

Abstract
Background:
Atherosclerotic disease is the most important cause of mortality in the world. Oxidation is an important pathway in the pathogenesis of coronary artery disease (CAD) through oxidation of low-density lipoprotein (LDL) and free radical formation. Copper (Cu) is an essential micronutrient for enzymes that catalyse LDL oxidation reactions. Therefore, an evaluation of Cu in the atherosclerotic disease is important.
Materials and Methods:
In this study, 334 subjects without recent cardiac event and history of collagen vascular or infectious disease were investigated. All patients divided into four groups to evaluate severity of CAD according to Syntax scoring system. All groups were matched in cardiovascular risk factors.
Results:
The serum level of Cu was significantly higher in total atherosclerotic groups than normal group (P value = 0.001) and significantly increased with severity of atherosclerosis.
Conclusion:
The finding indicated that the serum level of Cu is higher in atherosclerotic patients and it increases with severity of atherosclerosis. Therefore, it may be possible that the basic relationship exist between serum Cu level and atherosclerosis and an association between Cu level and severity of atherosclerosis.
Keywords: Atherosclerotic disease, copper, syntax score
INTRODUCTION
Atherosclerotic disease of the coronary arteries is one of the most common causes of mortality and morbidity. Despite all the methods of diagnosis and the new strategies in the treatment of patients, cardiovascular diseases (CVDs) are considered as the most important cause of mortality in Iran over the last decade.1 A number of known risk factors have been recognised for this disease, but less known factors such as trace elements may have a role in the progress of atherosclerosis.2 The serum level of copper (Cu) and oxidants like free radicals have also been considered in coronary artery disease (CAD).3,4
Several studies show that atherosclerosis is characterised with fatty fibrous plaques, localised in intima. Endothelial damage is the most important factor in the atherosclerotic process.5 The main effect of these factors on the endothelium is oxidative stress, lipid peroxidation and the formation of free radicals. Eventually, the structure of the endothelium is damaged. The essential element Cu acts as micro sources in biochemical reactions. Cu and CVD may be associated directly, through a direct effect on the vascular endothelium, or indirectly through lipoprotein metabolism. Copper ions can convert the superoxide and the hydrogen peroxide into the highly harmful hydroxyl radical that can damage to endothelium.6
The aim of this study is investigation about relationship between serum levels of Cu and the severity of atherosclerosis measured by Syntax score.
MATERIALS AND METHODS
This is a cross-sectional study conducted on patients hospitalised in Sari Heart Centre, Mazandaran University of Medical Sciences from February 2010 to July 2012. Written informed consent was obtained from all enrollees, according to the criteria of the Ethical Committee of Mazandaran University of Medical Sciences.
The sample consisted in 337 patients with chronic stable angina that each of them had been admitted for diagnostic coronary angiography into typical indications, such as evaluation of stable exertional angina.
The patients who had history of infectious disease in recent 2 months, collagen vascular disease and recent cardiac events were ineligible.
Coronary angiography was performed by the Judkins technique through femoral artery access and the angiograms evaluated by two cardiologists who were blinded to the study plan.
All patients divided into four groups to evaluate severity of CAD according to Syntax scoring system.
The diagnosis of CAD was based on the presence of 50% luminal diameter stenosis of the major epicardial coronary artery which determined in a standard manner during the coronary angiograms. The percent diameter stenosis is not considered in the algorithm. Distinction has been made only between occlusive (100% diameter stenosis) and non-occlusive (50-99% diameter stenosis) disease. A multiplication factor of 2 is used for non-occlusive lesions and 5 for occlusive lesions. CAD was categorised to mild for scores 1-22, moderate for 23-32 and severe for scores 33and higher.7,8
Cardiovascular risk factors including age, sex, systolic and diastolic blood pressure, smoking status, history of dyslipidaemia, diabetes, etc. were assessed for each subject.
Dyslipidaemia was defined as total cholesterol (TC) to high-density lipoprotein (HDL) more than 4. Hypertension (HT) is defined as a systolic blood pressure above 140 mmHg, or diastolic blood pressure above 90 mmHg, respectively, or current use of antihypertensive medication. Diabetes mellitus (DM) is defined as a known history of DM (fasting blood glucose 126 mg/dl or glucose tolerance test (GTT) higher than 200 mg/dl or treatment with insulin or oral hypoglycaemic agents. Different categories of cigarette smoking status are defined according to world health organisation (WHO) guidelines.9 Daily smoker is defined as who smokes cigarettes at least once a day; occasional smoker is who smokes cigarettes but not every day; ex-smoker is formerly daily or occasional smoker who currently does not smoke and never smoked defined as who never smoked before or smoked too little in the past.
