

Abstract
Objectives:
The present study evaluated the gingival condition among school going children in Sharjah, United Arab Emirates and determined its relationship with tooth brushing frequency, diet and dental caries.
Materials and Methods:
Four hundred and five children participated in the study. There were 232 boys (57%) and 173 (43%) girls. Children were grouped based on age as ≤6 years (n = 84) mean age 4.72 ± 0.50 and >6 years (n = 321) mean age 8.47 ± 1.65. The amount of dental plaque and gingival condition were assessed on the inner and outer surface of six index teeth using Silness and Loe and Loe and Silness criteria. Dental caries status was assessed using WHO 1997 criteria. Dental examination, tooth brushing frequency and 24 h diet chart were recorded by calibrated dentists. Logistic regression analysis was used to determine the predictors of gingivitis.
Results:
Increase in decayed, missing, and filled teeth values corresponds to increase in plaque index and gingival index scores (P ≤ 0.05). A logistic regression analysis of the predictors of gingivitis showed that males were 2.11 times less likely to have gingivitis compared with females (odds ratio [OR]: 0.47,95% confidence interval [CI]: 0.24-0.93, P = 0.03) and children aged ≤6 years were 3.06 times less likely to have gingivitis than those aged >6 years (OR: 0.33, 95% CI: 0.17-0.62, P = 0.00). Tooth brushing frequency and diet were not significant predictors.
Conclusion:
Current study clearly demonstrated that female gender and children more than 6 years were more likely to have gingivitis.
Keywords: Dental caries, gingival index, gingivitis, plaque index, school children
INTRODUCTION
Children with healthy gingival tissues most likely progress to adult life with good periodontal health.[1] Previous reports indicate that a periodontal disease is the second most frequent dental problem in children and adults.[2] Children often manifest periodontal disease as inflammation of the gingival tissue.[3] Studies in the Arab region showed moderate to the high prevalence of gingivitis in children, in Yemen 27% of the 5-year olds and 78.6% of the 12-year olds had gingivitis.[4] Prevalence of gingivitis was reported to be 97% in 6-7-year-old children in Iran.[5]
Gingivitis in children occurs, usually, as a result of bacterial plaque accumulation on the cervical margins of the teeth.[6] The amount of plaque accumulation in children varies in accordance to their tooth brushing frequency,[7] diet[8] and dental caries.[9] The severity of gingivitis observed in children could also depend on the above-mentioned factors.[7,8,9] Gender differences in the levels of plaque and gingivitis has been previously reported, where males tended to have significantly lower PI scores, but higher gingival index (GI) scores than females.[9] Since gingival inflammation is prevalent in children and adolescents, it is important to identify the factors that could influence the occurrence of gingivitis in its early stages. This could improve our understanding of the disease progression and could facilitate a treatment planning and oral hygiene care for children in need.[3]
Until date, there is a paucity of information on the status of gingival health in school children living in the United Arab Emirates (UAE). Therefore, the present study was undertaken to evaluate the gingival condition among school children in Sharjah, UAE and to determine its relationship with tooth brushing frequency, diet and dental caries.
MATERIALS AND METHODS
This cross-sectional study was conducted on a sample of 405 children who attended the pediatric dentistry teaching clinic at the University of Sharjah, from 2011 to 2013. The sample comprised of 232 (57%) boys and 173 (43%) girls. Children were grouped based on age, as ≤6 years, age range 3–6 years (n = 84) mean age 4.72 ± 0.50 and >6 years, age range 6–12 years (n = 321) mean age 8.47 ± 1.65. This study was approval by the Research and Ethics Committee, University of Sharjah. All parents signed consent forms. In this study, children with medically compromising conditions such as diabetes,[10] leukemia[11] and immunodeficiency[12] that could affect the periodontal health were excluded. Healthy children presently not undergoing orthodontic or periodontal treatment were included in this study.
All examinations were performed by dentists who passed an intra or inter-examiner calibration before the beginning of the study. The children were examined for gingival condition and dental caries while seated on the dental chair. The amount of dental plaque and gingival condition were assessed on the inner and outer surfaces of six index teeth. Silness and Loe[13] criteria were used to quantify plaque deposition, whereas gingival status was assessed using GI of Loe and Silness.[14] The average amount of plaque accumulation and the gingival condition in school children were measured and categorical scores were used. Dental caries was charted using WHO 1997 criteria.[15] Dental examination, tooth brushing frequency and 24 h diet chart were recorded on pediatric dentistry case sheet by calibrated dentists.[16] The diet was classified depending on the physical characteristics of the food as mixed and soft while examining the 24 h dietary recall chart. The parents of each child were asked to list everything their child consumed from the present to the previous day. The co-investigator reviewed the diet chart. Consumption of soft and liquid food was classified as soft diet, whereas inclusion of fruits, vegetables and cereals in the daily diet were considered as mixed.
