

Abstract
Background:
Overweight and obesity among children and adolescents is a public health concern.
Objective:
To assess the prevalence of overweight and obesity and its association with social and environmental determinants among the adolescent school children of Tirupati town of Andhra Pradesh, India.
Materials and Methods:
Data was collected by interviewer-administered method from school children aged between 12 to 16 years. The sample consisted of 2258 subjects (1097 boys and 1161 girls). Overweight and obesity were defined by body mass index (BMI) based on the current method recommended by the Centre for Disease Control and Prevention 2000. Data on social and environmental determinants were collected by using a pre-tested and validated questionnaire.
Results:
In the present sample, 11.2 percent and 4.8 percent of boys and 10.3 percent and 4.8 percent of girls were overweight and obese. The literacy level of parents, family income and child sleep duration significantly associated with overweight. Parental level of education was a risk factor for overweight (Mother: 1.570; 95% CI: 1.048-2.354). Similarly increase in family income (OR = 1.529; 95% CI: 1.089-2.148) and child sleep duration <7 hrs per day (OR = 2.006; 95% CI: 1.194-3.371) raised children's association in gaining weight.
Conclusion:
Our study reinforces the burgeoning prevalence of overweight and obesity among the adolescents. Interventional measures taken should consider family, school and physical environment to check the problem of overweight/obesity.
Keywords: Adolescents, body mass index, India, obesity, overweight, socioeconomic factors
INTRODUCTION
Overweight and obesity among children and adolescents is a public health concern, both in developed and developing Nations.[1] In the recent past, epidemiological transition is manifesting with increase in prevalence of non-communicable diseases and decline in communicable diseases. Prospective studies have clearly established an association of over-weight/obesity with non-communicable diseases.[2] Childhood obesity often tracks into adolescence vis-à-vis adults and is linked with increased mortality and morbidity.[3] Published reports have shown that overweight and obesity are associated with impaired glucose tolerance, hypertension, atherosclerotic risk factors and type II diabetes among children and adolescents.[4,5] Further overweight/obese children are frequently prone to unhealthy conditions, academically poor performance, social ineptness and laziness.[6]
In 1998, World Health Organization recognized obesity as a major health problem.[7] According to WHO,[8] the prevalence of obesity is 4.8% in developing countries, 17.1% in transitional countries and 20.4% in developed countries. The causes for the precipitation of overweight and obesity are multifactor including genetic, biological, social, and environmental determinants either collectively or independently affecting weight gain by acting through the mediators of energy metabolism and physical activity.[9] The rising prevalence of obesity among genetically stable population groups indicates that the social and environmental determinants might have importance in understanding the overweight and obesity epidemic.[10] A recent workshop on ‘Education for childhood obesity prevention: A life-course approach’, coordinated by the Pan-American Health Organization and the Pan-American Health and Education Foundation, held on 14 June 2012 in Aruba, as part of the II Pan-American Conference on Childhood Obesity, suggested life course frame work and education as a social determinant of health to address childhood obesity.[11] Towards this end, the Indian Council of Medical Research in its taskforce project cautioned to document information on obesity prevalence and its risk factors across the country in view of diverse cultures.[12] In the light of this information the current study was undertaken to asses the prevalence of overweight and obesity and its association with social and environmental determinants from adolescent school children of Tirupati, Andhra Pradesh, India.
MATERIALS AND METHODS
The present investigation was a cross sectional one, to collect and document the information on anthropometric indicators and social and environmental factors for a population of adolescent school children from Tirupati Town of Andhra Pradesh. The study was under taken between June 2011 to April 2012. The study was approved by the Departmental Ethics Committee of Sri Venkateswara University, Tirupati. Tirupati is one of the largest cities in Rayalaseema regions of Andhra Pradesh State, India.
