

Abstract
Background:
Early childhood caries (ECC) is a severe form of dental decay with multi-factorial origin.
Objectives:
The aim of this cross-sectional study was to determine the prevalence and related risk factors of ECC among preschool children residing in rural and urban areas of Trivandrum district in Kerala.
Methods:
A sample size of 1329 preschool children of <60 months of age was randomly selected from rural and urban areas of Trivandrum and decayed missing filled teeth indices were recorded. A standardized questionnaire was distributed to the parents. The data were subjected to SPSS version 16 and statistically analyzed with Chi-square test.
Results:
Prevalence of ECC in the study sample was found to be 54%. Furthermore, a positive association was obtained between ECC and age of the child, location of residence, dietary habits, and oral hygiene habits.
Conclusion:
There is an urgent need to implement preventive and curative oral health programs for preschool children in rural and urban areas.
Keywords: Early childhood caries, oral hygiene habits, preschool, syrupy medications, working status of mothers
Introduction
Dental caries is considered, the most common ignored chronic disease among children. In 2003, the American Academy of Pediatric Dentistry defined early childhood caries (ECC) as the presence of one or more decayed (noncavitated or cavitated), missing (due to caries), or filled tooth surfaces in any primary tooth in a child up to 71 months of age or younger.[1] The factors responsible for ECC include a susceptible host, fermentable carbohydrate diet, presence of dental plaque, a high number of cariogenic microorganisms such as Streptococcus mutans, Lactobacillus, and most importantly, time.[2] Dietary habits, socioeconomic status, working status of mother, oral hygiene habits, and frequent intake of medications are certain risk factors for this condition.[3,4]
Early childhood caries is considered as a serious public health problem as it is a complex disease of primary dentition which relay serious socio-behavioral issues that afflict mainly the infants and toddlers.[5,6] ECC, if left untreated, the deleterious effects are pain, compromised chewing ability, malocclusion, phonetic problems, sub-optimal health, lower self-esteem. Hence, ECC is a social, political, behavioral, medical, psychological, economical, and dental problem that affects the quality-of-life.[7,8]
The prevalence rate of ECC is low in the developed countries of Europe and USA.[9] In far East Asia, the prevalence and severity for ECC in 3-year-old ranged from 36% to 85%.[10,11]
In India, a fluctuant prevalence rate is found over the years. It varied from 55.5% in 1940 to 68% in 1960s.[12] Despite the preventive measures and awareness, the prevalence rate of ECC is steadily increasing in our country. Few studies conducted in Kerala showed high prevalence rate.[1] One of the significant studies conducted by Kuriakose and Joseph in 1999, the results showed an astonishing caries prevalence of 57%.[13] According to a study conducted in Brazil (2014) among 320 preschool children, the prevalence was 20%.[14]
The present study is an effort to determine the prevalence rate of ECC and evaluate its associated risk factors among preschool children of rural and urban areas of Trivandrum district.
Methods
The study group consisted of 1329 preschool children of <60 months of age from various Anganwadi centers, government aided day care centers and private owned kindergartens in rural and urban areas of Trivandrum district in Kerala. Institutional Ethical Committee clearance [IEC/012/2014] was obtained, and the consent for examining the children was procured from concerned authorities before the commencement of the study.
All the children from these preschools who were cooperative, in the age of 2–5 years and accompanied by their parent were included in the study. Exclusion criteria comprised of those children with developmental enamel defects and systemic diseases.
Clinical examination was done using a mouth mirror, and a probe was only used when in doubt with minimal pressure to remove debris, under sterile conditions. The decayed missing filled teeth (dmft) indices (dmft, Greubbell, 1944) were recorded and treatment cards were issued for those children who required treatments.
Questionnaires were distributed among all parents, in regional language to avoid linguistic barriers. It contained questions about socioeconomic, demographic data, dietary and oral hygiene habits of children. These questionnaires were collected, and data were analyzed.
Statistical analysis
The data were subjected SPSS version 16 (SPSS Inc. ChicagoIII. USA). The association of variables was obtained by Chi-square test at 0.01 and 0.05 significant levels.
