

Abstract
Objective. To implement the flipped teaching method in a 3-class pilot on cardiac arrhythmias and to assess the impact of the intervention on academic performance and student perceptions.
Design. An intervention group of 101 first-year pharmacy students, who took the class with the flipped teaching method, were supplied with prerecorded lectures prior to their 3 classes (1 class in each of the following subjects: basic sciences, pharmacology, and therapeutics) on cardiac arrhythmias. Class time was focused on active-learning and case-based exercises. Students then took a final examination that included questions on cardiac arrhythmias. The examination scores of the intervention group were compared to scores of the Spring 2011 control group of 105 first-year students who took the class with traditional teaching methods. An online survey was conducted to assess student feedback from the intervention group.
Assessment. The mean examination scores of the intervention group were significantly higher than the mean examination scores of the control group for the cardiac arrhythmia classes in pharmacology (with 89.6 ± 2.0% vs 56.8 ± 2.2%, respectively) and therapeutics (89.2 ± 1.4% vs 73.7 ± 2.1%, respectively). The survey indicated higher student satisfaction for flipped classes with highly rated learning objectives, recordings, and in-class activities.
Conclusion. Use of the flipped teaching method in a 3-class pilot on cardiac arrhythmias improved examination scores for 2 of the 3 classes (pharmacology and therapeutics). Student satisfaction was influenced by the quality of the learning objectives, prerecorded lectures, and inclass active-learning activities.
Keywords: flipped classroom, inverted classroom, active learning, teaching methods, pharmacy education
INTRODUCTION
Since the introduction of the term “flipped classroom” in 2007, the flipped teaching model has been rapidly gaining popularity in kindergarten through twelfth grades and undergraduate education nationwide.1 Its popularity and growth have been fueled by developments in digital media, software, and increased access to the Internet.2 As such, the new generation of pharmacy students will likely expect use of multimedia and flipped classrooms. As learners coming of age at the turn of the millennium have been defined by technology and social media,3 colleges and schools of pharmacy will need to update their curricula to match modern learning and media preferences in order to keep students stimulated and engaged.
Traditional teaching methods have relied heavily on professors disseminating information through lectures, and students passively absorbing material for a majority of the class period. Limitations of traditional teaching are recognized and call for curricular change voiced in schools of medicine, pharmacy, and other medical professional schools.4-7 Additionally, as the profession of pharmacy is becoming more clinical and patient-centered, the Accreditation Council for Pharmacy Education Accreditation Guidelines and the Center for Advancement of Pharmacy Education Educational Outcomes have become increasingly focused on teaching methods that increase communication, critical-thinking, problem-solving, and self-learning skills.8,9 In the flipped classroom, lectures, traditionally given in class, are offered in various forms (eg, multimedia recordings, online tutorials, etc) outside of the classroom to be completed prior to class, and class time is dedicated to application and discussion of lecture materials through active-learning exercises that utilize higher order cognitive skills.
At Touro University California College of Pharmacy (TUCOP), active learning has become an integral part of the pharmacy curriculum in order to expand these skills now required of today’s pharmacy professionals. In a typical 3-hour class period, Touro University pharmacy students spend roughly 2 hours listening to lecture and 1 hour in small group discussion sections in which students discuss case-based problems, prepare and give presentations, and perform other exercises. To further enhance and use the full class period for active learning, the flipped teaching method was piloted in the spring of 2012 for first-year pharmacy students on the topic of cardiac arrhythmias, a historically challenging topic for students.
The TUCOP didactic curriculum follows a semester system in which students are enrolled in 4 content-based courses: basic sciences (5 units), pharmacology (6 units), therapeutics (5 units), and social and administrative sciences (3 units). Organ systems and the associated diseases/therapeutic topics are covered in blocks, with each course covering content related to its title. The topic of cardiac arrhythmias, for example, was taught during the cardiology block of the first-year spring semester, with 1 class period in each relevant course: the basic sciences period covers basic pathophysiology and identification of cardiac arrhythmias on electrocardiograms; the pharmacology period covers the pharmacology of anti-arrhythmia drugs; and the therapeutics period covers the pharmacotherapy of cardiac arrhythmias (social and administrative sciences in not involved with this disease state). Thus, the flipped teaching pilot was implemented as 3 classes, 1 in each course, basic sciences, pharmacology, and therapeutics, over the course of 1 week.
