

Sir,
The term “isotopic response” describes the occurrence of a new unrelated skin disorder at the site of another, already healed skin disease. The proposed etiologies of isotopic response are viral, immunological, neural, vascular and locus minoris resistentiae (a site of lessened resistance). Most cases of isotopic response have been described in healed lesions (scars) of herpes zoster (HZ). Granuloma annulare, lichen planus, granulomatous folliculitis, tinea, multiple epidermoid cysts, morphea, rosacea, erythema annulare cetrifugum, Kaposi's sarcoma, leukemia cutis, metastasis, acne, verrucae plana, molluscum contagiosum, squamous cell carcinoma, basal cell carcinoma and sarcoidosis have been reported as second disease as part of an isotopic response.[1,2]
Herein we report a 65-year-old female who developed discoid lupus erythematosis (DLE) as a second disease on a HZ scar over the gluteal region. She was a known diabetic on oral hypoglycemic agents and presented with an occasionally itchy skin lesion over the gluteal area since approximately four months duration. She gave a past history of intramuscular injection and HZ over the same site five years ago. A general practitioner had administered an injection for preherpetic pain and the puncture site took a long time to heal. On examination, she had an irregular pigmented, thick plaque over the left gluteal region with areas of depigmentation, erosion, and adherent scale. A similar but smaller pigmented plaque with an adherent scale was seen above the large plaque. A small pigmented scar was present on the left side close to the midline [Figures 1 and 2]. The skin over the gluteal region was wrinkled and xerotic with minimal scaling. Histopathology was consistent with DLE [Figure 3]. Her hemogram was normal except for a low hemoglobin level and she was negative for antinuclear antibody. Her blood sugar was raised; urine was positive for sugar, but negative for albumin and deposits. She was treated with a topical corticosteroid and zinc along with oral antihistamines and antioxidants.
Figure 1.

Discoid lupus erythematosis plaque over scar of herpes zoster - posterolateral view
Figure 2.

Discoid lupus erythematosis plaque over scar of herpes zoster - posterior view
Figure 3.
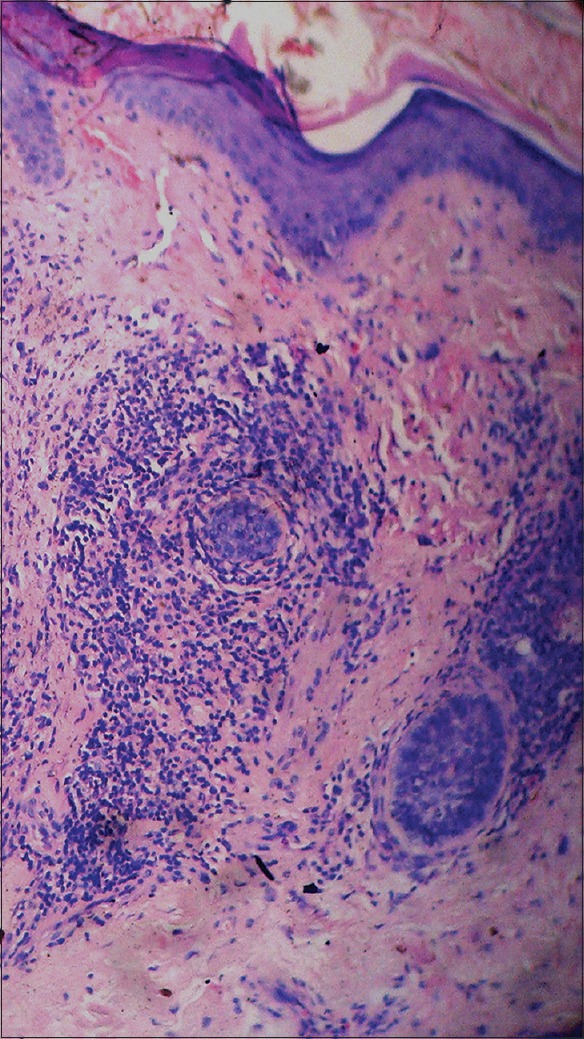
Histology showing hyperkeratosis, follicular plugging, epidermal atrophy, basal cell degeneration and perifollicular infiltrate around destroyed follicular structures. H and E, ×100
Discoid lupus erythematosis likely occurs in genetically predisposed individuals, but the exact genetic connection has not been determined. It has been suggested that a heat-shock protein (HSP) is induced in the keratinocyte, which can act as a target for T-cell-mediated epidermal cell cytotoxicity. In addition, toll-like receptors (TLR) may be involved in the pathogenesis.[3] Emerging evidences suggest the role of HSP47 and TLR4 in the pathogenesis of pathogenesis of scar tissue formation.[4,5] It has been hypothesized that the virus could alter the skin immune system locally inducing hyperreactivity towards tissue antigens. Injury to cutaneous nerve fibers, may alter the secretion of neuropeptides, impairing the immune response. Whether the occurrence of DLE over the HZ scar was because of alteration in the local skin immunity due to herpes virus infection or local injection could not be delineated. The role of HSP and the TLR in preparing a bed for a second lesion to appear over scar tissues needs further elucidation. DLE occurs predominantly over the sun exposed areas. To the best of the author's knowledge, DLE occurring as an isotopic response over a HZ scar has so far not been reported.
REFERENCES
- 1.Kaliyadan F, Gopinath S, Jayasree MG, Parmar C. Isomorphic and isotopic phenomenon occurring simultaneously in a case of granuloma annulare. Indian J Dermatol Venereol Leprol. 2009;75:307–9. doi: 10.4103/0378-6323.51270. [DOI] [PubMed] [Google Scholar]
- 2.Thappa D. Isotopic response versus isomorphic response. Indian J Dermatol Venereol Leprol. 2004;70:376. [PubMed] [Google Scholar]
- 3.Lehmann P, Hölzle E, Kind P, Goerz G, Plewig G. Experimental reproduction of skin lesions in lupus erythematosus by UVA and UVB radiation. J Am Acad Dermatol. 1990;22 2 Pt 1:181–7. doi: 10.1016/0190-9622(90)70020-i. [DOI] [PubMed] [Google Scholar]
- 4.Wang Z, Inokuchi T, Nemoto TK, Uehara M, Baba TT. Antisense oligonucleotide against collagen-specific molecular chaperone 47-kDa heat shock protein suppresses scar formation in rat wounds. Plast Reconstr Surg. 2003;111:1980–7. doi: 10.1097/01.PRS.0000054844.41243.F2. [DOI] [PubMed] [Google Scholar]
- 5.Wang J, Hori K, Ding J, Huang Y, Kwan P, Ladak A, et al. Toll-like receptors expressed by dermal fibroblasts contribute to hypertrophic scarring. J Cell Physiol. 2011;226:1265–73. doi: 10.1002/jcp.22454. [DOI] [PubMed] [Google Scholar]