Study population and design
Study population consisted of school children of both genders between the ages of 12-16 years. According to the available statistics, a total of 45,998 adolescents in the age range of 12-16 years were enrolled in various schools across the town in the academic year 2011-12 (Source: District Educational Office, Chittoor). The study used multistage random sampling technique to have precise estimates of the population. The town consists of 36 municipal wards. Eight wards were picked, and two schools from each ward were randomly selected and children were sampled with probability proportionate to the size. Thus, each individual in the population has the same probability of being sampled. The sample size was established assuming a 95% confidence interval with 3% sampling error. The required sample size was estimated to be 2200 subjects. In the current study, the sample used for the analysis was 2258 subjects (1097 boys and 1161 girls). The overall response rate was 76.0%.
The parents of the wards were contacted over phone by the school management and were explained the objectives of the study prior to obtaining their consent. On receiving their written consent, the children were included in the study. Further oral consent was obtained from each of the school children. Children with any gross abnormality and irregular in attending to the class work were excluded from the study enrollment.
Data collection
A structured schedule was designed with prior validation through pilot study. The questionnaire consisted information on the demographics, education, occupation, socioeconomic conditions of the parents. Further, children's sleep patterns, physical activity, video watching and eating habits were procured. Information on anthropometry like height, weight, waist circumference, hip circumference and skin fold thickness at biceps, sub scapular and abdomen was obtained as per the standard procedures.[13] Weight was measured in light clothing with no shoes, nearest to 10 g. Height of the students was measured with their shoes off and measurement was taken to the nearest 1 mm. Waist circumference was measured to the nearest 0.1 cm horizontally at the narrowest point between lower end of the rib cage and iliac crest. Hip circumference was measured to the nearest 0.1 cm, at the greatest horizontal circumference below the iliac crest at the level of greater trochanter. The triceps skinfold was measured on the back of the right arm over the triceps muscle, midway between the elbow and the acromion process of the scapula. The sub scapular skinfold was measured at the inferior angle of the right scapula. The abdominal skinfold was measured vertically at a site 2 cm to the right side of the umbilicus (bellybutton). Lange skinfold caliper (Cambridge) was used to measure the skinfold thickness. All the measurements were taken twice on the subject with a gap of 5 min and the average was taken for the analysis. Overweight and obesity were considered as BMI above the 85th and 95th percentiles, respectively, as specified for age and sex by Centre for Disease Control and Prevention (CDC) 2000.[14] Waist hip ratio was obtained as waist circumference/hip circumference. The three skin fold measurements were summed to calculate sum of the skin fold thickness.
Statistical analyzes
The data were coded and statistical analysis was carried out through Statistical Package for the Social Sciences software (SPSS version 16.0). Alpha levels were set at 0.05 as statistical significant. Data were provided with descriptive statistics and percentages. Chi square test, student's t-test and ANOVA were used to see the test of significance. The effect of socioeconomic and life style measures on the prevalence of overweight and obesity were analyzed by using odds ratios through multinomial logistic regression model after adjusting for age and sex. The variables that have shown significant variation in the prevalence of overweight and obesity were entered in the model.
