

Abstract
Acute locked knee is commonly caused by tears of the menisci in the knee, osteochondral injuries and also by the stump of a ruptured anterior cruciate ligament. We present two cases of acute locked knee atypically caused by gouty tophaceous lesions in the knee.
Keywords: Acute locked knee, Gout, Arthropathy, Knee
Introduction
Locked knee is a condition in which the affected person is unable to fully extend the knee. It is usually caused by mechanical impediment to knee extension such as bucket handle tears of the meniscus, loose osteochondral fragments or the stump of a ruptured anterior cruciate ligament. We present two cases in which atypical presentation of gouty arthropathy had caused acute locked knee in patients not previously diagnosed with this condition.
Case 1
A 35-year-old Malay man was seen in Serdang Hospital Specialist Clinic complaining of sudden inability to fully extend his left knee. There was no previous history of trauma to the knee. Further questioning revealed that he did experience non-specific left knee pain on and off which usually resolved by itself. There was no pain in other joints. The patient is not known to have any medical problems.
On examination, he walked with an antalgic gait with a swollen left knee that was locked in 10 degrees flexion. However, knee flexion was full. Clinical tests for torn ligaments and menisci were negative. His serum uric acid was within normal range. He was posted for diagnostic arthroscopy. Intra-operatively, there was generalized tophi deposit over the articular cartilage especially involving the patella (Fig. 1). Interestingly, there was also a tophaceous lesion noted arising from the anterior horn of the medial meniscus which prevented full extension (Fig. 2). The lesion was carefully excised and histopathological examination showed urate crystals present in the meniscal lesion. Post-operatively, he developed swelling in the left knee which required knee aspiration. He responded well to analgesics and a urate-lowering agent. He was able to regain a full range of motion in the left knee at four weeks post-operatively.
Fig. 1.
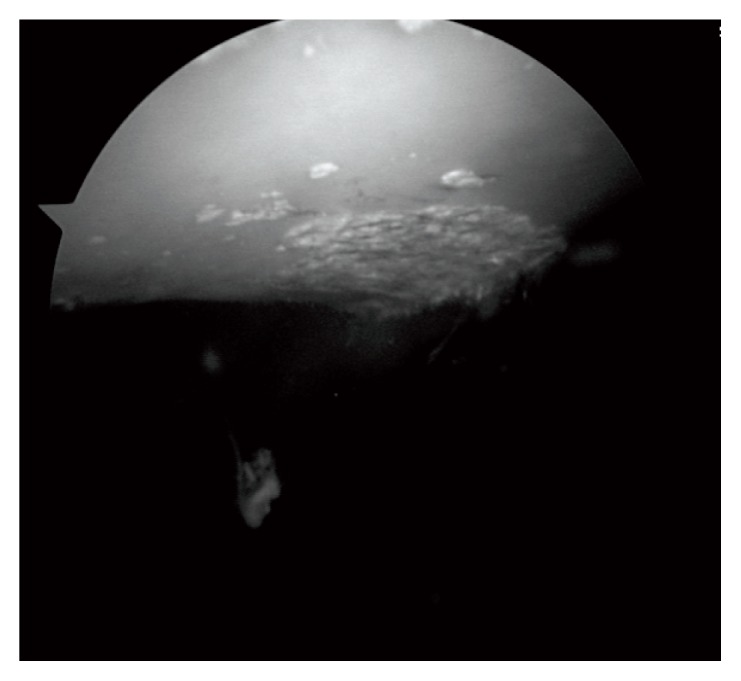
Arthroscopy of the left knee. Case 1 - Tophi deposit over the patellar surface.
Fig. 2.
