

Abstract
A 76-year-old man with known situs inversus totalis presented with left-sided discomfort. Abdominal ultrasonography and CT scan confirmed the diagnosis of a gallstone, as well as, situs inversus; the liver and gallbladder on the left side and the spleen on the right. The biliary system was thought to be left-right reversal, mirror image in the view of drip infusion cholangiogram and MRI. Laparoscopic cholecy stectomy was safely performed, despite of unexpected aberrant cystic artery running inferior to cystic duct of situs inversus. Laparoscopic surgeon should be careful for view of reversed relationships and also existence of other anomalies.
Keywords: Situs inversus totalis, Laparoscopic cholecy-stectomy, Inferior cystic artery
INTRODUCTION
Recently, laparoscopic cholecystectomy has become the standard technique for surgical removal of the gallbladder for symptomatic gallstones[1-3]. Situs inversus totalis is uncommon anatomic anomaly, with gallbladder on the left side. Some investigators reported that laparoscopic cholecystectomy was successfully applied in situs inversus totalis, but the patients of all these cases were without other additional anomaly. We recently encountered a patient in situs inversus, who had anomaly of the cystic artery with symptomatic gallstones and was managed by laparoscopic cholecystectomy.
CASE REPORT
A 76-year-old man, who was known to have situs inversus, was seen complaining of recurrent left-sided upper quadrant abdominal pain for 2 mo. Abdominal ultrasound and CT scan confirmed the solitary radiolucent gallstone and presence of chronic gallbladder wall inflammation as well as situs inversus with the liver and gallbladder on the left side and the spleen on the right. The cardiac shadow and stomach bubble were displayed on the right side of the chest roentgenogram. The endoscopic retrograde cholangio-pancreatography (ERCP) was performed, but it was too difficult to perform cholangiography (Figure 1A). The ERCP revealed the right sided pancreatic duct. Three dimensional (3D) drip infusion cholangiogram (DIC)-CT and magnetic resonance cholangio-pancreatography (MRCP) revealed the right-left reversal biliary system (Figures 1B and C). We did not perform the abdominal angiography before operation. All the preoperative examinations we performed revealed the mirror image anatomy without additional anomaly. Unexpected aberrant cystic artery was encountered as predicted by preoperative ultrasonography, CT, and MRCP.
Figure 1.
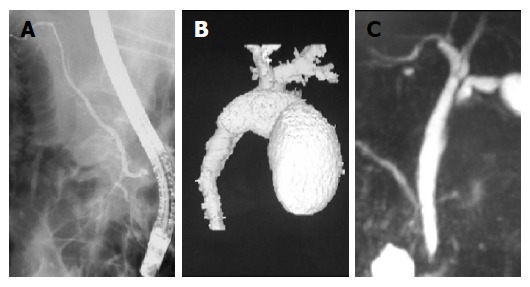
Reversed cholangiopancreatograms. A: ERCP; B: 3D-DIC CT; C: MRCP.
OPERATION
At first, small laparotomy was placed in the sub-umbilical portion, and a 10-mm trocar with a balloon was inserted into the abdominal cavity. A 10-mm trocar was placed in the sub-xiphoid locations, and two 5-mm trocars were placed in the left sub-costal and left lateral regions under the view of laparoscope (Figure 2). The surgeon mainly used the forceps inserted through the trocar of sub-xiphoid. By laparoscopic view of left upper abdomen, gallbladder was placed on the left side and hepatic round ligament on the right (Figure 3A). We grasped and tracted the fundus of gallbladder and the cord was revealed lying inferior to the cystic duct by dissection of Calot’s triangle (Figures 3B and C). The whole of the cystic duct was revealed by the dissection of the surroundings of the cystic duct after the traction of the cord (Figure 3D). We performed clip ligature and cut the cystic duct (Figure 3E). After cystic duct had been ligated, more dissection of the neck of the gallbladder was done and it revealed that the cord lead only to the gallbladder (Figure 3F). We thought that the cord was the cystic artery that was not placed on the mirror image of normal position. We performed the clip ligature and cut the cord. Finally the gallbladder was dissected and removed as usual.
