

Abstract
Background.
Platinum plus etoposide is the standard therapy for extensive-stage small cell lung cancer (ES-SCLC) and is associated with significant myelosuppression. We hypothesized that the combination of carboplatin and nanoparticle albumin-bound paclitaxel (nab-paclitaxel) would be better tolerated. We investigated carboplatin with nab-paclitaxel on every-3-week and weekly schedules.
Methods.
This noncomparative randomized phase II trial used a two-stage design. The primary objective was objective response rate, and secondary objectives were progression-free survival, overall survival, and toxicity. Patients with ES-SCLC and an Eastern Cooperative Oncology Group performance status ≤2 and no prior chemotherapy were randomized in a 1:1 ratio to arm A (carboplatin area under the curve [AUC] of 6 on day 1 and nab-paclitaxel of 300 mg/m2 on day 1 every 3 weeks) or arm B (carboplatin AUC of 6 on day 1 and nab-paclitaxel 100 mg/m2 on days 1, 8, and 15 every 21 days). Response was assessed after every two cycles.
Results.
Patients required frequent dose reductions, treatment delays, and omission of the weekly therapy. The trial was closed because of slow accrual.
Conclusion.
Carboplatin and nab-paclitaxel demonstrated activity in ES-SCLC but required frequent dose adjustments.
Author Summary
Discussion
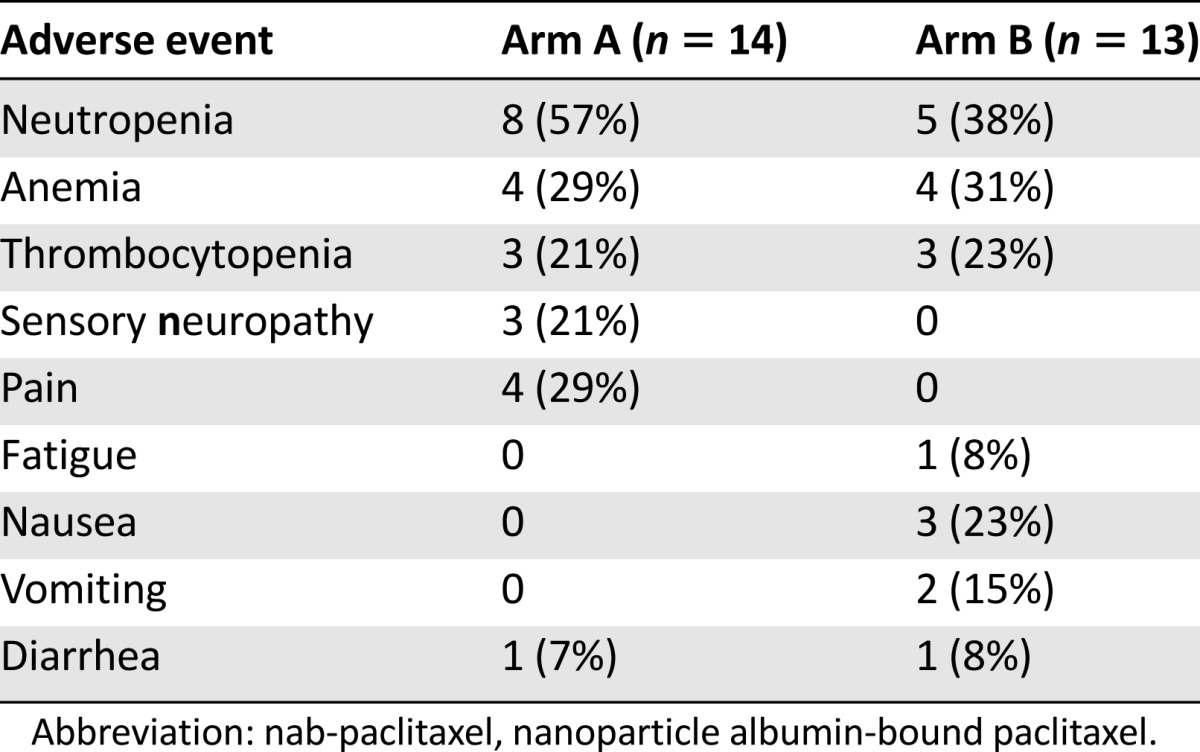
Based on trials of single-agent nanoparticle albumin-bound paclitaxel (nab-paclitaxel; Abraxane; Celgene Corp, Summit, NJ, http://www.celgene.com) in metastatic breast cancer and of carboplatin and nab-paclitaxel in patients with advanced solid tumors and in advanced non-small cell lung cancer (NSCLC), we expected this combination to have similar efficacy and better tolerability than platinum plus etoposide [1–3]. However, a significant number of patients in both arms required dose reductions and/or dose delays and, in the weekly arm, omission of day 8 or 15. The trial was amended, and the dose of nab-paclitaxel was reduced to 240 mg/m2 every week in arm A and to 80 mg/m2 on days 1, 8, and 15 every 21 days in arm B. The trial was closed because of slow accrual before the impact of the dose reduction on toxicity and treatment compliance could be assessed. The grade 3 or 4 adverse events are presented in Table 1. Both arms of the trial would have met the criteria to proceed to the second stage of the two-stage design, but no further assessment of efficacy could be made because of the small sample size.