The purpose of the study was to assess the effectiveness of the flipped teaching method on academic performance by comparing the examination scores of students in the flipped teaching setting to examination scores of students in the traditional teaching setting and to assess the perceived value of the flipped teaching method by analyzing student feedback.
DESIGN
In the spring of 2012, the entire class of first-year pharmacy students (n=101) enrolled at TUCOP was selected to participate in a flipped 3-class pilot on the topic of cardiac arrhythmias. The 3 classes, taught by 3 different professors covered basic sciences, pharmacology, and therapeutics of arrhythmias, respectively. Lectures were prerecorded using voice-over PowerPoint for the basic sciences course and WebEx videoconferencing software with audio and video (Cisco Systems, Inc., San Jose, CA) for the pharmacology and therapeutics courses. The length of the lecture recording was 90 minutes for basic sciences, 130 minutes for pharmacology and 80 minutes for therapeutics. Recordings were posted to the Blackboard (Blackboard Inc., Washington, D.C.) course webpage along with learning objectives, lecture slides, and reading materials at least 4 days prior to the class session with the expectation that students review materials beforehand. To encourage preclass preparation, announced quizzes were given at the beginning of each class.
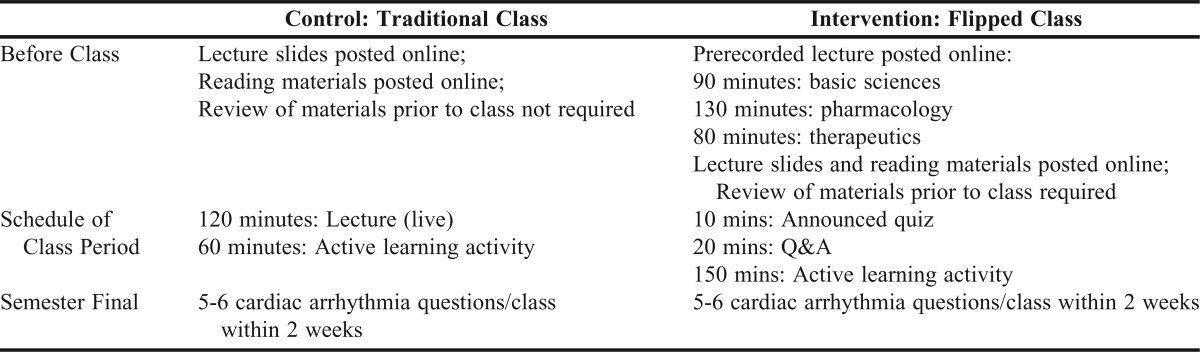
These short, multiple-choice quizzes assessed basic understanding and were followed by a 20-minute question-and-answer session for clarification of lecture material. The classes proceeded with active-learning exercises for the majority of the class period. Active-learning exercises included reading and interpreting electrocardiograms in basic sciences, performing calculations in pharmacology, and discussing and managing cardiac arrhythmia patient cases in therapeutics. Two weeks following the intervention, students were given a cumulative semester final examination for each class that included 5-6 multiple-choice questions on cardiac arrhythmias. The examination tested recall, comprehension, analysis, and synthesis. Table 1 shows an outline of the control and intervention class layouts.
Table 1.
Comparison of Control and Intervention Class Design
To determine the impact of the flipped teaching method on academic performance, the cardiac arrhythmia examination scores of the spring 2012 intervention group, consisting of 101 first-year pharmacy students, were compared to the examination scores of the spring 2011 control group, consisting of 103 first-year pharmacy students, taught using the traditional method.
