

Abstract
Rheumatoid arthritis (RA) is a chronic, systemic, autoimmune inflammatory disorder that is characterized by joint inflammation, erosive properties and symmetric multiple joint involvement. Temporomandibular joint (TMJ) is very rare to be affected in the early phase of the disease, thus posing diagnostic challenges for the dentist. Conventional radiographs fail to show the early lesions due to its limitations. More recently cone-beam computed tomography (CBCT) has been found to diagnose the early degenerative changes of TMJ and hence aid in the diagnosis of the lesions more accurately. Our case highlights the involvement of TMJ in RA and the role of advanced imaging (CBCT) in diagnosing the bony changes in the early phase of the disease.
Keywords: Cone beam computed tomography, rheumatoid arthritis, temporomandibular joint
Introduction
Rheumatoid arthritis (RA) is an autoimmune disease resulting in persistent inflammatory synovitis, usually involving peripheral joints with a symmetric distribution.[1] The prevalence of RA is 1% worldwide, affecting women more commonly then men in 3:1 ratio and age range between 35 and 45 years.[2,3] Temporomandibular joint (TMJ) is seldom joint to be affected first in the disease course.[3,4] The disease is associated with many clinical signs and symptoms of which pain is a major problem. Limited movements, gelling (joint stiffness), and muscle spasm are also present in the later stages.[2] RA affecting the TMJ presents as a diagnostic challenge to the dentist in the initial stages of disease course.[1] Comprehensive clinical examination along with radiological evaluation is required. Mild bony changes not demonstrated by conventional radiographs are clearly seen by advanced imaging modalities (cone beam computed tomography [CBCT]).
This case report highlights the case of RA with early involvement of TMJ and its classical radiographic findings.
Case Report
A 22-year-old female patient visited the outpatient department with a complaint of pain in the left jaw joint region since 1½ months. On eliciting the history, patient had pain on mastication and difficulty in opening the mouth due to which she was on the soft diet. Medical history revealed that she was diagnosed with RA 6 months back. The patient took homeopathy medicines for 1 month. But presently was not on any medication. On clinical examination of TMJ, the following signs and symptoms were assessed: Left side TMJ was associated with pain, TMJ range of motion was limited, associated with pain while maximum unassisted mouth opening (18 mm) and while lateral excursion [Figure 1], deviation of mandible toward left side while opening mouth was noticed. No clicking sounds on opening, closing and lateral movements. Muscles of mastication were tender on palpation. Intra orally, no teeth were carious, no occlusal prematurity was noticed. On radiological examination, panoramic radiograph depicted irregular erosions in the left condyle and decreased joint space both on right and left side. The findings were of degenerative joint disease but nonspecific due to the overlapping of structures [Figure 2]. TMJ tomography both open and closed mouth revealed slight erosion in the anterior surface of the left condyle but was not clearly appreciated [Figure 3]. Further evaluation was carried out by CBCT.
Figure 1.

Extra oral photograph showing restricted mouth opening
Figure 2.

Orthopantomogram showing no appreciable changes in the left condyle
Figure 3.
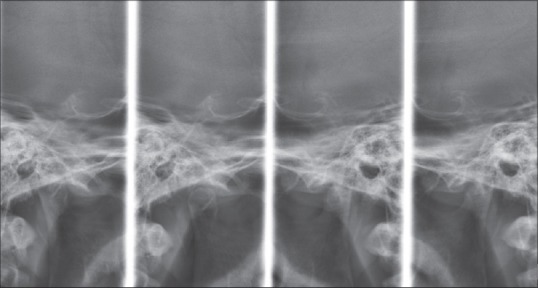
Temporomandibular joint (TMJ) tomogram revealing mild erosions at the anterior condyle of left TMJ
Cone beam computed tomography images revealed sclerosis of the outer surface of the condylar head, narrowing of the articular space bilaterally (more on the left). Coronal left closed mouth view revealed loss of joint space, loss of cortical bone on the superior surface and condylar head erosions compared to right side, which shows normal joint space and condylar structure [Figure 4a and b]. Coronal left open mouth view revealed narrowing of the articular space and erosions on superior head of condyle and right side depicting no changes in the joint space [Figure 5a and b]. Sagittal view open and closed mouth revealed decrease in joint space with erosions of the superior surface of the condyle on the left side [Figures 6a and b, 7a and b]. Hand wrist radiograph revealed the joint space narrowing of the distal phalange of the right thumb, narrowing of 3rd and 4th proximal phalanges and erosion of the middle phalange seen of index finger [Figure 8]. Knee and shoulder joint radiographs revealed no changes. Serum investigations were advised and it revealed rheumatoid factor (RF)-340 IU/ml (normally <40 IU/mL), C-reactive protein (CRP)-368 mg/dl (normally <0.8 mg/dL), erythrocyte sedimentation rate (ESR)-40 mm/h (normally <20 mm/h in females). All serum markers for RA were elevated. Final diagnosis of RA affecting TMJ was arrived at.
