google Scholar]
- 22.Choi JW, Lee JY, Yang SJ, Koh KS. The reliability of a surgery-first orthognathic approach without presurgical orthodontictreatment for skeletal class III dentofacial deformity. J Craniofac Surg. 2010;21:332–8. doi: 10.1097/SAP.0b013e318295dcce. [DOI] [PubMed] [Google Scholar]
- 23.Baek SH, Ahn HW, Kwon YH, Choi JY. Surgery-first approach in skeletal class III malocclusion treated with 2-jaw surgery: Evaluation of surgical movement and postoperative orthodontic treatment. J Craniofac Surg. 2010;21:332–8. doi: 10.1097/SCS.0b013e3181cf5fd4. [DOI] [PubMed] [Google Scholar]
- 24.Wang YC, Ko EW, Huang CS, Chen YR, Takano-Yamamoto T. Comparison of transverse dimensional changes in surgical skeletal class III patients with and without presurgical orthodontics. J Oral Maxillofac Surg. 2010;68:1807–12. doi: 10.1016/j.joms.2009.09.089. [DOI] [PubMed] [Google Scholar]
- 25.Ko EW, Hsu SS, Hsieh HY, Wang YC, Huang CS, Chen YR. Comparison of progressive cephalometric changes and postsurgical stability of skeletal class III correction with and without presurgical orthodontic treatment. J Oral Maxillofac Surg. 2011;69:1469–77. doi: 10.1016/j.joms.2010.07.022. [DOI] [PubMed] [Google Scholar]