Data were analyzed using the Statistical Package for Social Sciences SPSS version 21. Descriptive statistics, Chi-square, Spearman's rho, Kruskal–Wallis and Mann–Whitney tests were used to examine the relationship between dental caries, plaque and gingivitis scores (dependent variables) and age, gender, tooth brushing frequency and diet, the independent variables in this study. Logistic regression analysis was used to assess the relationship between gingivitis (present vs. absent) and possible risk factors (gender [male vs. female], age (≤6 years vs. >6 years), diet (soft vs. mixed) and tooth brushing frequency (irregular tooth brushing vs. one vs. twice vs. three)). Level of significance was set at α = 0.05 (two-tailed).
RESULTS
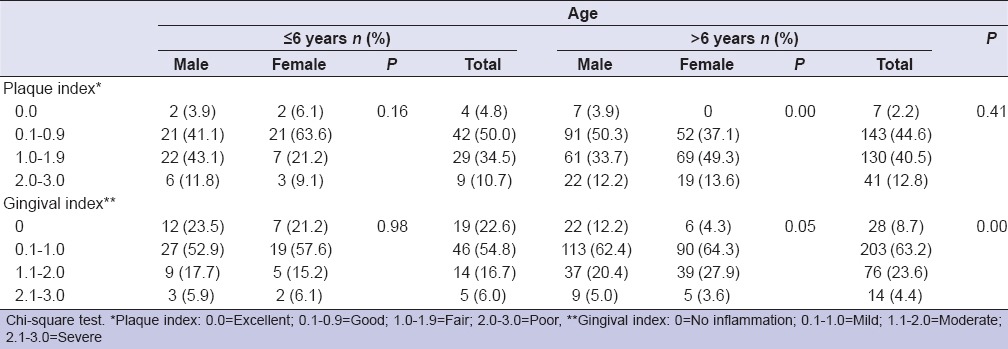
The mean plaque, gingival, decayed, missing, and filled teeth (dmft), DMFT scores for both males and females children in both age categories are shown in Table 1. Mean PI scores were significantly higher in males ≤6 years than females (mean: 1.63 [SD: 075] vs. mean = 1.33 [SD: 0.74]; P = 0.002). Whereas among children >6 years old, females had higher mean scores compared with males (mean: 1.76 [SD: 0.67] vs. mean: 1.54 [SD: 0.76], P = 0.02; respectively). Table 2 depicts the results of the association between plaque and gingival scores with age and gender. The results show that, females >6 years had significantly higher plaque and GI scores compared to male (P < 0.05). It is also apparent that children >6 years had higher gingival scores compared to those ≤6 years.
Table 1.
Mean plaque index, gingival index, DMFT and dmft scores in children ≤6 and >6 years old
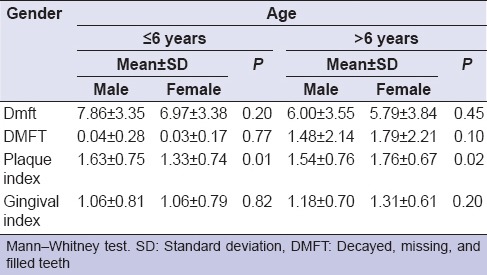
Table 2.
Relationship of plaque and gingival indices with the age and gender
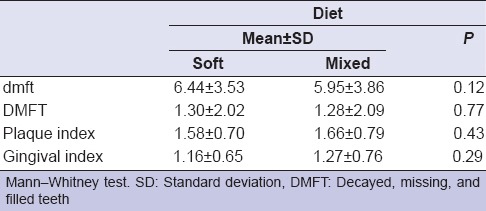
In the present sample, the majority of the children brushed their teeth once a day. And we could not observe a significant correlation between tooth brushing frequency and plaque and gingival score values (P > 0.05). The association between dental caries mean plaque and gingival scores are depicted in Table 3. An increase in primary dmft values corresponded to increase in plaque index and GI scores (P ≤ 0.05), although not significant, a similar trend was observed in DMFT scores (P = 0.06, P = 0.13, respectively). The present study showed no significant correlation between the physical structure of the diet with dmft/DMFT and plaque/GI scores [Table 4] (P > 0.05).