Table 1.
Grade 3 or 4 adverse events observed with carboplatin and every-3-week nab-paclitaxel (arm A) and carboplatin and weekly nab-paclitaxel (arm B)
The current standard of platinum and etoposide has been the treatment standard for extensive-stage SCLC. The median survival observed in clinical trials in the U.S. is 9–10 months, and outside the context of clinical trials, the median survival observed is ∼6 months [3–6]. Consequently, there is a desperate need for novel therapies, and the closure of the trial because of slow accrual was disappointing. Approximately 40% of patients with SCLC are aged ≥70 years, and many patients have significant cardiovascular and/or pulmonary comorbidities related to prolonged tobacco use [4]. Historically, elderly patients have been underrepresented in clinical trials, and many times, the organ function and restrictions related to comorbidities limit enrollment to the fit elderly [7]. Future trials should incorporate a geriatric assessment to assess the impact of comorbidities and age on treatment outcome and toxicity.
The safety of chemotherapy combinations in one patient population or disease often leads to the assumption that the combination will be safe in other diseases or patient populations. This trial illustrates the need for prospective trials in disease-specific patient populations because a multitude of known and unknown factors contribute to the tolerability of treatments.
Supplementary Material
Footnotes
For Further Reading: Makoto Maemondo, Akira Inoue, Shunichi Sugawara et al. Randomized Phase II Trial Comparing Carboplatin Plus Weekly Paclitaxel and Docetaxel Alone in Elderly Patients With Advanced Non-Small Cell Lung Cancer: North Japan Lung Cancer Group Trial 0801. The Oncologist 2014;19:352–353.
Abstract:
Background. Standard first-line chemotherapy for elderly non-small cell lung cancer (NSCLC) patients has been monotherapy with vinorelbine or gemcitabine. Docetaxel has also been considered as an alternative option for the elderly population in Japan. We have previously demonstrated the high efficacy of carboplatin plus weekly paclitaxel for elderly NSCLC patients. Consequently, we conducted a randomized phase II study to select the proper regimen for a future phase III trial.
Methods. Eligible patients were aged 70 years or older with newly diagnosed advanced NSCLC. Patients were randomly assigned either to a combination of carboplatin (area under the curve: 6 mg/mL per minute) with weekly paclitaxel (70 mg/m2) (CP regimen) or to single-agent docetaxel (60 mg/m2). The primary endpoint of this study was objective response rate. Secondary endpoints were progression-free survival, overall survival, and toxicity profile.
Results. Among 83 eligible patients (41 to CP, 42 to docetaxel), the objective response rates were 54% (95% confidence interval: 39%–69%) and 24% (95% confidence interval: 11%–37%) and median progression-free survival was 6.6 months and 3.5 months in the CP arm and the docetaxel arm, respectively. Severe neutropenia, febrile neutropenia, and nausea were significantly frequent in the docetaxel arm, whereas toxicities in the CP arm were generally moderate. One treatment-related death was observed in the docetaxel arm.
Conclusion. The CP regimen achieved higher activity with less toxicity than single-agent docetaxel. Considering the results of this phase II trial and the IFCT-0501 trial, we have selected the CP regimen for a future phase III trial in elderly patients with advanced NSCLC.
Access the full results at: Stinchcombe-14-327.theoncologist.com
ClinicalTrials.gov Identifier: NCT00454324
Sponsor(s): Abraxis Oncology
Principal Investigator: Thomas E. Stinchcombe
IRB Approved: Yes
Author disclosures and references available online.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.