Results
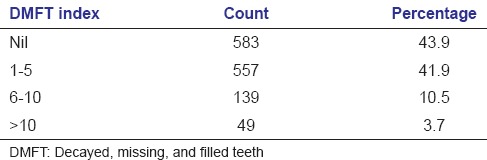
Of the total 1329 children, 3.9% were of 1–2 years, 22.4% were 3 years old, 41.1% were 4 years old, and 32.6% were of 5 years of age. Out of the children examined, 45.9% were male and rest female children. Only 45.9% of the sample population were caries free. Table 1 shows the distribution of sample according to decayed teeth. The study population was almost equally distributed among rural and urban areas (rural – 50.1% and urban – 49.9%). Frequency of caries among children was assessed using dmft index, percentage distribution is shown in Table 2. About 47.1% of the sample were children of working mothers.
Table 1.
Percentage distribution of the sample according to number of decayed teeth
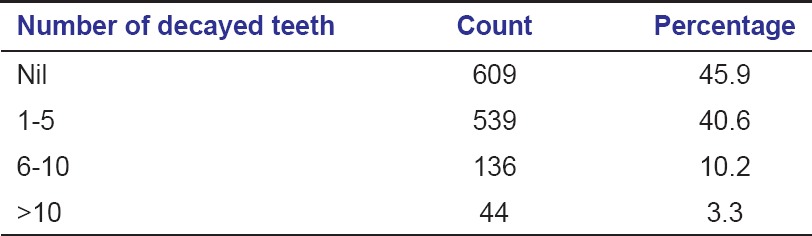
Table 2.
Percentage distribution of the sample according to dmft index
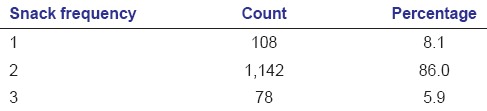
About 66% of the total children had oral rinsing habit after every meal. 52.1% of children took syrupy medications for various illnesses. Frequency of snacking in children is shown in Table 3. Half of the sample population preferred sticky foods (50%). Only a meager 17% of the children used to brush twice daily, and 11.1% had a history of previous dental visits.
Table 3.
Percentage distribution of the sample according to snack frequency
Association of factors such as sex, location of residence, and working status of mothers with the frequency of dental caries is shown in Table 4. Association with each variable was seen to be statistically significant at 0.05, 0.01, and 0.01 levels, respectively. Correlation between working status of mothers and oral hygiene habits is given in Table 5. Table 6 shows the association of previous dental visit with oral hygiene habits of children.
Table 4.
Association of sex, location, and working status of the mother with dental caries frequency
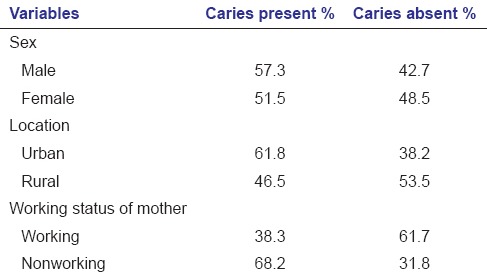
Table 5.
Association of working status of the mother with oral hygiene habit
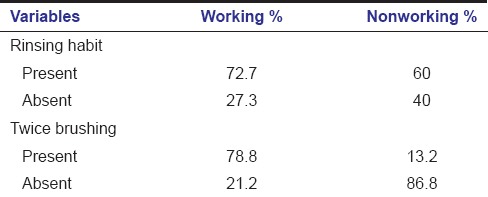
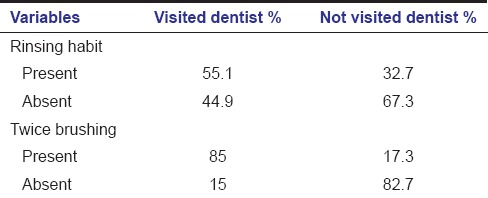
Table 6.
Association of previous dental visit of the child with oral hygiene habits
Of the 876 students with rinsing habits after meals, caries was noticed in 45.2% in contrast to 71.5% prevalence among the 453 students without rinsing. Dental caries was seen in 65.8% of 692 students who took syrupy medicines for various illnesses, whereas it was only 41.5% among those who did not. Among the 147 students who had previously visited dentists, caries was found in 70.7%.
Figure 1 shows the relation between dental caries and the snacking frequency in children. Dental caries was seen to rise in those with increased snacking frequency. The association between sticky food preference of children and dental caries is depicted in Figure 2. Caries was more prevalent in children who preferred sticky foods over fibrous foods. Figure 3 shows that there is a reduction in caries prevalence among those children who brushed their teeth twice daily.