Table 3.
Relationship between plaque and gingival indices with mean DMFT/dmft scores

Table 4.
Relationship of dmft, DMFT, plaque and gingival indices with diet
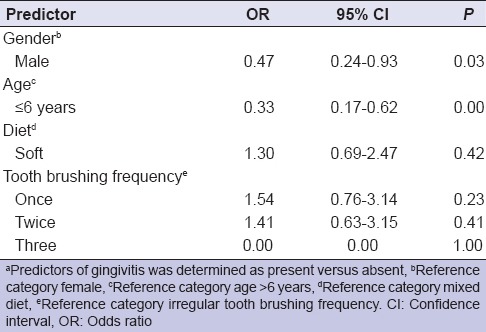
Logistic regression analysis of the predictors of gingivitis showed that males were 2.11 (odds ratio [OR] = 0.47) times less likely to have gingivitis compared with females (OR= 0.47, 95% confidence interval [CI]: 0.24-0.93; P = 0.03). Children who were 6 years of age and below were 3.06 times less likely to have gingivitis compared with older children (OR = 0.33, 95% CI: 0.17-0.62; P = 0.00). Other factors such as tooth brushing frequency and diet were not significantly associated with gingivitis [Table 5].
Table 5.
Logistic regression output on the predictors of gingivitisa
DISCUSSION
This study assessed the gingival condition and determined the predictors of gingivitis in schoolchildren in Sharjah, UAE. The sample comprised of 232 boys and 173 girls. The sample size used in this study is adequate to observe approximately 20% prevalence of moderate to severe gingivitis using a power of 80% and α level of 0.05 (two-tailed). Our findings showed higher gingivitis scores than previously reported in Yemen among 5-year-old children, in which, the mean plaque and gingivitis scores were 0.35 (SD: 0.47) and 0.19 (SD: 0.38); respectively. The mean dmft scores noted in the present study are higher than the previously reported mean dmft (4.9 ± 4.3) in 5- and 6-year-olds from Ajman, UAE.[17] In children >6-year-old mean plaque and GI scores were higher when compared with 12-year-old children from Yemen.[4] However, in a study conducted among Jordanian school children it was reported that 14–15 year olds had higher GI when compared with the present >6 year old group.[9] Whereas, the mean DMFT scores in >6 year olds noted in the present study are comparable to national survey of the oral health in 12 and 15 year old school children in the UAE, in which the mean DMFT at 12 years was 1.6.[18] These findings indicate that children in Sharjah, UAE have poor oral health. Hence, there is a need for oral health education and promotion among children in this age group in the UAE.
In the present study, plaque scores in 6-year-old boys were higher than girls; this could be due to the lack of proper supervised tooth brushing in young children.[19] It can also be speculated that 6-year-old boys are less likely to follow oral hygiene instructions when compared to girls because a male child is interested in outdoor activities. However, in children >6 year old, girls had a higher plaque and GI scores. This could be attributed to lack of appropriate tooth brushing. In the present study, it was observed that most of the children brushed their teeth once a day, but we did not observe a significant correlation between frequency of tooth brushing and gingival inflammation. This could be attributed to false reporting of tooth bushing practices. Gingival inflammation noted to be higher in the our study among girls >6 years old could be explained by early onset of puberty compared to boys.[20] In the present study girls >6 year old had a higher plaque and GI compared to boys. These findings were also reported by Mascarenhas.[21] To the contrary, Qaderi and Taani in Jordan,[9] Weissenbach et al.[22] in France showed that boys had a higher plaque and GI compared with girls. This lack of agreement could be related to culture difference, in which parents may pay more attention to their male than female children. While comparing the gingival health between age groups, children >6 years had higher mean GI score values compared to children ≤6 years, this finding is in agreement to previous results reported by Al-Haddad et.al.[4] in which 12-year-old children had a higher GI compared to 5-year-old.[4]
Consistent with previous research[23] increase plaque and GI scores were associated with increased dmft/DMFT. Similar findings were also observed in 13-15-year-old adolescents where increased DT values were significantly associated with increasing GI.[24] Therefore, fair (1.0-1.9) plaque scores observed in the present study could be attributed to caries development in primary and permanent teeth. Pain and sensitivity from decayed teeth might have prevented children from masticating on certain quadrants. This, compounded with poor tooth brushing practices, observed in the present study could explain the positive association between dmft/DMFT and GI.
