

Abstract
Objective:
The purposes of this retrospective study were to represent a newly designed theoretical model for determining orifice shape and morphologic properties of mandibular premolars and to correlate these findings with each other.
Materials and Methods:
A total of 287 mandibular premolar images obtained from 88 patients by cone-beam computed tomography were included in this study. The measurements were performed below the cementoenamel junction, and different orifice configurations were defined in accordance with various ratios. The age and gender of the patient, the tooth type and position, the number of roots, orifice configuration, root canal configuration, presence of C-shaped canal, and the presence of radicular groove were recorded. It was also recorded whether the root canal becomes round or not and if any, length of the root canal from the orifice to the section in which it becomes round. Furthermore, the theoretical model for determining orifice shape was defined after measurements. The orifice shape was determined as round, oval, flat, keyhole-shaped, and T-shaped, and orifices with short, normal length, and long isthmus. Statistical analyses were performed using Chi-square and Spearman's rank correlation tests (P = 0.05).
Results:
Orifice configurations were, usually, flat (37%), or keyhole-shaped (23%). The prevalence of T-shaped was found to be 3.8%. The prevalence of C-shaped canals was found to be 2.1%. The percentage of root canals that became round in the middle or apical thirds was 95.1%. Radicular grooves were detected in 37 (24%) of first premolars and six (4.5%) of second premolars. Statistical analysis revealed that the mean length of distance until the canal reached a round shape varied according to age group (r = −0.270; P < 0.001). There was a statistically significant difference between radicular groove and tooth type (P < 0.001).
Conclusions:
The mean length of distance until the canal reached a round shape correlated with the patient's age. The new theoretical model could be beneficial to determine orifice configurations.
Keywords: Cone-beam computed tomography, isthmus, mandibular premolars, orifice, theoretical modeling, Turkish
INTRODUCTION
Successful management of endodontic cases stems from a detailed understanding of the morphology of the root canal system. Adequate chemomechanical preparation and effective obturation of the root canal system are based on knowledge of normal root canal morphology and variations from the norm obtained from studies of root and canal morphology.[1] The complexity of root canal anatomy presents clinical challenges and difficulties that often lead to poor endodontic outcomes.[2,3,4]
The morphology of root canal systems of mandibular premolar teeth may differ depending on the population.[5,6,7,8] Previous studies have shown that these teeth show diversity in orifice configuration (round to irregular) root canal configuration (single canal to C-shaped) and the root morphology (more roots to radicular groove).[6,9] The variations in mandibular premolar teeth attract attention and may result in missing root canals, periodontal problems, nonsurgical endodontic treatment failure, and the need for surgical procedures.
Cone-beam computed tomography (CBCT) has been used to evaluate the morphology of root canals.[10,11,12,13] CBCT provides a practical tool for non-invasive and three-dimensional reconstructive imaging by clinicians in endodontic applications and morphological analyses allowing measurements. The purposes of this retrospective study were to present a theoretical model using CBCT images for determining orifice shape and morphologic properties of mandibular premolars, such as orifice configuration, root canal configuration, and radicular groove, and to correlate these findings, including the mean length of distance until the canal became round (with also age, gender and tooth type considered).
MATERIALS AND METHODS
We selected 248 previously obtained CBCT images from the archive of the Department of Oral and Maxillofacial Radiology of Izmir Katip Celebi University, Izmir. All images were obtained with a NewTom 5G CBCT machine (NewTom 5G®, QR, Verona, Italy) from patients with different dentomaxillofacial problems between October 2012 and June 2013. The voxel size was 0.15 mm, and a slice thickness was 0.150 mm. The acquisition process was performed by an experienced radiologist according to the manufacturer's recommended protocol.
Inclusion criteria were the presence of (1) high-quality CBCT images, and (2) CBCT images of at least one mandibular premolar. Exclusion criteria were the presence of (1) coronal restoration, (2) root canal fillings and posts, (3) internal/external resorption, (4) primary mandibular premolars, (5) impacted teeth in the mandibular premolar region, (6) periapical lesion, (7) immature apex, and (8) deep caries. The CBCT images of 287 mandibular premolar teeth from 88 patients who met the inclusion criteria were analyzed with NNT software version 3.00 (QR srl, Verona, Italy) using a Dell Precision T5400 workstation (Dell, Round Rock, TX, USA).