Blood samples were collected after 14-hours fasting for measurement of total cholesterol, HDL- cholesterol, glucose immediately before the coronary angiography was started. The samples were centrifuged at 3,000 g for 10 min at ambient temperature. The serum obtained was separated and frozen at −80°C until the time of analysis. Cu levels were assayed by flame atomic absorption spectrophotometer on an A100 variant. Then, the concentrations were determined following preparation of calibration curves and evaluation of line equation.
Statistical analyses
Data were analysed using the Statistical Package for the Social Sciences (SPSS)-16 software. Baseline demographic and laboratory data are presented for continuous variables as mean ± SD and discrete variables as frequencies. Parametric and non-parametric data analysed with t-test and chi-square between normal and total atherosclerotic groups. The mean difference of Cu level between four groups was analysed using a one-way analysis of variance (ANOVA). P < 0.05 was considered statistically significant.
RESULTS
Comparison of demographic data between groups
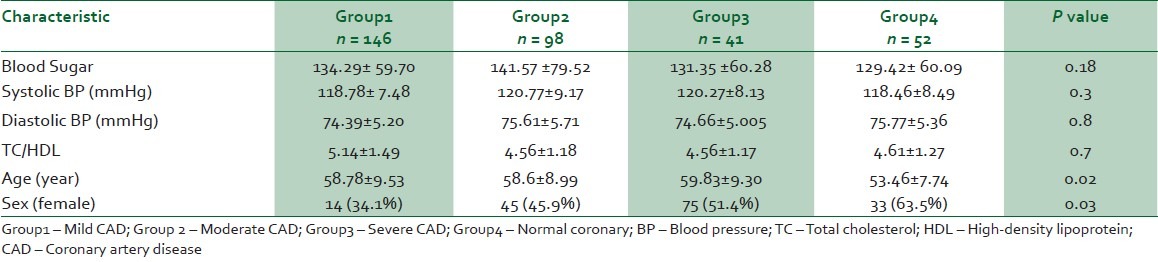
Table 1 summarises the demographic data for subjects. There was no significant difference in smoking habits, occurrence of DM and HT, serum TC/HDL and blood glucose levels between four groups.
Table 1.
Demographic data for subjects
Blood cu level in all groups
The main results are summarised in Table 2. The serum level of Cu in normal coronary group was significantly lower than the total atherosclerotic groups (P value = 0.001). The serum level of Cu was significantly increased with severity of atherosclerosis and significantly upper in sever atherosclerotic patients (33 Syntax scores and above it) than mild and moderate CAD groups. (P value = 0.001).
Table 2.
The serum level of Cu in four groups

Therefore, there were significant differences in serum level of Cu between normal coronary group and atherosclerotic patients and between CAD groups.
DISCUSSION
CAD has been associated with several risk factors including sex, age, dyslipidaemia, diabetes mellitus, cigarette smoking and hypertension.10
Oxidation is an important pathway in the pathogenesis of CAD through oxidation of low-density lipoprotein (LDL) and free radical formation11,12 and Cu is essential micronutrient for enzymes that catalyse oxidation–reduction reactions.12
In this study, higher serum level of copper in patients with atherosclerosis compare of the normal group was detected. On the other hand, the serum level of Cu increased dependent to degree of atherosclerosis. These findings suggest that high level of this element may play a role in atherosclerotic process.
Various studies have shown the results consistent of present research. Nourmohammadi et al. investigated that serum Cu level were significantly upper in patients with CAD than in healthy subjects.13 Shokrzadeh et al. determined the levels of Cu in 30 patients with ischemic cardiomyopathy diagnosed with coronary angiography. They found higher serum Cu levels in the patient groups than in the healthy subjects.14 In a study performed in patients with acute coronary syndrome by Altekin et al., there was the positive correlation between serum Cu levels with elevated troponin T, troponin I and CK-MB values (≥0.9, ≥1.0 and ≥30 ng/ml, respectively).15 The same results were declared by Cikim et al. in patients with acute coronary syndrome.16 Neither of these studies included stable coronary artery disease. Our study was performed in patients with stable angina and we found that serum level of copper is higher in CAD patients than normal group. The relationship between serum Cu levels and CAD is controversial in some studies.17,18 Alissa et al. proposed that serum Cu level had not significant difference in CAD group and healthy subjects6 but in his study, case and control groups were not completely matched.
In the present study, all groups were matched in regards of cardiovascular risk factors and we found that higher serum Cu level is an important CAD risk factor.
CONCLUSION
This study showed that, there is basic relationship between serum Cu level and atherosclerosis, and revealed an association between Cu level and the severity of atherosclerosis. Larger prospective cohort studies are needed to confirm our observations, and experimental data may further elucidate the biological mechanisms of the associations.