RESULTS
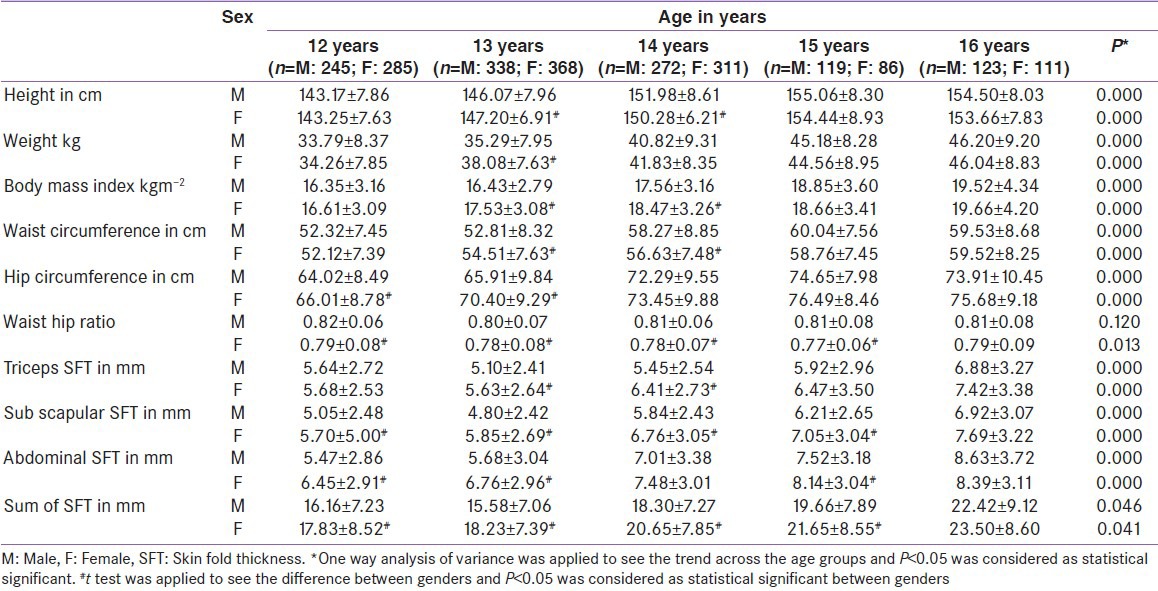
A total of 2258 subjects (1097 boys and 1161 girls) were studied to assess the prevalence of overweight and obesity. The response rate in the subject enrollment was 76 percent. Descriptive statistics for anthropometric measurements in different age groups for adolescent boys and girls were presented in Table 1. Anthropometric measurements like BMI, waist hip ratio and sum of the skin fold thickness have shown an increasing trend (P < 0.05) from 12 years to 16 years, in both boys and girls, except waist hip ratio in girls. Gender comparisons in different age groups indicate that girls were dominating boys in accumulating skin fold thickness at different sites. Waist hip ratio was significantly higher in boys than girls (P < 0.05) except in 16 years of age group. Girls have shown higher BMI than boys in 13 and 14 years age groups (P < 0.05).
Table 1.
Descriptive statistics and anthropometric measurements according to age among adolescent boys and girls
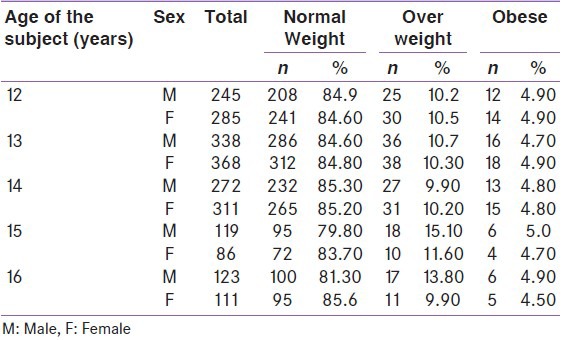
Prevalence of overweight and obesity in the sample was shown in Table 2. In the current sample, 11.2 percent of boys and 10.3 percent of girls were overweight. The obesity prevalence was 4.8 percent in boys and girls. No significant differences were observed in the prevalence of overweight and obesity across the age groups [Table 3]. The prevalence of overweight in 12 year age group of boys and girls were around 10.2 to 10.5 and rose to 9.9 to 13.80 in 16 year age group. Similarly, the obesity was 4.9 percent in 12 year age group and rose to 4.5 to 4.9 percent in 16 year age group.
Table 2.
Prevalence of overweight and obesity among adolescent boys and girls

Table 3.