Figure 4a.
CBCT coronal view of closed mouth – a) right condyle revealing slight decrease in joint space
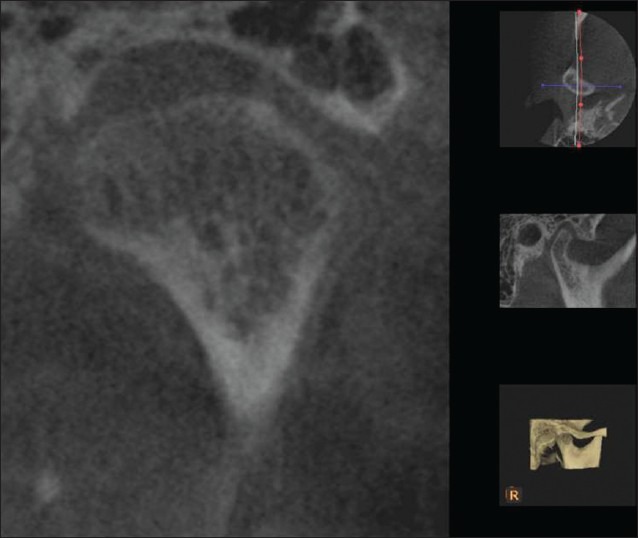
Figure 4b.
Left condyle revealing loss of joint space and severe condylar erosions
Figure 5.

Coronal view of open mouth – (a) right side depictingno changes in the joint space (b) Left side revealing narrowing of the articular space and erosions on superior head of the condyle
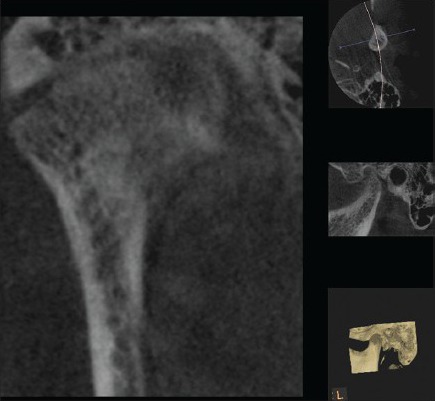
Figure 6.

Sagittal view open mouth: (a) right side depicting nochanges (b) decreased joint space and erosions of the superior surface of the condyle
Figure 7.

Hand wrist radiograph revealing the joint space narrowing of the distal phalange of the right thumb, narrowing of 3rd and 4th proximal phalanges and erosion of the middle phalange seen of index finger
Figure 8.
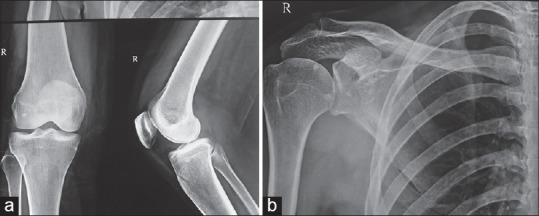
(a) Radiograph of right shoulder joint and knee joint revealing no changes. (b) Radiograph of right shoulder joint and knee joint revealing no changes
Patient was referred to rheumatologist for the further treatment, and she was prescribed Tab Methotrexate 75 mg once a week for 2 months and anti-inflammatory drug twice a day for 15 days and patient responded well to the treatment. Liver function test was also monitored with periodic follow-up. After 2 months of the follow-up, patient reported relief of pain and improvement in mouth opening.
Discussion
Rheumatoid arthritis is systemic inflammatory disease manifesting the synovial membrane of diarthroidal joints.[3] Systemic weight loss, fever, and fatigue may be the first presentation of RA.[1,4] The clinical course of RA may vary from mild joint discomfort of short duration to chronic polyarthritis, pain and gross deformity of joints. Chronic inflammation can lead to a loss of cartilage, erosion and weakness of the bones and muscles, resulting in joint deformity, destruction, and loss of function.[2]
There is no known etiology; however, it is considered multifactorial. Combination of infection, autoimmunity and strong genetic factors are associated with the incidence of RA. Rarely acute injury, surgeries, and trauma are known to initiate RA.[1,3] In the present case, there was no associated family history.
