

Dear Sir,
We read with great interest Metwalley and El-Saied paper on the development of abnormal glucose tolerance in Egyptian children and adolescents with β-thalassemia major (TM). The prevalence of diabetes mellitus (DM) was 5% (three out of 60 patients), and impaired glucose tolerance test was reported in five out of 60 patients (8%). The development of abnormal glucose tolerance was associated with alteration in oxidant-antioxidant status, antioxidant capacity and insulin resistance (IR).[1]
The interplay between liver siderosis and hepatitis C virus (HCV) infection facilitates the progression to DM, at least in adulthood.[2] This potential effect seems to be related to different HCV genotypes. The specific mechanisms by which HCV leads to diabetes are not fully understood, but it seems that an increase of IR associated with both steatosis and the overproduction of proinflammatory cytokines could play a crucial role.[3]
Many TM patients are infected with either HCV or hepatitis B virus, particularly those who were born before the 1990s.[4] Therefore, we aimed to investigate if there was any association between insulin-dependent DM in TM patients and HCV-RNA positivity and different genotypes.
We enrolled 148 TM patients (age range: 15–53 years; 72 males and 76 females), 78 were HCV-RNA positive. Fifteen patients (10.1%) had insulin dependent DM. In all of them (eight females) and in 46 nondiabetic TM patients the HCV genotype was done using specific primers. Serum HCV-RNA was detected using a sensitive polymerase chain reaction assay.
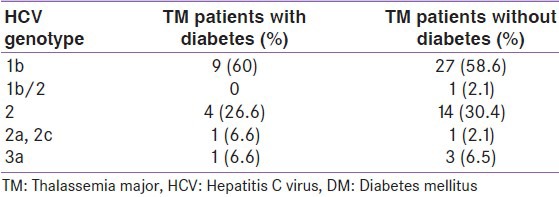
The most common genotype in TM patients with and without DM was 1b [Table 1]. Using Chi-square test, a statistical difference between the two groups was not found.
Table 1.
HCV genotypes in TM patients with and without insulin dependent DM
We also assessed the frequency of DM in TM patients with HCV+ and HCV-RNA−, and HCV+ and HCV-RNA+. Again no difference was found between groups.
A multiple regression analysis was also conducted using multiple linear fitting with least squares method. No significant correlation was observed between biochemical parameters (albumin, total protein, liver enzymes or international normalized ratio) serum ferritin, insulin growth factor 1 on the one hand and HCV-RNA status on the other hand.
Although a “divorce” between HCV infection and diabetes is in the air;[5] before the dogma on the role of IR in the pathogenesis of HCV infection is excluded, we believe that these findings need to be replicated in larger studies and across other ethnic groups. A better knowledge of the pathogenic mechanisms involved in diabetes associated with HCV infection will enable us not only to further identify those patients at high risk of developing diabetes, but also to select the best therapeutic option.[3]
We wish to thank the members of International Network of Clinicians for Endocrinopathies in Thalassemia and Adolescence Medicine-A network: Giuseppe Raiola, Maria Concetta Galati, Saveria Campisi, Salvatore Anastasi (Italy) and Mohamed El Kholy (Egypt) for taking part the study.
Sincerely yours,
REFERENCES
- 1.Metwalley KA, El-Saied AR. Glucose homeostasis in Egyptian children and adolescents with ß-thalassemia major: Relationship to oxidative stress. Indian J Endocrinol Metab. 2014;18:333–9. doi: 10.4103/2230-8210.131169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.De Sanctis V, Soliman A, Yassin M. Iron overload and glucose metabolism in subjects with ß-thalassaemia major: An overview. Curr Diabetes Rev. 2013;9:332–41. doi: 10.2174/1573399811309040005. [DOI] [PubMed] [Google Scholar]
- 3.Lecube A, Hernández C, Genescà J, Esteban JI, Jardí R, Simó R. High prevalence of glucose abnormalities in patients with hepatitis C virus infection: A multivariate analysis considering the liver injury. Diabetes Care. 2004;27:1171–5. doi: 10.2337/diacare.27.5.1171. [DOI] [PubMed] [Google Scholar]
- 4.Mancuso A. Hepatocellular carcinoma in thalassemia: A critical review. World J Hepatol. 2010;2:171–4. doi: 10.4254/wjh.v2.i5.171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cusi K. The relationship between hepatitis C virus infection and diabetes: Time for a divorce? Hepatology. 2014;60:1121–3. doi: 10.1002/hep.27252. [DOI] [PubMed] [Google Scholar]