To assess the perceived value of the flipped teaching method, the intervention group was given a voluntary, anonymous, web-based, 15-item survey administered through Qualtrics Research Suite (Qualtrics, LLC., Provo, UT) 1 week following the flipped pilot. Using a 4-point Likert scale (strongly agree, agree, disagree, strongly disagree), students were asked to rate the helpfulness of the preclass lecture recording, clarity of learning objectives, and overall effectiveness of the flipped method. Free-response feedback was also captured in the survey. The study was deemed exempt by the Touro University Institutional Review Board.
EVALUATION AND ASSESSMENT
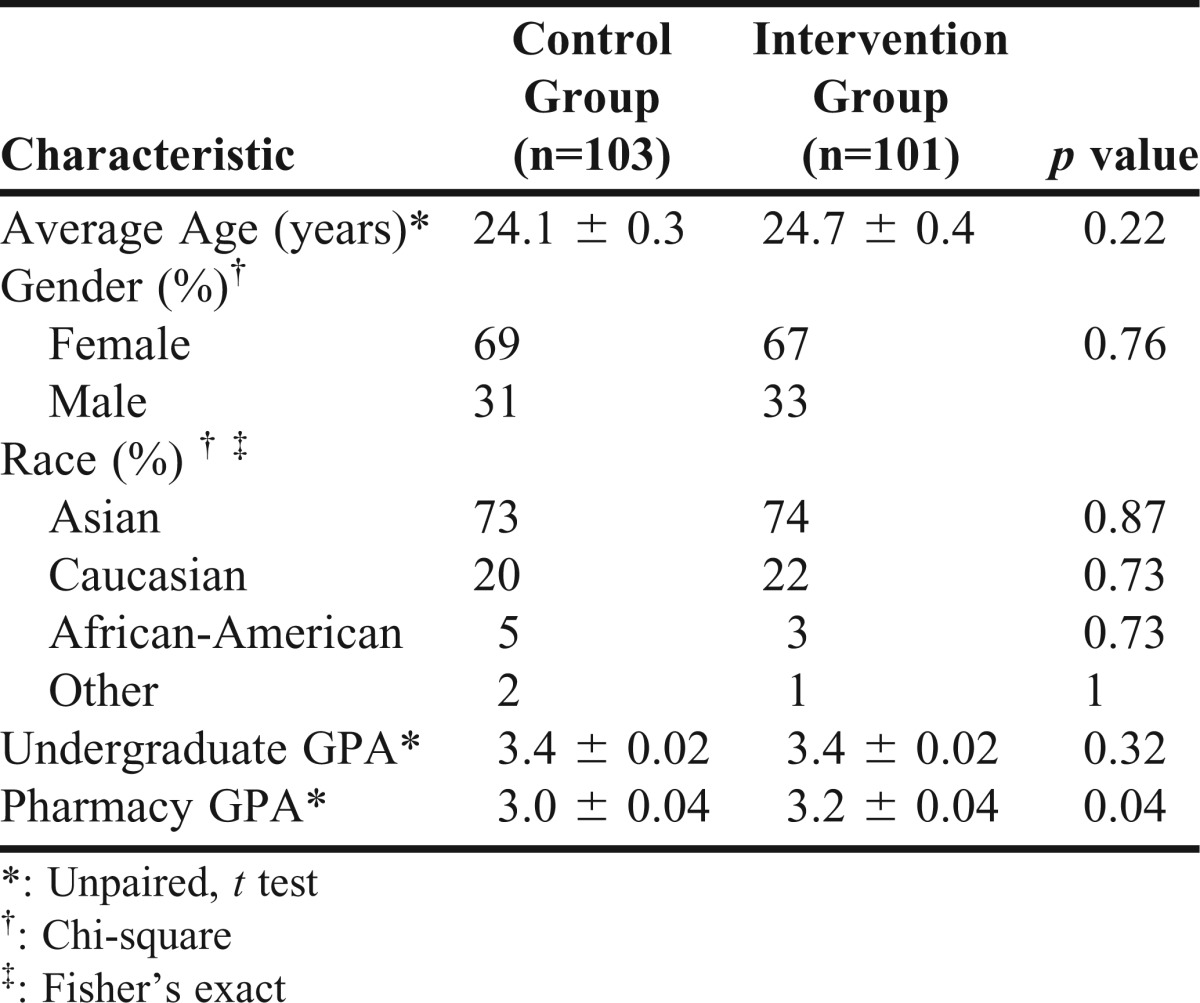
The demographic characteristics of the intervention and control groups did not differ in mean age, gender, or undergraduate grade point average (GPA), though the intervention group had a slightly higher pharmacy GPA (Table 2). Students that did not attend all 3 classes and/or were repeating any of the courses were excluded from the study. The professors and examination questions for both the intervention and control group were the same, though this was not revealed to the students.