Clinical TMJ involvement is found in 4–80% of RA patients. Most studies indicate that more than 50% of RA patients clinically exhibit TMJ involvement.[3,5] This wide range might be due to different examinations performed, patient's selection, and the use of different criteria for classifying joint involvement.[6,7]
The clinical findings in the TMJ affected with RA are similar to those described for other joints, that is, pain, swelling, movement impairment and crepitation. Malocclusion of the teeth and anterior open bite may occur in advanced stages.[6] Clinically, there is preauricular pain or sensitivity during joint movement. The joints are tender upon pressure, and there is morning stiffness usually lasting more than 30 min and decreased masticatory force.[7] It has been suggested that compression of retrodiscal tissue may be the cause of pain in TMJ. Other suggested causes are inflammatory changes secondary to internal derangement, stretching of the joint capsule and synovitis.[7]
In children, it may result in disturbance in mandibular growth, facial deformity and ankylosis. TMJ ankylosis secondary to RA is generally found in the later stages of the disease, but it is a rare finding and is not well documented.[4,8]
Diagnosis of TMJ involvement with RA is based on history, physical findings, radiographic findings and laboratory values. Hematologically certain abnormal blood antibodies are frequently found in patients with RA like “RF” and “ANA” and raised ESR values. Other confirmatory tests like citrulline antibody and CRP test are recommended in doubtful cases.[1,2,3] Our case showed an elevated level of RF, ESR, CRP.
Radiological examination is useful and important tool for diagnosis and assessment of TMJ disease.[9] Radiographic changes in RA generally do not appear in the early phase of the disease. The reported incidence of findings on conventional radiographs of the TMJ in RA patients varies from 19% to 86%.[3,4] Destruction of the TMJ in RA patients is correlated to the severity and duration of the disease. Previously, it has been noted that the initial radiographic findings are not readily visible with panoramic radiographs due to its limitations of overlapping and distortions, this is reemphasized by the present report. The radiographic changes of TMJ includes flattening of the mandibular head, cortical erosion, gradual decrease in joint space due to granulation, deossification, pencil head or spiked deformity of the condylar head and sub cortical cysts.[6,7,8] The diagnostic imaging techniques used for RA include extraoral radiography, CT, magnetic resonance imaging, arthrography and arthrotomography.[3] More recently, CBCT has been the object of study for TMJ evaluation by various authors who consider it the best-recommended imaging modality for the degenerative diseases of TMJ.[10]
The severity of the radiographic changes is graded according to Larsen's classification into six grades (0–V) based on the radiographic appearance: 0: Normal, I: Slight abnormality, joint space is slight narrow, II: Early abnormality, joint space is slightly narrow, with erosion, III-moderate destruction, joint space is narrow and eroded, IV-severe destruction, joint space is narrow, with erosions and bone deformity, V-mutilating abnormality, disappearance of joint space, with erosion and bone deformity.[11]
The present case corresponded to grade III, since there were joint space narrowing and loss of cortical bone on the superior surface and erosions of the condylar head.