Age and sex-wise proportion of overweight and obese among the study sample
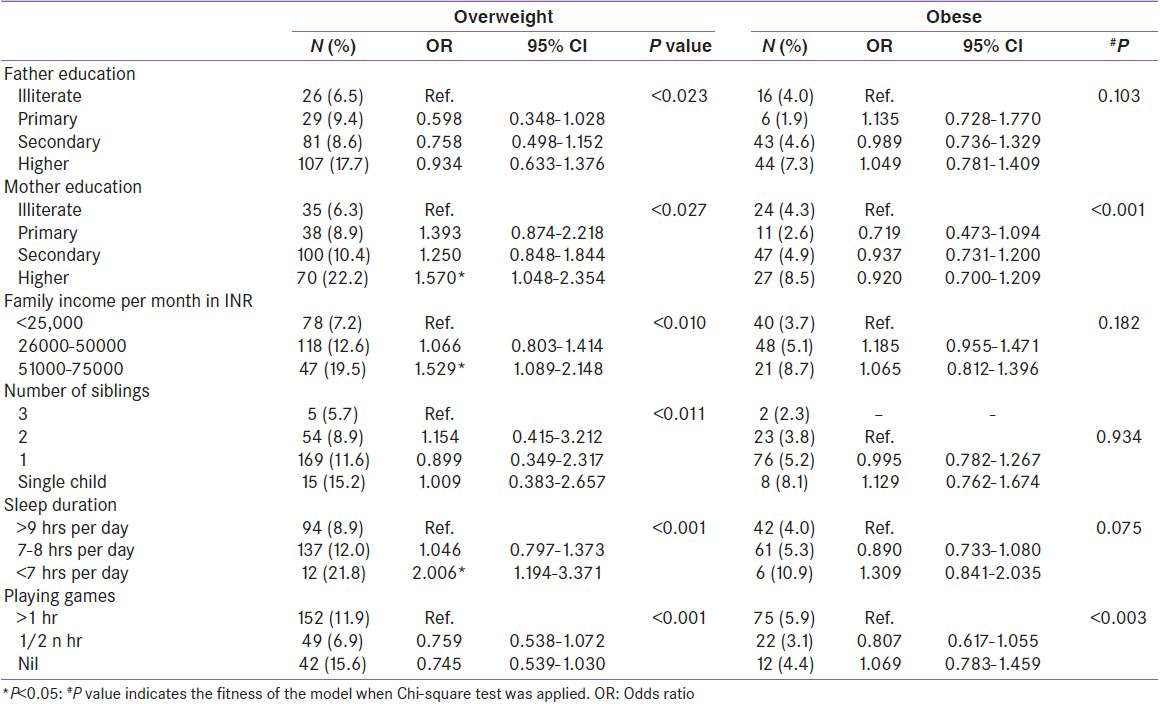
Socioeconomic and life style gradients and its impact on the prevalence of overweight and obesity were shown in Table 4. Children belonging to educated parents show higher rates of overweight and obesity. Increase in family income documented with increase in adolescent overweight and obesity. The prevalence of overweight and obesity was highest in single child and a decreasing trend was seen when number of siblings increased. Overweight and obesity prevalence rates were low in subjects whose sleep duration is 9 hrs and above when compared to 7 hrs and below. Multinomial logistic regression analysis shows that the magnitude of being an overweight child is 1.6 fold (95% CI: 1.048-2.354) when the mother attained higher education. Increased family income raised children's overweight (OR = 1.529; 95% CI: 1.089-2.148). Children's sleep duration for <7 hrs showed 2.0 times (95% CI: 1.194-3.371) association towards overweight when compared to children whose sleep duration was 9 hrs and above per day.
Table 4.
Age and sex adjusted OR and 95% CI for the prevalence of overweight and obesity according to socioeconomic and life style determinants
DISCUSSION
The prevalence of overweight and obesity among the adolescents of the present sample were 10.8% and 4.8%, respectively. The prevalence rates of overweight and obesity were lower when compared to adolescents from Germany (15% and 6%),[15] Portugal (20.3% and 11.3%)[16] and higher than Brazil (9.65% and 2.1%)[17] etc., In the Indian sample, the prevalence of overweight and obesity among affluent girls aged 10-15 years in Chennai was 9.6% and 6.2%, respectively.[18] Another study by Goyal et al.,[19] shows that the prevalence rates of overweight and obesity were 11.75% and 2.2%, respectively. Our results were consistent with other studies indicating that obesity is epidemic in 21st century in Indian continent. In the given situation, if the trend of overweight and obesity is not managed, it may lead to adult overweight and obesity.[3]
The variables associated with overweight, independently seems to be parental education and economy and the child's sleep duration. Parental literacy levels seem to be the most pertinent social problem in India for the observed escalation in overweight and obesity.[20] The association of being overweight was increasing with the increasing levels of mothers education. Prospective studies undergone in developed countries have clearly indicated that lower levels of parental education was a risk factor for childhood obesity.[21] In contrary, developing countries like India noticed weight gain with increased parental education.