Two independent endodontists assessed the axial, sagittal, and coronal sections, and in quantitative analysis where a consensus was not reached, an oral radiologist was asked to perform a decisive evaluation.
The following were recorded:
Age and gender of the patient: The ages of the patients were divided into three sections (13-30; 31-50; and 51-70)
Tooth type and position
Number of roots
Orifice configuration: For determining this, the axial section below the cementoenamel junction was used.[8,14] The buccolingual length of the orifice was defined as R1. The orifice was divided into three parts buccolingually [Figure 1] and R2 was defined as the mesiodistal length in the middle part. The long mesiodistal length in the buccal or lingual parts was defined as d1. The short mesiodistal length in the buccal or lingual parts was defined as d2 [Figures 1 and 2]. The ratios (R2/R1; R2/d2; R1/d1; d1/d2; d1/R2) were calculated to determine the shape of the orifice. The theoretical model to determine the shape of orifice is shown in Figure 3. According to this modeling process:
Figure 1.
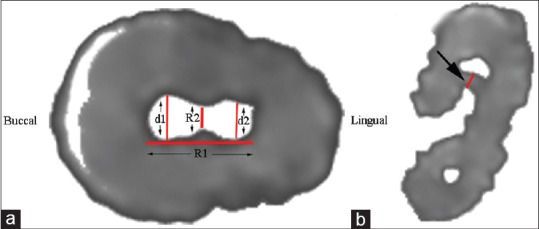
Shows measurements. (a) R1: Buccolingual length of orifice, R2: Mesiodistal length in the middle of the orifice, d1-d2: The mesiodistal length in the buccal and lingual parts was defined as d1 (long) and d2 (short), and (b) shortest distance between the root canal and outer surface of the groove
Figure 2.
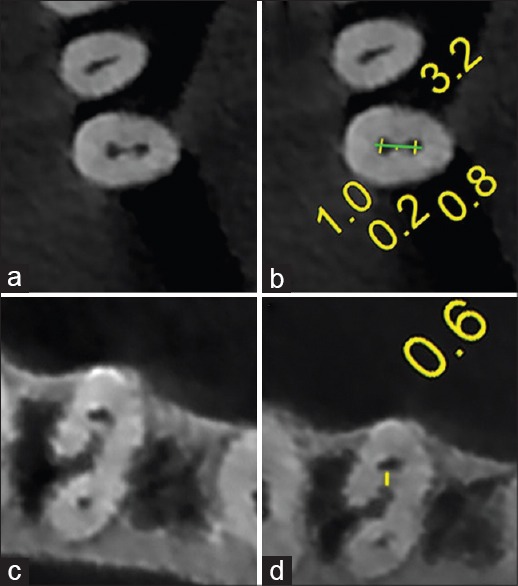
Measurements on the cone-beam computed tomography images. (a and b) Lengths measurements at the orifice, (c and d) shortest distance between the root canal and outer surface of the groove
Figure 3.

Theoretical model for determining orifice configuration (R1: The buccolingual length of the orifice, R2: The mesiolingual length in the middle after the orifice was divided into three parts buccolingually, d1: The long mesiodistal length in the buccal or lingual part of the orifice, d2: The short mesiodistal length in the buccal or lingual part of the orifice)
Round canal orifice
The orifice shape was determined as round if the R2/R1 was equal to 1 ± 0.4.
Oval canal orifice
If the R2/R1 was between 0.6 and 0.3, the orifice shape was defined as oval.
If the R2/R1 was small than 0.3, following definitions was performed:
Keyhole shaped canal orifice
If R2/d2 was between 0.5 and 2, R1/d1 was between 1.5 and 4, and d1/d2 was smaller than 2; the orifice shape was defined as keyhole shaped canal orifice.
T shaped canal orifice
If R2/d2 was between 0.5 and 2, R1/d1 was between 1.5 and 4, d1/R2 was >2, and d1/d2 was >3; the orifice shape was defined as T shaped canal orifice.
If R2/d2 was <0.5 and d1/R2 was >2, the orifice was defined as orifice with isthmus. The length of the isthmus was defined as follows:
Canal orifice with short isthmus
If R1/d1 was <1.5, the shape was defined as canal orifice with short isthmus.