Figure 1.
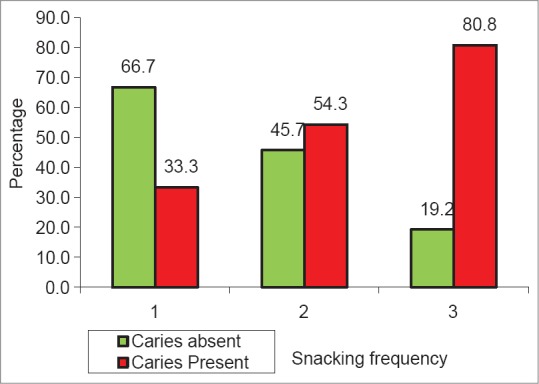
Snacking frequency and dental caries
Figure 2.
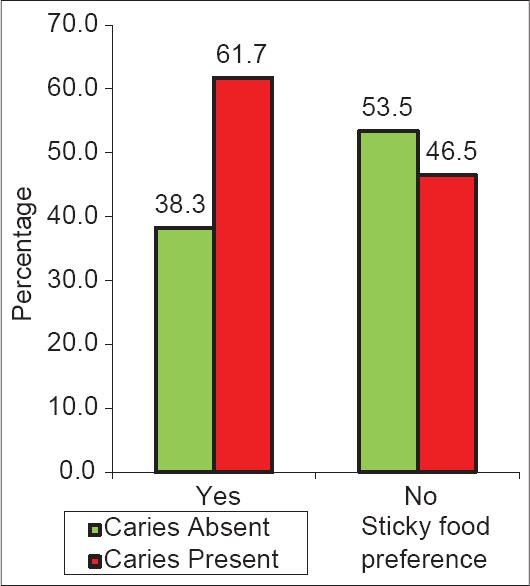
Sticky food preference and dental caries
Figure 3.
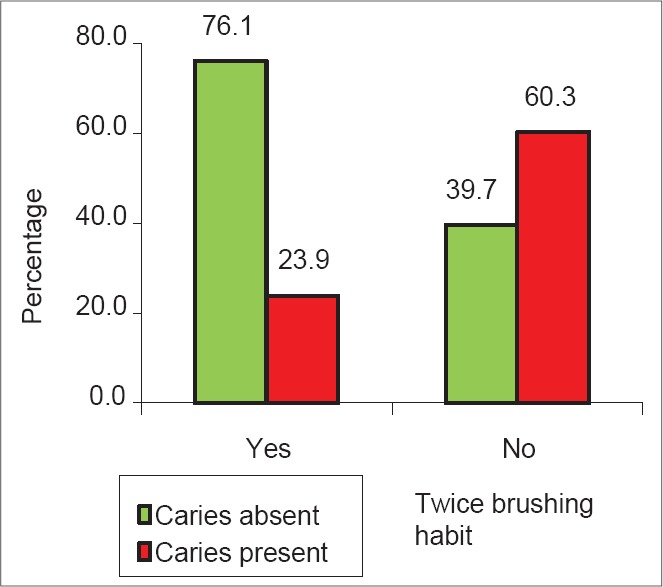
Twice brushing habit and dental caries
Discussion
Early childhood caries is a prevalent and common disease of childhood. Infants and toddlers are most affected by this condition as they are mostly dependent on their parents or caregivers for diet and oral hygiene methods.
A total of 1,329 children of <60 months was screened to determine the prevalence of ECC from the randomly selected kindergarten schools from government, government-aided, and private managements in the rural and urban areas of Trivandrum district.
The prevalence of ECC in the present study was 54%. The prevalence reported in Western countries is varied. The mean deft found in Karnataka (Bangalore), Andhra Pradesh, and Kerala were 0.6, 1.63, and 2.1, respectively.[15] In Kerala, the prevalence studies of this age group were comparatively less. We got a mean dmft of 2.3 ± 3.2 (mean ± standard deviation) in comparison with previous studies.[6] Our study showed an increased prevalence rate in spite of preventive methods and dental accessibility.
Determining the prevalence rate of caries in preschool children is a difficult process as the children of this age group are not easily accessible and are uncooperative.[16] Caries prevalence was seen to increase with age, which is in accordance with previous studies.[17] As children grow older, change in their dietary habits and oral hygiene practices pose a greater cariogenic challenge.