The association between the physical characteristics of the diet, dental caries and gingival health was explored in this study. It was assumed that a child consuming a mixed diet with fiber content will have a better cleansing effect on the teeth and surrounded soft tissues leading to reduced susceptibility to dental caries and gingivitis. However, we did not observe a statistically significant difference between diet and dental caries or gingivitis. Nevertheless, the mean dmft/DMFT in children consuming soft diet with no fiber content was higher than children consuming mixed diet. Previously it was shown that, sucrose consumption presumably a soft diet was associated with increased visible plaque and risk of developing dental caries in 6-year-olds, which was 1.7 times higher compared to children consuming sweets once a week or less.[25]
Regression analysis in the current study clearly demonstrated that females and children aged more than 6-years were likely to have gingivitis. Though the status of gingival health in children have been assessed in the neighboring Arab countries, this information is scarce in the UAE.[4,5,9] Therefore, the findings of the present study contributed to the knowledge on the presence of gingivitis in children in the age range of 3-6 and >6-12 years.
Limitations of this study include that data were not collected on the children's socioeconomic status, which is known to have an effect on children's oral health.[2]
More information regarding the children's diet such as sugar intake, frequency of snacking could also have provided additional evidence regarding the relationship between diet, gingivitis and dental caries.
In view of the presence of dental caries and gingivitis in children living in the UAE, efforts should be made to control this disease by encouraging good oral and dental health for children at the community and individual levels. Skills required to improve oral hygiene practices in children could be refined by teaching and motivating them to brush their teeth through implementing preventive programs in public and private schools in the country.
CONCLUSION
Current study clearly demonstrated that female gender and children more than 6-years were more likely to have gingivitis.
ACKNOWLEDGMENT
We would like to thank Dr. Marwa Moustafa for her assistance in data analysis and statistics.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared
REFERENCES
- 1.Jenkins WM, Papapanou PN. Epidemiology of periodontal disease in children and adolescents. Periodontol 2000. 2001;26:16–32. doi: 10.1034/j.1600-0757.2001.2260102.x. [DOI] [PubMed] [Google Scholar]
- 2.Chiapinotto FA, Vargas-Ferreira F, Demarco FF, Corrêa FO, Masotti AS. Risk factors for gingivitis in a group of Brazilian schoolchildren. J Public Health Dent. 2013;73:9–17. doi: 10.1111/jphd.12001. [DOI] [PubMed] [Google Scholar]
- 3.Bossnjak A, Curilovic Z, Vuccicevic-Boras V, Plancak D, Jorgic-Srdjak K, Relja T, et al. Prevalence of gingivitis in 6- to 11-year-old Croatian children. Eur J Med Res. 2003;8:313–7. [PubMed] [Google Scholar]
- 4.Al-Haddad KA, Ibrahim YT, Al-Haddad AM, Al-Hebshi NN. Assessment of gingival health status among 5- and 12-year-old children in Yemen: A Cross-Sectional Study. ISRN Dent 2013. 2013:352621. doi: 10.1155/2013/352621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jalaleddin H, Ramezani GH. Prevalence of gingivitis among school attendees in Qazvin, Iran. East Afr J Public Health. 2009;6:171–4. [PubMed] [Google Scholar]
- 6.López R, Fernández O, Baelum V. Social gradients in periodontal diseases among adolescents. Community Dent Oral Epidemiol. 2006;34:184–96. doi: 10.1111/j.1600-0528.2006.00271.x. [DOI] [PubMed] [Google Scholar]
- 7.Kolawole KA, Oziegbe EO, Bamise CT. Oral hygiene measures and the periodontal status of school children. Int J Dent Hyg. 2011;9:143–8. doi: 10.1111/j.1601-5037.2010.00466.x. [DOI] [PubMed] [Google Scholar]