Canal orifice with normal isthmus
If R1/d1 was between 1.5 and 4, the shape was defined as canal orifice with normal isthmus.
Canal orifice with long isthmus
If R1/d1 was >4, the shape was defined as canal orifice with long isthmus.
Flat canal orifice
If R2/R1 was <0.3 and the other ratios did not match with the model above, the orifice shape was defined as flat. The model was controlled by four authors for randomly selected teeth.
Whether root canal becomes round: This was recorded by evaluating axial sections of the images obtained from the root canals, excluding those with round orifices, if any:
Length of root canal from the orifice to the section in which it becomes round: The numbers of the axial sections showing an orifice and a round root canal were recorded. Then the length was calculated according to the following formula: 0.150 mm × (section number of orifice − section number where root canal becomes round)
-
Root canal configuration: The axial cross sections were evaluated. The root canal configuration was categorized using Vertucci's classification[15] as the main reference. Additional forms of root canals were also evaluated using additional types reported by Awawdeh and Al-Qudah,[5] and Sert and Bayirli.[16] It was accepted that the beginning configuration of the root canal was two in the teeth with isthmus.
- Type I (1): In this type, single root canal leaves the pulp chamber and ends as single foramen
- Type II (2–1): Two root canals leave the pulp chamber and end as single foramen
- Type III (1–2–1): In this type, single root canal leaves the pulp chamber, separates into two separate root canals, and ends as single foramen
- Type IV (2): Two root canals leave the pulp chamber and end as two foramina
- Type V (1–2): In this type, single root canal leaves the pulp chamber and ends as two foramina
- Type VI (2–1–2): Two root canals leave the pulp chamber, join again as single root canal, and end as two foramina
- Type VII (1–2–1–2): In this type, single root canal leaves the pulp chamber, separates into two separate root canals. These root canals join again as a single root canal, and end as two foramina
- Type VIII (3): Three root canals leave the pulp chamber, and end as three foramina
- Additional type (2–1–2–1) (introduced by Sert and Bayirli[16]): Two root canals leave the pulp chamber, join again as single root canal, which separates into two branches and end as one foramina
- Additional type (1–2–3) (introduced by Awawdeh and Al-Qudah[5]): Single root canal leaves the pulp chamber, separates into two separate root canals, and end as three foramina
- Additional type (1–3-1) (introduced by Awawdeh and Al-Qudah[5]): Single root canal leaves the pulp chamber, separates into three separate root canals, and end as one foramina
- Additional type (1–3-2) (introduced by Awawdeh and Al-Qudah[5]): Single root canal leaves the pulp chamber, separates into three separate root canals, and end as two foramina
- Additional type (1–2-3–2) (introduced by Awawdeh and Al-Qudah[5]): Single root canal leaves the pulp chamber, separates into two separate root canals. These root canals separate into three root canals, and end as two foramina.
To avoid confusing definitions of root canal complexity, two distinct categories were used: “Noncomplex” and “complex”. The root canals with Vertucci type I classification was defined as non-complex and the others were defined as complex. Also, those with type I which did not become round were defined as complex.
Presence/absence of C-shaped canal: According to the Fan's classification, only type 1, 2, 3, and 4 was defined as C-shaped root canal[17]
Presence/absence of the groove: If any:
Length of the groove: The numbers of the axial sections showing the start and finish of the groove were recorded. Then, the length of the groove was calculated according to the following formula:
0.150 mm × (start section number-finish section number)
The lengths were classified to three categorize as 0-3, 3-6, and 6-9 mm.
Statistical analysis
Statistical analyses were performed using Chi-square and Spearman's rank correlation tests (P = 0.05). All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 16.0 software (SPSS Inc., Chicago, USA).
RESULTS
In this study, 47 patients were female, and 41 male, and were aged between 13 and 70 years (mean 35.50). CBCT images of 160 patients did not meet the criteria of the study. Consequently, CBCT images of 287 mandibular premolar teeth were evaluated by the examiners, namely, 154 mandibular first premolars (77 right and 77 left), and 133 mandibular second premolars (64 right and 69 left). Sixty-seven patients had bilateral mandibular first premolars, and 58 patients had bilateral mandibular second premolar teeth. Among them, 68 bilateral teeth had the same orifice configurations, 105 had the same root canal configurations, five teeth had bilateral C-shaped root canals, and 11 had bilateral radicular grooves.