Male children are more affected than female children. This could probably be due to the fact that male children are more favored in the Indian communities and that can also be associated with increased an physical activity, that instigates the increase in demand for more food when compared to females. Children from rural areas were more affected than their urban counterparts. This could probably be due to the poor access to dental care in these areas and lack of awareness to this problem.
Hygiene habits of preschool children are modeled by family behavior particularly maternal behavior which is related to the caries prevalence in their children. An association was found between caries incidence and education status of the parent in our study. This may be attributed to the lack of information and education about the oral health care for children among uneducated mothers.[18] Decreased awareness among parents of rural children regarding oral health regime should be one of the factors that have influenced the disease process since our study reported greater number of carious teeth.
In this present study, 52.9% of mothers were found to be nonworking. 68.2% of children with working mothers were caries affected. Hence, a strong association was found between the working status of mother and dental caries, which corroborates with previous studies.
The study also highlighted a strong association between oral hygiene practices and the working status of the mother. The children of working mothers had a habit of rinsing after meals, and brushed their teeth twice regularly than others. This can be due to better care and education from preschool and accessibility of early dental care.
The present study supports earlier studies which state that frequent consumption of foods, snacks, and drinks in-between meals increases the risk for caries. There was a significant association between carious lesions and consumption of in-between meal snacks. In this study, those who consumed snacks three and more times had more carious lesions (80%). Hence, limiting snacking time together with an emphasis on the quality of snacks is essential. Furthermore, the association was found between sticky food preferences of the child with dental caries. 61.7% children were caries affected, who preferred sticky food, which is in accordance with previous studies.[19] Proper diet counseling should include detergent foods and foods rich in antioxidants.
Nutritional supplements and dietary factors have a profound and lasting effect on the developing and developed dentition. Sugary base containing syrupy medicines have a reverse effect. It is proven that the prolonged use of this medicine results in dental caries. Viscosity and pH are other risk factors in these medicines.[20] In our study, children who were on syrupy medicines for prolonged time were more caries affected (65.7%) than those who were not. This suggests that a careful inspection of the labels in medicines regarding sugar content should be undertaken prior to prescription of these drugs. Steps should be undertaken to educate the general physician and pediatricians regarding the ill effects of more palatable syrupy medicines.
We found an important correlation between the oral hygiene habits and dental caries as well. Preschool children neither understand nor have the manual dexterity to maintain good oral hygiene. Parental assistance and guidance are essential to reduce the risk of developing caries. There is a need for prolonged parental participation in the cleaning of preschool children's teeth. In this study, we found 76.1% of children having brushing habit twice a day, were caries free.
We also observed that those children with previous dental visits had a more complaints of dental caries when compared to their peers who did not visit. This calls for an effective and efficient patient as well as parent education regarding oral health care and preventive strategies which can be easily implemented during initial visits that may eventually reduce the caries incidence.
Since India is a developing country, the preponderance of infectious diseases limits the available health services to fund the treatment needs in the dental field. Many of our attitudes and habits concerning food and health are acquired in early childhood.
Conclusion