Table 2.
Population Demographics
Statistical analysis was performed using GraphPad PRISM 6 (GraphPad Software, Inc., San Diego, CA). Chi-square and student t tests were used to analyze categorical and continuous data, respectively (p<0.05).
RESULTS
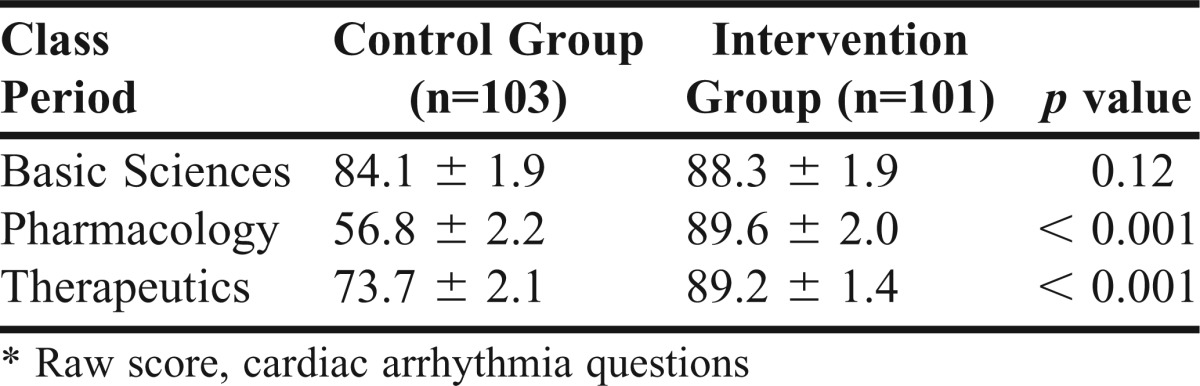
Mean examination scores (on cardiac arrhythmia specific-questions) for the intervention and control groups were 88.3 ± 1.9% vs 84.1 ± 1.9% (p=0.12) for basic sciences, 89.6 ± 2.0% vs 56.8 ± 2.2% (p<0.001) for pharmacology, and 89.2 ± 1.4% vs 73.7± 2.1% (p<0.001) for therapeutics class.
The intervention group showed significantly higher examination scores for 2 of the 3 flipped classes with increases of 32.8 ± 3.0% and 15.5 ± 2.5% for pharmacology and therapeutics classes (Table 3). Mean examination scores for basic sciences did not show significant differences (p=0.12).
Table 3.
Academic Performance Measures – Mean Examination Scores (%)
Sixty-eight out of 101 students completed the flipped teaching survey, a response rate of 67.3%. Answers of strongly agree/agree and strongly disagree/disagree were combined for the analysis of the Likert scale questions (Table 4). The most common feedback was summarized and presented with the percentage defined by number of student comments containing the statement divided by total number of student comments (Table 5). Student satisfaction was found to vary depending on the class.
Table 4.