Among the mandibular first premolars, 19 had two roots, and among the mandibular second premolars, five had two roots.
The frequency distribution of the orifice configuration according to tooth type is shown in Table 1. Statistical analysis revealed no significant association between the orifice configuration and tooth type (P = 0.764) and gender (P = 0.345). However, there was a statistically significant difference between orifice configuration and age (P = 0.001).
Table 1.
Number of percentage of orifice configuration

The frequency distribution of the C-shaped root canal configuration according to tooth position is shown in Table 1. Six teeth (2.1%) exhibited a C-shaped root canal system. Statistical analysis revealed no significant association between the presence of a C-shaped root canal configuration and tooth type (P = 0.812), gender (P = 0.242), and age (P = 0.347). The Pearson correlation test revealed that there was a moderate correlation between the presence of a C-shaped root canal configuration and the presence of a groove (r = 0.348; P < 0.001).
Table 2 shows the number of teeth with root canals which became round according to tooth type. The mean length of distance until the canal reached the round shape varied according to age groups [Table 3]. The Pearson correlation test revealed that there was a moderately negative correlation between them (r = −0.270; P < 0.001).
Table 2.
Number of tooth with root canal which becomes round according to tooth type

Table 3.
Length of root canal from the orifice to the section in which it becomes round according to age group (mm)

The frequency distribution of different canal configurations is shown in Table 4. Overall, type I, which indicated one root canal, was the most prevalent (n = 233, 81.1%), and 2.1% (n = 6) had a C-shaped root canal system. Root canal configurations of 1–2–3 and 1–3–2 which have not been demonstrated in recent literature are shown in Figure 1. Chi-square statistical test revealed no significant association between root canal configuration, gender (P = 0.422), and age (P = 0.207). However, there was a statistically significant difference between root canal configuration and tooth type (P < 0.001).
Table 4.
Number of percentage of root canal configuration

Table 5 shows the distribution of orifice configuration according to non-complex and complex root canal configurations. The Chi-square statistical test revealed no significant association between the orifice configuration and root canal configuration (P = 0.002). The least percent of complex root canals was determined in the root canal systems with keyhole shaped orifices (14.9%).
Table 5.
Number of percentage of orifice configuration with noncomplex and complex root canal configuration

The radicular grooves were detected in 37 (24%) of the first premolars, and 6 (4.5%) of second premolars. The perpendicular length of the groove and the shortest distance between the root canal and the outer surface of the groove according to the tooth type are seen in Table 6. Chi-square statistical analysis revealed that no significant association between the presence of radicular groove and gender (P = 0.722), and age (P = 0.094). However there was statistically significant difference between radicular groove and tooth type (P < 0.001).
Table 6.
The details of radicular grooves according to tooth type

DISCUSSION
One of the aims of this study was to define orifice configurations in mandibular premolars. Previously, it has been demonstrated that the pulp chamber floor is usually below this anatomic landmark.[18] Thus, the measurements were performed below the cementoenamel junction. A preliminary study conducted in order to calculate the numeric range of the different orifice configuration. Different numeric range was determined for each orifice configuration according to the shape of the orifice. The ratios were obtained and orifice configurations were logically defined using these ratios. According to obtained data a new theoretical model was developed. Structural model index that ribbon like shape corresponding to 0 scholastic math inventory (SMI) score or cylindrical shape corresponding to an SMI of 3 was used in the previous studies.[19,20] In the present theoretical model classifications were detailed with respect to isthmus length and five different canal shapes. Statistically significant differences were determined between the orifice configuration and tooth type [Table 1]. Overall, orifices usually had a flat (37%) or keyhole shape (%23). Keyhole shape could be clinically significant because the incidence of complex root canal configuration was minimal in teeth with this orifice shape. In the present study, a new classification called T shape was defined. T shape classification is similar to keyhole shape with having a ledge but they are different with having round or flat canals in the remaining part. The incidence of T shaped canal was 3.8% in the present study.
An isthmus is an anatomical variant found in root canals and is defined as a narrow, ribbon-shaped communication between two root canals.[9] In the present study, the narrowness was defined logically and orifices with isthmuses were recorded as two root canals. This method could be beneficial in solving instability of whether there are one or two root canals.