Increased economy is negatively correlated with excessive body weight in both adolescents and adults in developed countries.[22] On the contrary, increased economy is associated with increased body weight in developing countries like India as noticed in the present sample.[12] Increased economy may provide an opportunity to have choice and preparation of food. In developed countries, it is assumed that children belonging to families of disadvantaged economic status, because of their lower earning power and decreased knowledge of healthy nutrition, were more exposed to high calorie foods and simple carbohydrates, which are cheaper and easier to access. A reverse trend is being in force in developing countries. Modernization and urbanization offer calorie rich foods for the children being known that it may lead to develop obesity and associated complications. This association appears to be characteristic of a region in an economic transition.[8]
In this sample, sleep time found to be one of the significant environmental problem towards accumulating body weight in adolescents. Less sleep is advantageous in developing many chronic conditions. The adolescent whose sleep time was 7 hrs and less per day witnessed overweight. Similar results were published elsewhere.[23] The limitations of the study were lack of data on food consumption patterns. The captured information on adolescents eating behavior of ice creams, chats, chocolates and fast foods failed to show any association. Probably both parents and children either may have failed to explain or the techniques were not properly validated by the researchers.
In conclusion, the data revealed that the trend of adolescent overweight and obesity is a worrying phenomenon in the national perspective. The findings of the study strongly advocate the need to implement interventional measures for preventing adolescent overweight and obesity.
ACKNOWLEDGMENTS
RKA thank the University Grants Commission (UGC; New Delhi) for the grant support in completing this research successfully (F. No. 39-94/2010 (SR) dt. 24.12.2010). The authors express their gratitude to all the subjects who volunteered into the study and provided necessary information.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Reilly JJ. Obesity in childhood and adolescence: Evidence based clinical and public health perspectives. Postgrad Med J. 2006;82:429–37. doi: 10.1136/pgmj.2005.043836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Stevens GA, Singh GM, Lu Y, Danaei G, Lin JK, Finucane MM, et al. Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Body Mass Index). National, regional, and global trends in adult overweight and obesity prevalences. Popul Health Metr. 2012;10:22. doi: 10.1186/1478-7954-10-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kalra S, Unnikrishnan AG. Obesity in India: The weight of the nation. J Med Nutr Nutraceut. 2012;1:37–41. [Google Scholar]
- 4.Velasquez-Mieyer P, Perez-Faustinelli S, Cowan PA. Identifying children at risk for obesity, type 2 diabetes, and cardiovascular disease. Diabetes Spectrum. 2005;18:213–20. [Google Scholar]
- 5.Mohan V, Jaydip R, Deepa R. Type 2 diabetes in Asian Indian youth. Pediatr Diabetes. 2007;8:28–34. doi: 10.1111/j.1399-5448.2007.00328.x. [DOI] [PubMed] [Google Scholar]
- 6.Chatterjee P. India sees parallel rise in malnutrition and obesity. Lancet. 2002;360:1948. doi: 10.1016/S0140-6736(02)11943-X. [DOI] [PubMed] [Google Scholar]
- 7.WHO: Geneva; 1998. Report of a WHO consultation on obesity. Preventing and managing the global epidemic. [PubMed] [Google Scholar]
- 8.World Health Organization. Geneva: WHO; 2004. Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. WHO Technical Report Series no. 894. [PubMed] [Google Scholar]