Survey of Student Perceptions Regarding the Flipped Teaching Method (n=68)
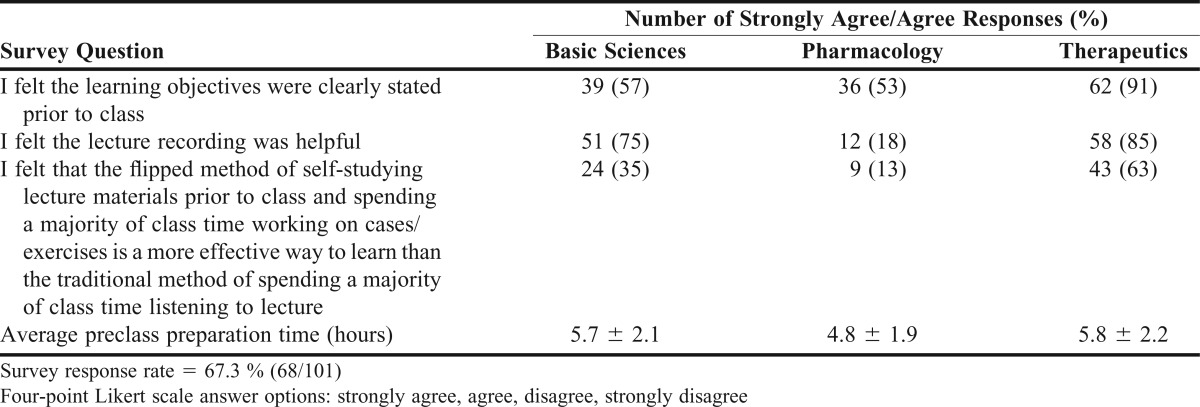
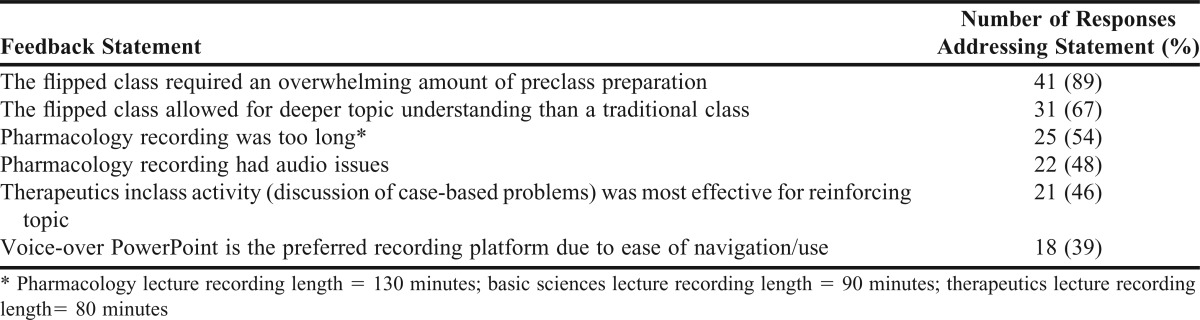
Table 5.
Common Feedback Statements (n=46)
DISCUSSION
Our study showed the flipped teaching method significantly improved cardiac arrhythmia examination scores in 2 of 3 classes (pharmacology and therapeutics), but not the basic sciences class. A possible reason the intervention group did not show significant improvement compared to the control group for the basic sciences class was that the control group already had a relatively high mean examination score. Our findings contributed to the growing body of evidence that the flipped teaching method can improve academic outcomes in pharmacy schools.10,11 Additionally, Ferreri and O’Connor found improved academic performance in a single course after an entire semester of flipped classes,10 and Pierce and Fox found similar improvement after 8 weeks of flipped classes.11 Our week-long flipped teaching pilot showed that improved academic outcomes can result after even shorter exposures. As course-wide or semester-long curricular reform may require substantial efforts, large-scale implementation of flipped teaching may prove challenging for many institutions. Our study showed that flipped teaching could still prove valuable and was capable of improving academic performance on smaller-scale, shorter-duration implementations.
The survey showed that levels of student satisfaction and positive feedback did not necessarily increase with improved examination scores or student acknowledgment of increased topic understanding. This was consistent with various studies on flipped classrooms in pharmacy and nursing schools.10,12 Studies in which flipped teaching was implemented over longer periods of time (weeks to years) uniformly showed a large majority of students to prefer the flipped classroom over the traditional classroom.13-15 As our intervention occurred as a week-long pilot and was a major change from what students normally experienced, a flipped study over a longer period of time may yield higher rates of satisfaction and greater preference for the flipped classroom.