Root canal treatment procedures are more difficult in teeth with complex anatomical structures, such as oval canals. A round root canal allows manipulation and control over instrumentation and obturation. Fan et al.[6] stated that the morphology of the canal in the mandibular first premolar was usually oval at the coronal third, round or oval in the middle third, and round in the apical third. Similarly, in the present study, 95.1% of root canals became round. Expecting this finding, the mean length of the distance until the canal reached a round shape was measured and correlated with age. Interestingly, it varied according to age groups. A predisposition of the long of root canal where it becomes round was determined to decrease in younger patients. This result has clinical inference in that young patients could be much more likely to have non-circular long canals.
Calıskan et al.,[21] who determined the incidence of a second canal in a Turkish population, reported a single canal in 64% of first premolars and 94% of second premolars. They also reported 53% and 39% of these teeth had lateral canals respectively. Similarly, in their investigation the root and canal morphology of mandibular permanent teeth on a Turkish population, Sert et al.[22] encountered that 62% of mandibular first premolar and 71% mandibular second premolar had single canal. Sert and Bayirli[16] detailed the gender differences of root canal configurations in same populations and determined that 65% of the male and 56% of the female mandibular first premolars had a single canal, whereas the incidence of a single canal in the second premolars was 57% and 85% for males and females, respectively. The possibility of the second premolars having a single root canal in females was almost twice that of males. In the first premolars, lateral canals existed in 22% of males and 6% of females, whereas in the second premolars, the ratio was 9% and 24% for males and females, respectively. Investigators also encountered fourteen new root canal configurations in their study that was not included in the classification other classification systems. Ok et al.[23] have reported that the prevalence of one canal was 93.5% for the mandibular first premolar, and 98.5% for the second premolar. They also found that the incidence of one canal was higher on the right side and females. The literature on mandibular premolar teeth in the Turkish population reveals that the incidence of one canal in the mandibular first premolar was reported to be considerably wide range. As well as these studies provide a general estimation on the root canal configuration, additionally our study details the orifice configuration new theoretical model.
Cone-beam computed tomography has been used as a tool to examine root canal morphology in different populations.[12,24,25] Neelakantan et al.[26] demonstrated that CBCT is as accurate as the canal staining and clearing technique in identifying root canal morphology. This study was conducted using CBCT and showed that the incidence of complex root canal configurations in mandibular premolars was 19.8% (n = 54). This result is in accordance with Yang et al.[27] who reported 22.5% in a study of a Chinese subpopulation. It was higher than that reported by Khedmat et al. (11.5%)[7] and lower than that reported by Awawdeh and Al-Qudah (35.7%),[5] and Velmurugan and Sandhya (28%).[28] The differences among the studies may be due to the differences in the ethnicity.
The incidence of C-shaped root canal configurations in mandibular premolars was reported from 1% to 24% in different populations.[6,28] In this study, the prevalence of C-shaped canals in mandibular premolars in a Turkish population was approximately 2%, which was similar to a previous report by Khedmat et al.(1.3%).[7] No statistically significant association was found between the presence of C-shaped root canal configurations and tooth type, gender, and age.
The radicular groove is a developmental malformation that extends along the root to varying lengths.[29] The radicular grooves might not give the patient any sign until it presents advanced periodontal pathosis and secondary pulpal involvement.[30] The shortest distance between the root canal and outer surface of the groove can vary from 0 to 1 mm regardless of age, gender or tooth type. This finding is important because of the risk of perforation during root canal preparation. Fan et al.[6] demonstrated that grooves can extend up to 9.5 mm. Similarly, in the present study, it was demonstrated that although most of them (55%) can extend 3-6 mm, 7.4% of the radicular grooves can extend up to 6-9 mm. An inevitable finding was that a correlation was found between the presence of C-shaped root canal configurations and the presence of grooves. Thus, it can be suggested that radicular grooves can result in C-shaped roots, and consequently, C-shaped root canal configurations.
