

Abstract
Cutaneous metastases from primary internal malignancies are an uncommon presentation. Cutaneous metastases are more frequently seen in breast cancer than in any other visceral malignancy in women. Medical practitioners should be vigilant of the possibility of unusual presentations of metastatic disease in breast cancer patients with lobular carcinoma presenting as cutaneous lesions mimicking benign dermatological conditions. Herein, we present a case of a 75-year-old woman presenting with cutaneous lobular breast carcinoma metastases on her anterior right leg, which had previously been misdiagnosed as dermatitis for 9 years.
Keywords: Breast cancer, cutaneous metastases, dermatitis
What was known?
Breast cancer is the most common primary internal malignancy that presents with cutaneous metastases. The most common presentations of breast carcinoma cutaneous metastasis are metastatic nodules followed by alopecia neoplastica and telangiectatic carcinoma.
Introduction
Cutaneous metastasis from primary internal malignancies is an uncommon presentation, with an incidence ranging from 0.7 to 10.4%,[1,2] representing only 2% of all skin malignancies.[3] The incidence of breast carcinoma cutaneous metastasis (BCCM) has been reported as 23.9% in the largest series in the literature,[2] therefore, making it the most common metastases in women seen by dermatologists.[4]
BCCM has a wide range of clinical presentations. Metastatic nodules are the most common followed by alopecia neoplastica, telangiectatic carcinoma and carcinoma erysipeloides.[5] The majority of metastases are reported on the chest wall and other less common sites include the scalp, neck, upper extremities, and back.[6]
Case Report
We report the case of a 75-year-old woman presenting to her GP with a 5 × 3 cm erythematous, flat, cutaneous lesion on her anterior right leg [Figure 1]. This cutaneous lesion had previously been diagnosed as dermatitis without biopsy 9 years ago and been managed with topical corticosteroid preparations. Initially, this course of treatment had provided some temporary benefit. However, over the last year the lesion had become refractory to this treatment and had been slowly enlarging as well as becoming painful and itchy.
Figure 1.

Examination revealed a 5 × 3 cm erythematous, flat skin lesion on the pretibial region of the right leg
In this patient's past medical record, there was a history of a right-sided lobular breast carcinoma with axillary lymph nodal spread that had been managed with surgery, radiotherapy, chemotherapy, and hormonal treatment 10 years prior to this presentation. Additionally, she suffered from type II diabetes mellitus, atrial fibrillation, and had had two previous cerebrovascular events.
After referral to a dermatologist, punch biopsy revealed an infiltrate of malignant cells consistent with spread from an infiltrating lobular carcinoma of the breast [Figure 2]. Further analysis demonstrated that the metastasis contained over 80% estrogen receptor positive cells [Figure 3]. As a result, the patient was commenced on endocrine treatment in the form of exemestane, an aromatase inhibitor. Computed tomography scan of the thorax, abdomen, and pelvis revealed no other metastasis. On follow-up, 6 months after the diagnosis, the lesion was found to be static and the patient's symptoms had resolved. The patient is currently being monitored in outpatient clinic.
Figure 2.
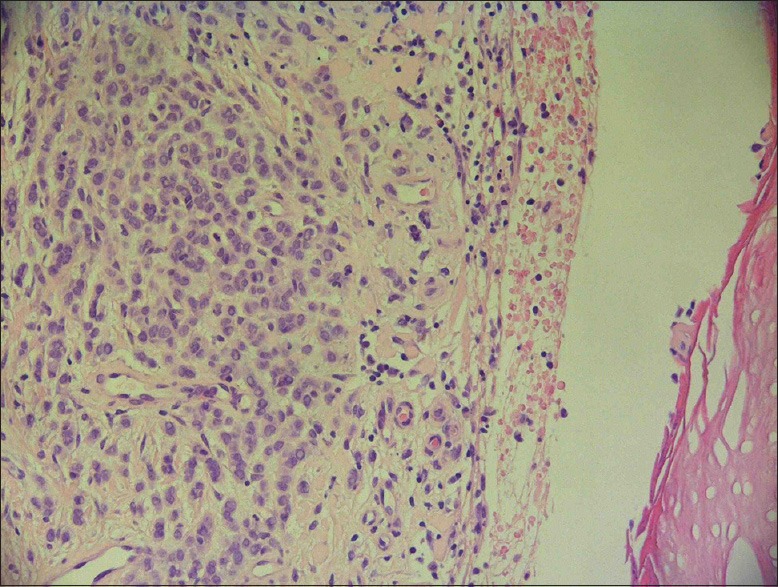
Skin biopsy showed an infiltrate of malignant cells characterized by pleomorphic atypical nuclei and ample pale cytoplasm (hematoxylin and eosin, ×2000)
Figure 3.