Though the treatment of RA is complex, multidisciplinary and noncurative, the goal is to maintain function, and to prevent joint and organ damage until the disease enters remission. Two classes of medications are used in treating RA: Fast-acting “first-line drugs” and slow-acting “second-line drugs” (also referred to as disease-modifying anti-rheumatic drugs). The first-line drugs, such as aspirin and cortisone, are used to reduce pain and inflammation. The slow-acting second-line drugs, such as methotrexate, and hydroxychloroquine promote disease remission and prevent progressive joint destruction, but they are not anti-inflammatory agents. Some newer “second-line” drugs for the treatment of RA include leflunomide and the “biologic” medications etanercept, infliximab, rituximab, and abatacept.[1,9,10]
There is no good evidence of long-term benefit of physiotherapy, but it can be used in the short-term to manage restricted mouth opening or after arthroscopy or open surgery. NSAIDs are indicated for pain secondary to inflammation. Joint pain can be temporarily relieved by injection of local anesthetic into the joint space, and pain relief suggests that arthroscopy may be considered as a therapeutic and diagnostic aid.[12,13,14,15]
The involvement of TMJ in RA usually correlates well with the radiographic damage of the joints in the hands and feet. The present case was initial case of RA with the duration of disease less than a year, and TMJ was primarily involved along with few appreciable changes in hand wrist X-ray. In the early phases, conventional radiographs are compromised due to their limitations. The recent imaging modality, CBCT reveals early degenerative changes in the TMJ more accurately and hence can aid in timely diagnosis and management of this debilitating degenerative disease.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Chitroda P, Katti G, Ghali S. Bilateral TMJ involvement in rheumatoid arthritis, a case report. J Oral Health Res. 2011;12:74–8. [Google Scholar]
- 2.Milind P, Sushila K. How to live with rheumatoid arthritis. Int Res J Pharm. 2012;3:115–21. [Google Scholar]
- 3.Delantoni A, Spyropoulou E, Chatzigiannis J, Papademitriou P. Sole radiographic expression of rheumatoid arthritis in the temporomandibular joints: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:e37–40. doi: 10.1016/j.tripleo.2005.12.024. [DOI] [PubMed] [Google Scholar]
- 4.Seymour RL, Crouse VL, Irby WB. Temporomandibular ankylosis secondary to rheumatoid arthritis. Report of a case. Oral Surg Oral Med Oral Pathol. 1975;40:584–9. doi: 10.1016/0030-4220(75)90367-9. [DOI] [PubMed] [Google Scholar]
- 5.Paiva FM, Maria E, Cesar R. Treatment of temporomandibular disorders in children: Summary statements and recommendations. American Academy of Pediatric Dentistry University of Texas Health. Science Center at San Antonio Dental School. J Am Dent Assoc. 1990;120:265–9. [PubMed] [Google Scholar]
- 6.Scutellari PN, Orzincolo C. Rheumatoid arthritis: Sequences. Eur J Radiol. 1998;27(Suppl 1):S31–8. doi: 10.1016/s0720-048x(98)00040-0. [DOI] [PubMed] [Google Scholar]
- 7.Goupille P, Fouquet B, Cotty P, Goga D, Valat JP. Direct coronal computed tomography of the temporomandibular joint in patients with rheumatoid arthritis. Br J Radiol. 1992;65:955–60. doi: 10.1259/0007-1285-65-779-955. [DOI] [PubMed] [Google Scholar]
- 8.Helenius LM, Hallikainen D, Helenius I, Meurman JH, Könönen M, Leirisalo-Repo M, et al. Clinical and radiographic findings of the temporomandibular joint in patients with various rheumatic diseases. A case-control study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99:455–63. doi: 10.1016/j.tripleo.2004.06.079. [DOI] [PubMed] [Google Scholar]
- 9.Kobayashi R, Utsunomiya T, Yamamoto H, Nagura H. Ankylosis of the temporomandibular joint caused by rheumatoid arthritis: A pathological study and review. J Oral Sci. 2001;43:97–101. doi: 10.2334/josnusd.43.97. [DOI] [PubMed] [Google Scholar]
- 10.Wenneberg B, Kopp S, Hollender L. The temporomandibular joint in ankylosing spondylitis. Correlations between subjective, clinical, and radiographic features in the stomatognathic system and effects of treatment. Acta Odontol Scand. 1984;42:165–73. doi: 10.3109/00016358408993868. [DOI] [PubMed] [Google Scholar]
- 11.Tabeling HJ, Dolwick MF. Rheumatoid arthritis: Diagnosis and treatment. Fla Dent J. 1985;56:16–8. [PubMed] [Google Scholar]
- 12.Littman H, Grieder A. Medical and dental coordination in juvenile rheumatoid arthritis. Ann Dent. 1985;44:32–4. [PubMed] [Google Scholar]
- 13.Helms A, Kaplan P. Diagnostic imaging of the temporomandibular joint: Recommendations for use of the various techniques. Am J Radiol. 1990;154:319–22. doi: 10.2214/ajr.154.2.2105023. [DOI] [PubMed] [Google Scholar]
- 14.Sidebottom AJ, Salha R. Management of the temporomandibular joint in rheumatoid disorders. Br J Oral Maxillofac Surg. 2013;51:191–8. doi: 10.1016/j.bjoms.2012.04.271. [DOI] [PubMed] [Google Scholar]
- 15.Moore RA, Tramèr MR, Carroll D, Wiffen PJ, McQuay HJ. Quantitative systematic review of topically applied non-steroidal anti-inflammatory drugs. BMJ. 1998;316:333–8. doi: 10.1136/bmj.316.7128.333. [DOI] [PMC free article] [PubMed] [Google Scholar]