CONCLUSION
Thorough preparation of the mandibular premolars can be difficult due to their complex variations, ranging from orifice shape to root canal configuration. If the benefits of CBCT outweigh detriments in a case, CBCT could be beneficial in understanding the kinds of diversity awaiting the clinician. The presented theoretical model could be beneficial in determining orifice configurations. The ratios could be used in anatomical studies in which root canals will be evaluated.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared
REFERENCES
- 1.Sachdeva GS, Ballal S, Gopikrishna V, Kandaswamy D. Endodontic management of a mandibular second premolar with four roots and four root canals with the aid of spiral computed tomography: A case report. J Endod. 2008;34:104–7. doi: 10.1016/j.joen.2007.10.004. [DOI] [PubMed] [Google Scholar]
- 2.Barbizam JV, Ribeiro RG, Tanomaru Filho M. Unusual anatomy of permanent maxillary molars. J Endod. 2004;30:668–71. doi: 10.1097/01.don.0000121618.45515.5a. [DOI] [PubMed] [Google Scholar]
- 3.Ayranci LB, Arslan H, Topcuoglu HS. Maxillary first molar with three canal orifices in MesioBuccal root. J Conserv Dent. 2011;14:436–7. doi: 10.4103/0972-0707.87222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Poorni S, Karumaran CS, Indira R. Mandibular first premolar with two roots and three canals. Aust Endod J. 2010;36:32–4. doi: 10.1111/j.1747-4477.2009.00170.x. [DOI] [PubMed] [Google Scholar]
- 5.Awawdeh LA, Al-Qudah AA. Root form and canal morphology of mandibular premolars in a Jordanian population. Int Endod J. 2008;41:240–8. doi: 10.1111/j.1365-2591.2007.01348.x. [DOI] [PubMed] [Google Scholar]
- 6.Fan B, Yang J, Gutmann JL, Fan M. Root canal systems in mandibular first premolars with C-shaped root configurations. Part I: Microcomputed tomography mapping of the radicular groove and associated root canal cross-sections. J Endod. 2008;34:1337–41. doi: 10.1016/j.joen.2008.08.006. [DOI] [PubMed] [Google Scholar]
- 7.Khedmat S, Assadian H, Saravani AA. Root canal morphology of the mandibular first premolars in an Iranian population using cross-sections and radiography. J Endod. 2010;36:214–7. doi: 10.1016/j.joen.2009.10.002. [DOI] [PubMed] [Google Scholar]
- 8.Lee MM, Rasimick BJ, Turner AM, Shah RP, Musikant BL, Deutsch AS. Morphological measurements of anatomic landmarks in pulp chambers of human anterior teeth. J Endod. 2007;33:129–31. doi: 10.1016/j.joen.2006.08.016. [DOI] [PubMed] [Google Scholar]
- 9.Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10:3–29. [Google Scholar]
- 10.Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone-beam computed tomography to identify root canal systems in vitro. J Endod. 2008;34:87–9. doi: 10.1016/j.joen.2007.10.016. [DOI] [PubMed] [Google Scholar]
- 11.Blattner TC, George N, Lee CC, Kumar V, Yelton CD. Efficacy of cone-beam computed tomography as a modality to accurately identify the presence of second mesiobuccal canals in maxillary first and second molars: A pilot study. J Endod. 2010;36:867–70. doi: 10.1016/j.joen.2009.12.023. [DOI] [PubMed] [Google Scholar]
- 12.Zhang R, Wang H, Tian YY, Yu X, Hu T, Dummer PM. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J. 2011;44:990–9. doi: 10.1111/j.1365-2591.2011.01904.x. [DOI] [PubMed] [Google Scholar]
- 13.Zhang R, Yang H, Yu X, Wang H, Hu T, Dummer PM. Use of CBCT to identify the morphology of maxillary permanent molar teeth in a Chinese subpopulation. Int Endod J. 2011;44:162–9. doi: 10.1111/j.1365-2591.2010.01826.x. [DOI] [PubMed] [Google Scholar]
- 14.Min Y, Fan B, Cheung GS, Gutmann JL, Fan M. C-shaped canal system in mandibular second molars Part III: The morphology of the pulp chamber floor. J Endod. 2006;32:1155–9. doi: 10.1016/j.joen.2006.07.004. [DOI] [PubMed] [Google Scholar]