- 9.Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity: Public health crisis, common sense cure. Lancet. 2002;360:473–82. doi: 10.1016/S0140-6736(02)09678-2. [DOI] [PubMed] [Google Scholar]
- 10.Hakala P, Rissanen A, Koskenvuo M, Kaprio J, Ronnemaa T. Environmental factors in the development of obesity in identical twins. Int J Obes Relat Metab Disord. 1999;23:746–53. doi: 10.1038/sj.ijo.0800923. [DOI] [PubMed] [Google Scholar]
- 11.Pérez-Escamilla R, Hospedales J, Contreras A, Kac G. Education for childhood obesity prevention across the life-course: Workshop conclusions. Int J Obes Suppl. 2013;3:S18–9. doi: 10.1038/ijosup.2013.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Raj M, Krishna RK. Obesity in children and adolescents. Indian J Med Res. 2010;132:598–607. [PMC free article] [PubMed] [Google Scholar]
- 13.Weiner JS, Lourie JA. General medical examinations, techniques. Practical Human Biology, Academic Press. 1981 [Google Scholar]
- 14.Gonzalez-Casanova I, Sarmiento OL, Gazmararian JA, Cunningham SA, Martorell R, Pratt M, et al. Comparing three body mass index classification systems to assess overweight and obesity in children and adolescents. Rev Panam Salud Publica. 2013;33:349–55. doi: 10.1590/s1020-49892013000500006. [DOI] [PubMed] [Google Scholar]
- 15.Kurth BM, Schaffrath Rosario A. The prevalence of overweight and obese children and adolescents living in Germany. Results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS) Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2007;50:736–43. doi: 10.1007/s00103-007-0235-5. [DOI] [PubMed] [Google Scholar]
- 16.Pandez C, Mourao I, Moreira P, Rosado V. Prevalence and risk factors for overweight and obesityin Portuguese children. Acta Paediatr. 2005;94:1550–7. doi: 10.1080/08035250510042924. [DOI] [PubMed] [Google Scholar]
- 17.Guedes DP, Rocha GD, Silva AJ, Carvalhal IM, Coelho EM. Effects of social and environmental determinants on overweight and obesity among Brazilian schoolchildren from a developing region. Rev Panam Salud Publica. 2011;30:295–302. [PubMed] [Google Scholar]
- 18.Subramanyam V, Jayshree R, Rafi M. Prevalence of overweight and obesity in affluent adolescent girls in Chennai in 1981 and 1998. Indian Pediatr. 2003;40:332–6. [PubMed] [Google Scholar]
- 19.Goyal RK, Shah VN, Saboo BD, Phatak SR, Shah NN, Gohel MC, et al. Prevalence of overweight and obesity in Indian adolescent school going children: Its relationship with socioeconomic status and associated lifestyle factors. J Assoc Physicians India. 2010;58:151–8. [PubMed] [Google Scholar]
- 20.Ghosh A. Rural-urban comparison in prevalence of overweight and obesity among children and adolescents of Asian Indian origin. Asia Pac J Public Health. 2011;23:928–35. doi: 10.1177/1010539511428697. [DOI] [PubMed] [Google Scholar]
- 21.Lamerz A, Kuepper-Nybelen J, Wehle C, Bruning N, Trost-Brinkhues G, Brenner H, et al. Social class, parental education, and obesity prevalence in a study of six-year-old children in Germany. Int J Obes (Lond) 2005;29:373–80. doi: 10.1038/sj.ijo.0802914. [DOI] [PubMed] [Google Scholar]
- 22.Wang Y, Beydoun MA. The obesity epidemic in the United States--gender, age, socioeconomic, racial/ethnic, and geographic characteristics: A systematic review and meta-regression analysis. Epidemiol Rev. 2007;29:6–28. doi: 10.1093/epirev/mxm007. [DOI] [PubMed] [Google Scholar]
- 23.Kleiser C, Schaffrath Rosario A, Mensink GB, Prinz-Langenohl R, Kurth BM. Potential determinants of obesity among children and adolescents in Germany: Results from the cross-sectional KiGGS study. BMC Public Health. 2009;9:46. doi: 10.1186/1471-2458-9-46. [DOI] [PMC free article] [PubMed] [Google Scholar]