Some frequently addressed areas of concern in the student feedback included quality of audio/video of prerecorded material, length of prerecorded lectures, ease of use of the media platform, and nature of inclass learning activities (Table 5). As the success of a flipped curriculum is underscored by the students’ acceptance and willingness to devote time for self-study prior to class, it will be important to further study these factors. Students felt that the flipped teaching method appeared better suited for therapeutics than pharmacology because the nature of the inclass learning activity of the former (discussion of patient cases) was perceived to be more effective than that of the latter (discussion of calculations). In light of this feedback, it may be that flipped teaching need not be adopted across the entire curriculum, but possibly for certain courses or topics where it is best fit and/or where there may be time constraints, or for material that students historically need more time to grasp.
The most common student complaint was the “overwhelming” amount of preclass preparation time. Thus, to maximize perceived effectiveness, attention must be paid to creating preclass materials of reasonable length. According to feedback, a lecture of 90 minutes or less (basic sciences and therapeutics) was more positively received by students, while a 2-hour lecture (pharmacology) was found to be less favored. In addition, as flipped teaching demands greater amounts of preclass preparation time, the additional demands of this effort must be accounted for by other means of curricular adjustment (eg, increase in the number of course credit/units to reflect expected increase in academic effort, decrease in the amount of inclass time, or decrease in the number of projects outside of class). Implementers must also consider the impact of curricular change on accreditation requirements as coursework done outside of scheduled class time may pose issues with registered course hours. The replacement of official inclass lectures with active-learning activities may also pose of problem if the inclass activities only qualify for laboratory hours rather than lecture hours. Each institution would need to ensure that curricular restructuring efforts meet all accreditation criteria.
Easily used media platforms may also influence student satisfaction. In the feedback, many students stated preferring voice-over PowerPoint slides to the WebEx video recordings because they found the former easier to navigate (ie, find/repeat specific content), and the PowerPoint slides received fewer complaints regarding technical issues than the WebEx video recordings received. McLaughlin, Griffin, and Esserman found students highly preferred flipped teaching that included 35-minute prerecorded lectures, which replaced 75 minutes of traditional lecture time.13 Thus, the traditional 2-hour lectures given at TUCOP may be better received when condensed to 60-minute prerecorded lectures for future flipped classes.
There are several limitations of this study that must be addressed. First, the study analyzed the effects of the flipped teaching method on the single topic of cardiac arrhythmias. It is imperative to see how other topics would fare. Whether the flipped teaching curriculum is effective for more or less complex or time-consuming topics has yet to be determined. Second, the average pharmacy GPA of the intervention group was slightly higher than that of the control group (3.16 ± 0.04 vs 3.04 ± 0.04, respectively). It is possible that improvements in examination scores for the intervention group may have in part been attributed to a slightly higher degree of overall academic performance in the pharmacy program. Third, our flipped teaching pilot involved active communication among the 3 professors across 3 different departments (basic sciences, pharmacology, and therapeutics) prior to delivery. Such implementation across 3 courses/departments was aided by the TUCOP curricular format that organizes blocks of teaching according to organ systems and disease states/topics. As other pharmacy schools may offer different curricular formats and have different opportunities for integration and communication among departments, methods of implementation and results may differ. Also, the assessment of end-of-semester examination scores were within 2 weeks of the intervention. Thus, only relatively short-term academic performance measures could be assessed. Future research may wish to focus on reassessment of academic performance on cardiac arrhythmias further along in the curriculum (ie, an examination covering cardiac arrhythmias 1 year post-intervention, a pre-APPE high stakes examination that includes cardiac arrhythmias, or APPE performance on actual arrhythmia patient cases). Such postintervention assessments may yield information regarding the long-term effectiveness of the flipped teaching method. Further areas of research may also include surveys of faculty member perceptions of, or concerns, regarding the flipped teaching method. This could provide valuable insight and allow teaching institutions to address faculty member readiness and barriers to implementation.
SUMMARY
Flipped teaching allows for increased classroom time for students to engage in active learning that fosters critical thinking, analysis, and the communication skills necessary for today’s student pharmacist. Students in the flipped teaching intervention group achieved significantly higher examination scores than students in the control group. Positive student feedback was seen in classes with higher-rated learning objectives, quality lecture recordings of reasonable length (less than or equal to 90 minutes), and effective inclass activities. Additional studies are needed to assess the effectiveness (academic and perceived) of the flipped teaching method on both short-term and long-term learning in pharmacy school curricula.