Figure 2.
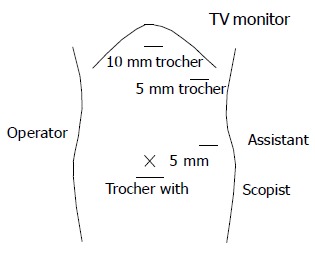
Arrangement around the operating table and positions of the trocars.
Figure 3.
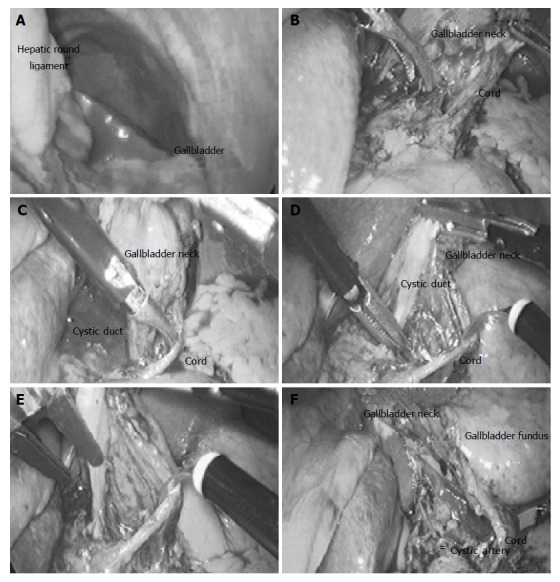
Laparoscopic view during cholecystectomy. A: Gallbladder was placed on the left side and hepatic round ligament on the right; B: the fundus of gallbladder was grasped and tracted; C: the cord was revealed lying inferior to the cystic duct; D: the surroundings of the cystic duct were dissected after the cord was tracted; E: the cystic duct was cut after the clip ligature; F: the cord lead only to the gallbladder.
DISCUSSION
Situs inversus viscerum is a rare condition, occurring in 1:5 000-1:10 000 hospital admissions[4]. As reported by Sato et al laparoscopic observations were performed in 1 802 consecutive patients and situs inversus was investigated in 0.2%[5]. Because the number of laparoscopic cholecystectomy recently becomes large, the reports of that of in situ inversus totalis have been increasing[6-15]. Ten cases of laparoscopic cholecystectomy in situs inversus totalis were reported.
In all reports, in which we can investigate about anatomy of cystic artery[6-10,12-15], it is reported that the cystic artery runs with the mirror image against normal patient. According to the report described by Hugh et al[16], the cystic artery arises as a branch of the right hepatic artery within the hepato-biliary triangle and runs immediately cephalic to the cystic duct toward the gallbladder in 70-80% of patients without situs inversus totalis. It is also reported that “Inferior” cystic artery arises outside the hepatobiliary triangle, runs ventral to the bile duct and lies inferior to the cystic duct in 6% of the patients. We thought that the cystic artery in our case is the mirror image of this anomaly. Because we did not perform the angiography, the anomalies of hepatic artery and cystic artery cannot be revealed indeed. However, we successfully and safely performed laparoscopic cholecystectomy in our case. According to consideration of our case, the angiography may be done in situs inversus totalis.
Since we carefully operated under the laparoscopic view and cut the cord recognized as the cystic artery, we have successfully carried out laparoscopic cholecystectomy in the patient with situs inversus totalis, despite the reversed anatomic relationships and other arterial anomaly. In the future, the frequency of anomalies of cystic artery detected in situs inversus totalis will increase under the laparoscopic cholecystectomy. In conclusion, we suggest that the experienced laparoscopic surgeons can successfully perform laparoscopic cholecystectomy in situs inversus totalis with care for the reversed relationships and possible existence of other anomalies.