Early childhood caries is a morbid condition that is difficult to treat in infants and very young children. This study emphasizes a relatively high dental caries prevalence rate of 54%. Our study sirens the call for an urgent need to implement preventive and curative oral health programs for preschool children in our society. Furthermore, the present preventive programs are inadequate to minimize the population affected by this infectious disease. A more effective and acceptable prevention program should be implemented during the baby steps of a child's life. The importance of first dental visit, diet counseling, and proper oral care methods should be stringently advocated to expectant parents, new parents and preschool teachers and caregivers to inculcate lasting oral health attitudes among children.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.American Academy of Pediatric Dentistry. Reference manual 2002-03. Policies on early childhood caries; Unique challenges and treatment options. Pediatr Dent. 2003;23:24–5. [Google Scholar]
- 2.Ripa LW. Nursing caries: A comprehensive review. Pediatr Dent. 1988;10:268–82. [PubMed] [Google Scholar]
- 3.Curzon ME, Preston AJ. Risk groups: Nursing bottle caries/caries in the elderly. Caries Res. 2004;38(Suppl 1):24–33. doi: 10.1159/000074359. [DOI] [PubMed] [Google Scholar]
- 4.Quinonez R, Santos RG, Wilson S, Cross H. The relationship between child temperament and early childhood caries. Pediatr Dent. 2001;23:5–10. [PubMed] [Google Scholar]
- 5.Postma TC, Ayo-Yusuf OA, van Wyk PJ. Socio-demographic correlates of early childhood caries prevalence and severity in a developing country – South Africa. Int Dent J. 2008;58:91–7. doi: 10.1111/j.1875-595x.2008.tb00182.x. [DOI] [PubMed] [Google Scholar]
- 6.Jose B, King NM. Early childhood caries lesions in preschool children in Kerala, India. Pediatr Dent. 2003;25:594–600. [PubMed] [Google Scholar]
- 7.Kagihara LE, Niederhauser VP, Stark M. Assessment, management, and prevention of early childhood caries. J Am Acad Nurse Pract. 2009;21:1–10. doi: 10.1111/j.1745-7599.2008.00367.x. [DOI] [PubMed] [Google Scholar]
- 8.Casamassimo PS, Thikkurissy S, Edelstein BL, Maiorini E. Beyond the dmft: The human and economic cost of early childhood caries. J Am Dent Assoc. 2009;140:650–7. doi: 10.14219/jada.archive.2009.0250. [DOI] [PubMed] [Google Scholar]
- 9.Milnes AR. Description and epidemiology of nursing caries. J Public Health Dent. 1996;56:38–50. doi: 10.1111/j.1752-7325.1996.tb02394.x. [DOI] [PubMed] [Google Scholar]
- 10.Tsai AI, Chen CY, Li LA, Hsiang CL, Hsu KH. Risk indicators for early childhood caries in Taiwan. Community Dent Oral Epidemiol. 2006;34:437–45. doi: 10.1111/j.1600-0528.2006.00293.x. [DOI] [PubMed] [Google Scholar]
- 11.Douglass JM, Wei Y, Zhang BX, Tinanoff N. Caries prevalence and patterns in 3-6-year-old Beijing children. Community Dent Oral Epidemiol. 1995;23:340–3. doi: 10.1111/j.1600-0528.1995.tb00259.x. [DOI] [PubMed] [Google Scholar]
- 12.Newdelhi: ICMR; 1994. Oral health ICMR bulletin; p. 24. [Google Scholar]
- 13.Kuriakose S, Joseph E. Caries prevalence and its relation to socio-economic status and oral hygiene practices in 600 pre-school children of Kerala-India. J Indian Soc Pedod Prev Dent. 1999;17:97–100. [PubMed] [Google Scholar]
- 14.dos Santos Junior VE, de Sousa RM, Oliveira MC, de Caldas Junior AF, Rosenblatt A. Early childhood caries and its relationship with perinatal, socioeconomic and nutritional risks: A cross-sectional study. BMC Oral Health. 2014;14:47. doi: 10.1186/1472-6831-14-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Johnson NW. Cambridge: Cambridge University Press; 1991. Dental Caries: Markers of High and Low Risk Groups and Individuals. [Google Scholar]
- 16.Damle SG. Pediatric Dentistry. New Delhi: Arya Publishing House; 2002. Epidemiology of dental caries in India; pp. 75–96. [Google Scholar]
- 17.Sudha P, Bhasin S, Anegundi RT. Prevalence of dental caries among 5-13-year-old children of Mangalore city. J Indian Soc Pedod Prev Dent. 2005;23:74–9. doi: 10.4103/0970-4388.16446. [DOI] [PubMed] [Google Scholar]
- 18.Suresh BS, Ravishankar TL, Chaitra TR, Mohapatra AK, Gupta V. Mother's knowledge about pre-school child's oral health. J Indian Soc Pedod Prev Dent. 2010 Dec 28;:282–7. doi: 10.4103/0970-4388.76159. [DOI] [PubMed] [Google Scholar]
- 19.Huew R, Waterhouse P, Moynihan P, Kometa S, Maguire A. Dental caries and its association with diet and dental erosion in Libyan schoolchildren. Int J Paediatr Dent. 2012;22:68–76. doi: 10.1111/j.1365-263X.2011.01170.x. [DOI] [PubMed] [Google Scholar]
- 20.Subramaniam P, Nandan N. Cariogenic potential of pediatric liquid medicaments – An in vitro study. J Clin Pediatr Dent. 2012;36:357–62. doi: 10.17796/jcpd.36.4.nt11584612462t84. [DOI] [PubMed] [Google Scholar]