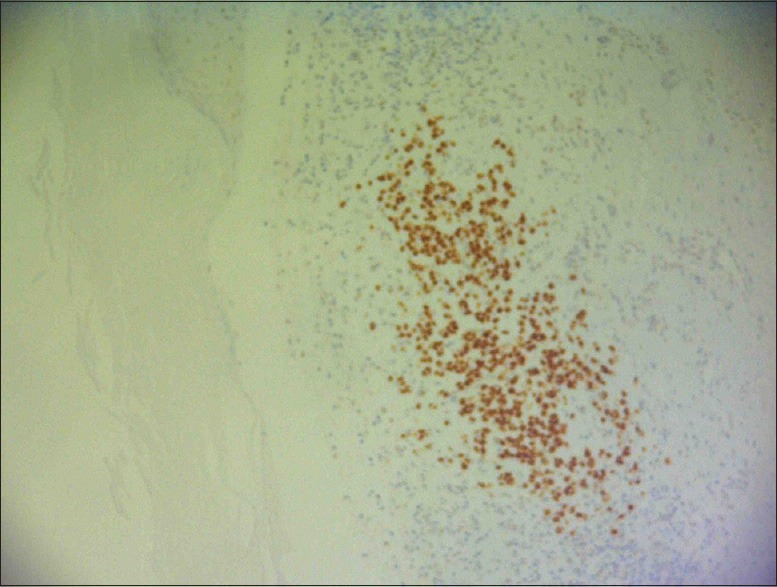
Carcinoma cells in skin biopsy stain positive for estrogen receptors (immunohistochemistry for estrogen receptors, × 1000)
Discussion
Cutaneous metastases are more commonly seen in breast cancer than in any other visceral malignancy in women. Patients can present with cutaneous manifestations of breast disease at the time of their initial diagnosis or on occasion, well after diagnosis and management has been completed. Additionally, these lesions have variable clinical appearances and can be mistaken for benign skin lesions.[7]
The patient in our case presented with a flat, erythematous lesion on her right leg that was misdiagnosed on clinical examination as dermatitis and managed intermittently with topical corticosteroids for 9 years. BCCM commonly presents as a nodular[5] lesion and dermatitis-like appearance is a rare presentation with only two previous cases reported in the literature.[8,9]
A presentation of BCCM that is similar to our case is carcinoma erysipeloides, which is also known as inflammatory breast carcinoma. Carcinoma erysipeloides is an uncommon form of cutaneous metastasis that is characterized by warm, tender, well-demarcated plaques that can resemble erysipelas or cellulitis[5] and therefore can be misdiagnosed and incorrectly treated with antibiotics.
The site of BCCM in our case on the right leg was exceptionally distant to the location of the primary malignancy in the right breast. BCCM usually presents in the chest wall in close proximity to the primary malignancy[5] usually through direct extension or lymphatic spread and less commonly hematogenous spread. The metastatic pathway in our case was likely to be due to lymphatic spread as the patient had previous axillary lymph node involvement. Although there are reports of BCCM in the scalp, neck, back, abdomen, and upper extremities;[6] there are few cases in the literature of lower limb BCCM. The remote location of cutaneous lesion in our case may have led clinicians to assume that it was unrelated to the patient's history of breast cancer.