ACKNOWLEDGMENT
The authors would like to thank the TUCOP class of 2015 for their participation and feedback.
REFERENCES
- 1.Bergmann J, Sams A. Flip your Classroom: Reach Every Student in Every Class Every Day. Eugene, OR: International Society for Technology in Education; 2012. [Google Scholar]
- 2.Lage M, Platt G, Treglia M. Inverting the classroom: a gateway to creating an inclusive learning environment. J Econ Educ. 2000;31(1):30–43. [Google Scholar]
- 3.Pew Research Center. Millennials: A Portrait of Generation Next. February 2010. http://www.pewsocialtrends.org/files/2010/10/millennials-confident-connected-open-to-change.pdf. Accessed February 9, 2014.
- 4.Prober CG, Khan S. Medical education reimagined: s call to action. Acad Med. 2013;88(10):1407–1410. doi: 10.1097/ACM.0b013e3182a368bd. [DOI] [PubMed] [Google Scholar]
- 5.Blouin RA, Joyner PU, Pollack GM. Preparing for a renaissance in pharmacy education: the need, opportunity, and capacity for change. Am J Pharm Educ. 2008;72(2):Article 42. doi: 10.5688/aj720242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mehta NB, Hull AL, Young JB, Stoller JK. Just imagine: new paradigms for medical education. Acad Med. 2013;88(10):1418–1423. doi: 10.1097/ACM.0b013e3182a36a07. [DOI] [PubMed] [Google Scholar]
- 7.Greiner AC, Knebel E. Health Professions Education: A Bridge to Quality. Washington, DC: National Academies Press; 2003. [PubMed] [Google Scholar]
- 8.Accreditation Council for Pharmacy Education (ACPE) Accreditation Standards and Guidelines for the Professional Program in Pharmacy Leading to the Doctor of Pharmacy Degree. http://www.acpe-accredit.org/pdf/ACPE_Revised_PharmD_Standards_Adopted_Jan152006.pdf. Accessed May 4, 2012.
- 9.American Association of Colleges of Pharmacy. Center for Advancement of Pharmaceutical Education (CAPE) Educational Outcomes. http://www.aacp.org/resources/education/cape/Open%20Access%20Documents/CAPEoutcomes2013.pdf. Accessed December 21, 2013.
- 10.Ferreri SP, O’Connor SK. Redesign of a large lecture course into a small group learning course. Am J Pharm Educ. 2013;77(1):Article 13. doi: 10.5688/ajpe77113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pierce R, Fox J. Vodcasts and active-learning exercises in a “flipped classroom” model of a renal pharmacotherapy module. Am J Pharm Educ. 2012;76(10):Article 196. doi: 10.5688/ajpe7610196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Missildine K, Fountain R, Summers L, et al. Flipping the Classroom to Improve Student Performance and Satisfaction. J Nurs Educ. 2013;52(10):597–599. doi: 10.3928/01484834-20130919-03. [DOI] [PubMed] [Google Scholar]
- 13.McLaughlin JE, Griffin LM, Esserman DA, et al. Pharmacy student engagement, performance, and perception in a flipped satellite classroom. Am J Pharm Educ. 2013 doi: 10.5688/ajpe779196. 12;77(9):Article 196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McLaughlin JE, Roth MT, Glatt DM, et al. The flipped classroom: a course redesign to foster learning and engagement in a health professions school. Acad Med. 2014;89(2):236–243. doi: 10.1097/ACM.0000000000000086. [DOI] [PubMed] [Google Scholar]
- 15.Periyakoil VS, Basaviah P. The flipped classroom paradigm for teaching palliative care skills. Virtual Mentor. 2013;15(12):1034–1037. doi: 10.1001/virtualmentor.2013.15.12.medu1-1312. [DOI] [PMC free article] [PubMed] [Google Scholar]