- 8.Al-Ahmad A, Roth D, Wolkewitz M, Wiedmann-Al-Ahmad M, Follo M, Ratka-Krüger P, et al. Change in diet and oral hygiene over an 8-week period: Effects on oral health and oral biofilm. Clin Oral Investig. 2010;14:391–6. doi: 10.1007/s00784-009-0318-9. [DOI] [PubMed] [Google Scholar]
- 9.El-Qaderi SS, Quteish Ta’ani D. Dental plaque, caries prevalence and gingival conditions of 14-15-year-old schoolchildren in Jerash District, Jordan. Int J Dent Hyg. 2006;4:150–3. doi: 10.1111/j.1601-5037.2006.00184.x. [DOI] [PubMed] [Google Scholar]
- 10.Al-Khabbaz AK, Al-Shammari KF, Hasan A, Abdul-Rasoul M. Periodontal health of children with type 1 diabetes mellitus in Kuwait: A case-control study. Med Princ Pract. 2013;22:144–9. doi: 10.1159/000342624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Demirer S, Ozdemir H, Sencan M, Marakoglu I. Gingival hyperplasia as an early diagnostic oral manifestation in acute monocytic leukemia: A case report. Eur J Dent. 2007;1:111–4. [PMC free article] [PubMed] [Google Scholar]
- 12.Rwenyonyi CM, Kutesa A, Muwazi L, Okullo I, Kasangaki A, Kekitinwa A. Oral Manifestations in HIV/AIDS-Infected Children. Eur J Dent. 2011;5:291–8. [PMC free article] [PubMed] [Google Scholar]
- 13.Silness J, Loe H. Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condtion. Acta Odontol Scand. 1964;22:121–35. doi: 10.3109/00016356408993968. [DOI] [PubMed] [Google Scholar]
- 14.Loe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol Scand. 1963;21:533–51. doi: 10.3109/00016356309011240. [DOI] [PubMed] [Google Scholar]
- 15.4th ed. Geneva: WHO; 1997. World Health Organization Oral Health Surveys Basic Methods; pp. 40–52. [Google Scholar]
- 16.Gopinath VK. Assessment of nutrient intake in cleft lip and palate children after surgical correction. Malays J Med Sci. 2013;20:61–6. [PMC free article] [PubMed] [Google Scholar]
- 17.Hashim R, Williams SM, Thomson WM, Awad MA. Caries prevalence and intra-oral pattern among young children in Ajman. Community Dent Health. 2010;27:109–13. [PubMed] [Google Scholar]
- 18.El-Nadeef MA, Al Hussani E, Hassab H, Arab IA. National survey of the oral health of 12- and 15-year-old schoolchildren in the United Arab Emirates. East Mediterr Health J. 2009;15:993–1004. [PubMed] [Google Scholar]
- 19.Khadri FA, Gopinath VK, Hector MP, Davenport ES. How pre-school children learn to brush their teeth in Sharjah, United Arab Emirates. Int J Paediatr Dent. 2010;20:230–4. doi: 10.1111/j.1365-263X.2010.01042.x. [DOI] [PubMed] [Google Scholar]
- 20.Felimban N, Jawdat D, Al-Twaijri Y, Al-Mutair A, Tamimi W, Shoukri M, et al. Pubertal characteristics among schoolgirls in Riyadh, Saudi Arabia. Eur J Pediatr. 2013;172:971–5. doi: 10.1007/s00431-012-1752-2. [DOI] [PubMed] [Google Scholar]
- 21.Mascarenhas AK. Determinants of caries prevalence and severity in higher SES Indian children. Community Dent Health. 1999;16:107–13. [PubMed] [Google Scholar]
- 22.Weissenbach M, Chau N, Benamghar L, Lion C, Schwartz F, Vadot J. Oral health in adolescents from a small French town. Community Dent Oral Epidemiol. 1995;23:147–54. doi: 10.1111/j.1600-0528.1995.tb00219.x. [DOI] [PubMed] [Google Scholar]
- 23.Levine M, Brumley RL, Avery KT, Owen WL, Parker DE. Elevated antibody to D-alanyl lipoteichoic acid indicates caries experience associated with fluoride and gingival health. BMC Oral Health. 2002;2:2. doi: 10.1186/1472-6831-2-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kukletova M, Izakovicova Holla L, Musilova K, Broukal Z, Kukla L. Relationship between gingivitis severity, caries experience and orthodontic anomalies in 13-15 year-old adolescents in Brno, Czech Republic. Community Dent Health. 2012;29:179–83. [PubMed] [Google Scholar]
- 25.Karjalainen S, Söderling E, Sewón L, Lapinleimu H, Simell O. A prospective study on sucrose consumption, visible plaque and caries in children from 3 to 6 years of age. Community Dent Oral Epidemiol. 2001;29:136–42. doi: 10.1034/j.1600-0528.2001.290208.x. [DOI] [PubMed] [Google Scholar]