Footnotes
Science Editor Guo SY Language Editor Elsevier HK
References
- 1.Lüdtke FE, Lepsien G, Neufang T, Peiper HJ. New trends in biliary surgery. Zentralbl Chir. 1994;119:362–370. [PubMed] [Google Scholar]
- 2.Perissat J. Laparoscopic cholecystectomy: the European experience. Am J Surg. 1993;165:444–449. doi: 10.1016/s0002-9610(05)80938-9. [DOI] [PubMed] [Google Scholar]
- 3.Siewert JR, Feussner H. Minimalinvasive chirurgie-Zwishenbilanz 1994. Langenbecks Arch Chir. 1994:129–139. [Google Scholar]
- 4.Mayo CW, Rice RG. Situs inversus totalis; a statistical review of data on 76 cases with special reference to disease of the biliary tract. Arch Surg. 1949;58:724–730. [PubMed] [Google Scholar]
- 5.Sato S, Watanabe M, Nagasawa S, Niigaki M, Sakai S, Akagi S. Laparoscopic observations of congenital anomalies of the liver. Gastrointest Endosc. 1998;47:136–140. doi: 10.1016/s0016-5107(98)70345-1. [DOI] [PubMed] [Google Scholar]
- 6.Campos L, Sipes E. Laparoscopic cholecystectomy in a 39-year-old female with situs inversus. J Laparoendosc Surg. 1991;1:123–125; discussion 126. doi: 10.1089/lps.1991.1.123. [DOI] [PubMed] [Google Scholar]
- 7.Lipschutz JH, Canal DF, Hawes RH, Ruffolo TA, Besold MA, Lehman GA. Laparoscopic cholecystectomy and ERCP with sphincterotomy in an elderly patient with situs inversus. Am J Gastroenterol. 1992;87:218–220. [PubMed] [Google Scholar]
- 8.Drover JW, Nguyen KT, Pace RF. Laparoscopic cholecystectomy in a patient with situs inversus viscerum: a case report. Can J Surg. 1992;35:65–66. [PubMed] [Google Scholar]
- 9.Takei HT, Maxwell JG, Clancy TV, Tinsley EA. Laparoscopic cholecystectomy in situs inversus totalis. J Laparoendosc Surg. 1992;2:171–176. doi: 10.1089/lps.1992.2.171. [DOI] [PubMed] [Google Scholar]
- 10.Goh P, Tekant Y, Shang NS, Ngoi SS. Laparoscopic cholecystectomy in a patient with empyema of the gallbladder and situs inversus. Endoscopy. 1992;24:799–800. doi: 10.1055/s-2007-1010589. [DOI] [PubMed] [Google Scholar]
- 11.Huang SM, Chau GY, Lui WY. Laparoscopic cholecystectomy for cholelithiasis in a patient with situs inversus totalis. Endoscopy. 1992;24:802–803. doi: 10.1055/s-2007-1010591. [DOI] [PubMed] [Google Scholar]
- 12.McDermott JP, Caushaj PF. ERCP and laparoscopic cholecystectomy for cholangitis in a 66-year-old male with situs inversus. Surg Endosc. 1994;8:1227–1229. doi: 10.1007/BF00591057. [DOI] [PubMed] [Google Scholar]
- 13.Crosher RF, Harnarayan P, Bremner DN. Laparoscopic cholecystectomy in situs inversus totalis. J R Coll Surg Edinb. 1996;41:183–184. [PubMed] [Google Scholar]
- 14.Demetriades H, Botsios D, Dervenis C, Evagelou J, Agelopoulos S, Dadoukis J. Laparoscopic cholecystectomy in two patients with symptomatic cholelithiasis and situs inversus totalis. Dig Surg. 1999;16:519–521. doi: 10.1159/000018780. [DOI] [PubMed] [Google Scholar]
- 15.Djohan RS, Rodriguez HE, Wiesman IM, Unti JA, Podbielski FJ. Laparoscopic cholecystectomy and appendectomy in situs inversus totalis. JSLS. 2000;4:251–254. [PMC free article] [PubMed] [Google Scholar]
- 16.Hugh TB, Kelly MD, Li B. Laparoscopic anatomy of the cystic artery. Am J Surg. 1992;163:593–595. doi: 10.1016/0002-9610(92)90564-8. [DOI] [PubMed] [Google Scholar]