ACKNOWLEDGMENT
We would like to thank the Mazandaran University of Medical Sciences for founding this investigation. The code of research proposal is 1424.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Aghaeishahsavari M, Noroozianavval M, Veisi P, Parizad R, Samadikhah J. Cardiovascular disease risk factors in patients with confirmed cardiovascular disease. Saudi Med J. 2006;27:1358–61. [PubMed] [Google Scholar]
- 2.Vyas RK, Gupta AP, Gupta A, Aeron AK. Serum copper, zinc, magnesium and calcium levels in various human disease. Indian J Med Res. 1982;76:301–4. [PubMed] [Google Scholar]
- 3.Ridker PM, editor. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. Philadelphia: W.B. Saunders; 2005. Risk Factors for Atherothrombotic Disease. [Google Scholar]
- 4.Russel RO, Robert SR, Wayne AL, editors. Factors Influencing Atherogenesis: Hurst's, the Heart, A Textbook of Cardiovascular Disease. Volume: 1. New York: McGraw-Hill; 2001. [Google Scholar]
- 5.Cikim G. Investigation of new risk factors and dyslipidemies in patients with coronary heart disease [Medical Residency thesis] Turkey: College of Medicine, Firat University, Elazig; 2002. [Google Scholar]
- 6.Alissa EM, Bahjri SM, Ahmed WH, Al-Ama N, Ferns GA. Trace element status in Saudi patients with established atherosclerosis. J Trace Elem Med Biol. 2006;20:105–14. doi: 10.1016/j.jtemb.2005.10.004. [DOI] [PubMed] [Google Scholar]
- 7.Pearson TA. Coronary angiography in the study of the epidemiology of coronary artery disease. Epidemiol Rev. 1984;6:140–66. doi: 10.1093/oxfordjournals.epirev.a036269. [DOI] [PubMed] [Google Scholar]
- 8.Sianose G, Morel MA, Kappetein AP, Morice MC, Colombo A, Dawkins K, et al. The SYNTAX Score: An angiographic tool grading the complexity of coronary artery disease. EuroIntervention. 2005;1:219–27. [PubMed] [Google Scholar]
- 9.World Health Organization, Guideline for controlling and monitoring the Tobacco Epidemic. Geneva: 1998. [at: 06/06/2014]. Available in: http://apps.who.int/bookorders/anglais/detart1.jsp?sesslan=1&codlan=1&codcol=15&codcch=468 . [Google Scholar]
- 10.Kagan A, Kannel WB, Dawber TR. The coronary profile. Ann N Acad Sci. 1963;97:883–94. doi: 10.1111/j.1749-6632.1962.tb56002.x. [DOI] [PubMed] [Google Scholar]
- 11.Steinberg D, Parthasarathy S, Carew TE, Khoo JC, Witztum JL. Beyond cholesterol. Modifications of low-density lipoprotein that increase its atherogenicity. N Engl J Med. 1989;320:915–24. doi: 10.1056/NEJM198904063201407. [DOI] [PubMed] [Google Scholar]
- 12.Linder MC, Hazegh-Azam M. Copper biochemistry and molecular biology. Am J Clin Nutr. 1996;63:797–811S. doi: 10.1093/ajcn/63.5.797. [DOI] [PubMed] [Google Scholar]
- 13.Nourmohammadi I, et al. Serum levels of Zn,Cu,Cr and Ni in Iranian Subjects with Atherosclerosis, in Arch Irn Med. 2001;4:21–4. [Google Scholar]
- 14.Shokrzadeh M, Ghaemian A, Salehifar E, Aliakbari S, Saravi SS, Ebrahimi P, et al. Serum zinc and copper levels in ischemic cardiomyopathy. Biol Trace Elem Res. 2009;127:116–23. doi: 10.1007/s12011-008-8237-1. [DOI] [PubMed] [Google Scholar]
- 15.Altekin E, Coker C, Sisman AR, Onvural B, Kuralay F, Kirimli O. The relationship between trace elements and cardiac markers in acute coronary syndromes. J Trace Elem Med Biol. 2005;18:235–42. doi: 10.1016/j.jtemb.2004.12.002. [DOI] [PubMed] [Google Scholar]
- 16.Cikim G, Canatan H, Gursu MF, Gulcu F, Baydas G, Kilicoglu AE. Levels of zinc and lipid peroxidation in acute coronary syndrome. Biol Trace Elem Res. 2003;96:61–9. doi: 10.1385/BTER:96:1-3:61. [DOI] [PubMed] [Google Scholar]
- 17.Ford ES. Serum copper concentration and coronary heart disease among US adults. Am J Epidemiol. 2000;151:1182–8. doi: 10.1093/oxfordjournals.aje.a010168. [DOI] [PubMed] [Google Scholar]
- 18.Salonen JT, Salonen R, Korpela H. Serum copper and the risk of acute myocardial infarction: A prospective population study in men in eastern Finland. Am J Epidemiol. 1991;134:268–76. doi: 10.1093/oxfordjournals.aje.a116080. [DOI] [PubMed] [Google Scholar]