This unusual case of remote cutaneous breast cancer metastasis that was misdiagnosed for nearly a decade as dermatitis highlights the variable clinical appearance of BCCM. Medical practitioners should be vigilant of the possibility of metastatic disease in breast cancer patients presenting as cutaneous lesions mimicking benign dermatological conditions. If there is any uncertainty regarding the etiology of cutaneous lesion, histological confirmation of diagnosis from tissue biopsy must be carried out. Furthermore, it is important to acknowledge that BCCM may be the first sign of undiagnosed breast cancer[10] and further assessment by breast cancer specialists through triple assessment: Clinical breast examination, mammography or ultrasound, and tissue biopsy of breast mass will be necessary.
What is new?
Breast carcinoma cutaneous metastasis rarely presents as a dermatitis-like skin lesion. Medical practitioners should be vigilant of the possibility of metastatic disease in breast cancer patients presenting as cutaneous lesions at sites remote to the breast that bear a resemblance to benign dermatological conditions.
Acknowledgment
Dr. Ian Seddon, Consultant Histopathologist, for provision of microscope images.
Footnotes
Source of support: Nil
Conflict of Interest: Nil.
References
- 1.Schwartz RA. Cutaneous metastatic disease. J Am Acad Dermatol. 1995;33:161–82. doi: 10.1016/0190-9622(95)90231-7. [DOI] [PubMed] [Google Scholar]
- 2.Lookingbill DP, Spangler N, Helm KF. Cutaneous metastases in patients with metastatic carcinoma: A retrospective study of 4020 patients. J Am Acad Dermatol. 1993;29:228–36. doi: 10.1016/0190-9622(93)70173-q. [DOI] [PubMed] [Google Scholar]
- 3.Nashan D, Meiss F, Braun-Falco M, Reichenberger S. Cutaneous metastases from internal malignancies. Dermatol Ther. 2010;23:567–80. doi: 10.1111/j.1529-8019.2010.01364.x. [DOI] [PubMed] [Google Scholar]
- 4.Alcaraz I, Cerroni L, Rütten A, Kutzner H, Requena L. Cutaneous metastases from internal malignancies: A clinicopathologic and immunohistochemical review. Am J Dermatopathol. 2012;34:347–93. doi: 10.1097/DAD.0b013e31823069cf. [DOI] [PubMed] [Google Scholar]
- 5.De Giorgi V, Grazzini M, Alfaioli B, Savarese I, Corciova SA, Guerriero G, et al. Cutaneous manifestations of breast carcinoma. Dermatol Ther. 2010;23:581–9. doi: 10.1111/j.1529-8019.2010.01365.x. [DOI] [PubMed] [Google Scholar]
- 6.Hussein MR. Skin metastasis: A pathologist's perspective. J Cutan Pathol. 2010;37:e1–20. doi: 10.1111/j.1600-0560.2009.01469.x. [DOI] [PubMed] [Google Scholar]
- 7.Virmani NC, Sharma YK, Panicker NK, Dash KN, Patvekar MA, Deo KS. Zosteriform skin metastases: Clue to an undiagnosed breast cancer. Indian J Dermatol. 2011;56:726–7. doi: 10.4103/0019-5154.91838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ai-Ping F, Yue Q, Yan W. A case report of remote cutaneous metastasis from male breast carcinoma. Int J Dermatol. 2007;46:738–9. doi: 10.1111/j.1365-4632.2006.02923.x. [DOI] [PubMed] [Google Scholar]
- 9.Ahmed M. Cutaneous metastases from breast carcinoma. BMJ Case Rep. 2011;28:2011. doi: 10.1136/bcr.06.2011.4398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cidon EU. Cutaneous metastases in 42 patients with cancer. Indian J Dermatol Venereol Leprol. 2010;76:409–12. doi: 10.4103/0378-6323.66584. [DOI] [PubMed] [Google Scholar]