- 15.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 16.Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30:391–8. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 17.Fan W, Fan B, Gutmann JL, Fan M. Identification of a C-shaped canal system in mandibular second molars. Part III. Anatomic features revealed by digital subtraction radiography. J Endod. 2008;34:1187–90. doi: 10.1016/j.joen.2008.06.013. [DOI] [PubMed] [Google Scholar]
- 18.Krasner P, Rankow HJ. Anatomy of the pulp-chamber floor. J Endod. 2004;30:5–16. doi: 10.1097/00004770-200401000-00002. [DOI] [PubMed] [Google Scholar]
- 19.Peters OA, Peters CI, Schönenberger K, Barbakow F. ProTaper rotary root canal preparation: Effects of canal anatomy on final shape analysed by micro CT. Int Endod J. 2003;36:86–92. doi: 10.1046/j.1365-2591.2003.00626.x. [DOI] [PubMed] [Google Scholar]
- 20.Versiani MA, Leoni GB, Steier L, De-Deus G, Tassani S, Pécora JD, et al. Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file, Reciproc, WaveOne, and ProTaper universal systems. J Endod. 2013;39:1060–6. doi: 10.1016/j.joen.2013.04.009. [DOI] [PubMed] [Google Scholar]
- 21.Caliskan MK, Pehlivan Y, Sepetçioglu F, Türkün M, Tuncer SS. Root canal morphology of human permanent teeth in a Turkish population. J Endod. 1995;21:200–4. doi: 10.1016/S0099-2399(06)80566-2. [DOI] [PubMed] [Google Scholar]
- 22.Sert S, Aslanalp V, Tanalp J. Investigation of the root canal configurations of mandibular permanent teeth in the Turkish population. Int Endod J. 2004;37:494–9. doi: 10.1111/j.1365-2591.2004.00837.x. [DOI] [PubMed] [Google Scholar]
- 23.Ok E, Altunsoy M, Nur BG, Aglarci OS, Colak M, Güngör E. A cone-beam computed tomography study of root canal morphology of maxillary and mandibular premolars in a Turkish population. Acta Odontol Scand. 2014:1–6. doi: 10.3109/00016357.2014.898091. [DOI] [PubMed] [Google Scholar]
- 24.Kim Y, Lee SJ, Woo J. Morphology of maxillary first and second molars analyzed by cone-beam computed tomography in a korean population: variations in the number of roots and canals and the incidence of fusion. J Endod. 2012;38:1063–8. doi: 10.1016/j.joen.2012.04.025. [DOI] [PubMed] [Google Scholar]
- 25.Zheng Q, Zhang L, Zhou X, Wang Q, Wang Y, Tang L, et al. C-shaped root canal system in mandibular second molars in a Chinese population evaluated by cone-beam computed tomography. Int Endod J. 2011;44:857–62. doi: 10.1111/j.1365-2591.2011.01896.x. [DOI] [PubMed] [Google Scholar]
- 26.Neelakantan P, Subbarao C, Ahuja R, Subbarao CV, Gutmann JL. Cone-beam computed tomography study of root and canal morphology of maxillary first and second molars in an Indian population. J Endod. 2010;36:1622–7. doi: 10.1016/j.joen.2010.07.006. [DOI] [PubMed] [Google Scholar]
- 27.Yang H, Tian C, Li G, Yang L, Han X, Wang Y. A cone-beam computed tomography study of the root canal morphology of mandibular first premolars and the location of root canal orifices and apical foramina in a Chinese subpopulation. J Endod. 2013;39:435–8. doi: 10.1016/j.joen.2012.11.003. [DOI] [PubMed] [Google Scholar]
- 28.Velmurugan N, Sandhya R. Root canal morphology of mandibular first premolars in an Indian population: a laboratory study. Int Endod J. 2009;42:54–8. doi: 10.1111/j.1365-2591.2008.01494.x. [DOI] [PubMed] [Google Scholar]
- 29.Lee KW, Lee EC, Poon KY. Palato-gingival grooves in maxillary incisors. A possible predisposing factor to localised periodontal disease. Br Dent J. 1968;124:14–8. [PubMed] [Google Scholar]
- 30.Attam K, Tiwary R, Talwar S, Lamba AK. Palatogingival groove: endodontic-periodontal management – case report. J Endod. 2010;36:1717–20. doi: 10.1016/j.joen.2010.06.025. [DOI] [PubMed] [Google Scholar]