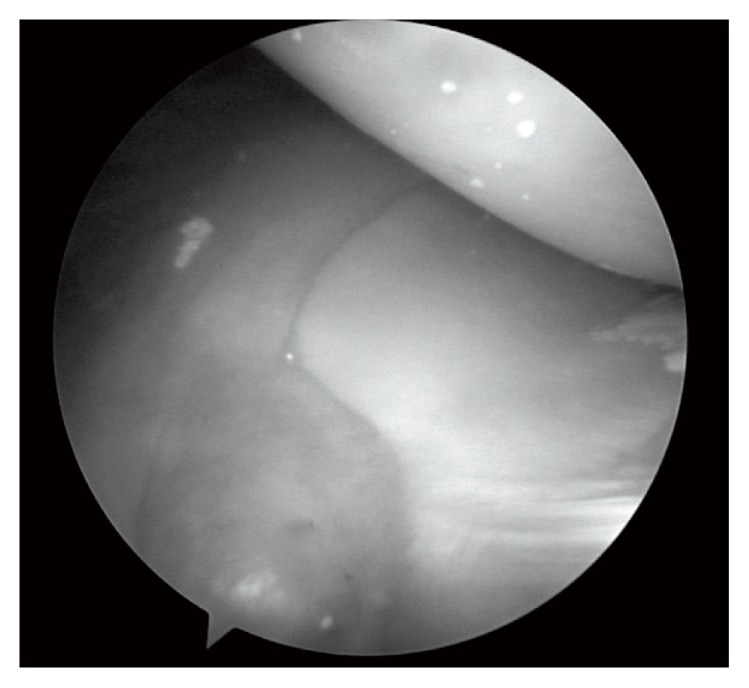
Left knee. Case 1 - Tophaceous lesion noted arising from the anterior horn of the medial meniscus preventing full extension of the knee.
Case 2
A 24-year-old Malay man presented to the clinic with swelling and inability to straighten his left knee. He related his condition to an episode of fall three weeks prior to the visit. Upon examination, his left knee was swollen and was locked in 30 degrees of flexion. There was tenderness along both joint lines. Lachmann test for anterior cruciate ligament deficiency was positive. A magnetic resonance imaging (MRI) was performed and revealed a complete anterior cruciate ligament tear with intra-articular loose bodies.
The patient underwent a diagnostic arthroscopy which revealed significant findings of synovitis with formation of clumps of tophi in the synovial tissue near the anterior horn of the medial meniscus. There was also generalized tophi deposit on the articular cartilage especially over the patella. These tophaceous synovial clumps prevented full extension of the knee during arthroscopic examination. There was complete tear of the anterior cruciate ligament (ACL) with deposition of chalky material over the ACL stump and the posterior cruciate ligament. Debridement of the tophi was done. The diagnosis was later confirmed histopathologically by evidence of urate crystals in the synovial biopsy. He was subjected to physiotherapy, a urate-lowering agent and non-steroidal anti-inflammatory (NSAID) drugs post operatively. He regained full range of movement three weeks after the procedure and treatment.
Discussion and conclusion
Locked knee is considered a ‘relative’ emergency condition of the knee. Common causes of locked knee are mechanical blocks from various aetiology (1). Once the knee is held in a chronically locked position, structures around the affected knee will be contracted and this will result in flexion deformity. This deformity will be permanent unless the locking is corrected. Furthermore, chronic locked knee will develop a focal stress point over the tibia-femoral articulation which in turn will promote cartilage degeneration.
Gouty arthritis is a common metabolic disorder which causes hyperuricaemic state due abnormal purine metabolism. This condition will progress into formation of mono-sodium urate crystals in the body. The clinical spectrum of presentation varies from asymptomatic to chronic pain. There are four distinct phases which include asymptomatic hyperuricaemia, acute gouty arthritis, intercritical gout and chronic tophaceous gout (2). Deposition of the tophi can be found in the toes, fingers, scrotum and external ears. Crystals can also be deposited in the articular cartilage and tendons.
Gouty arthritis is a great mimicker. It can mimic conditions such as infection and neoplasm. The most common site of presentation of gout is in the first metatarsophalageal joint. Unilateral presentation of knee pain is another common presentation of gout. The presence of intra-articular tophi can cause mechanical block and pain is usually caused by intra-articular loose bodies (3, 4). Although the condition is rare as illustrated in this case report, locked knee can be the only presentation for this disease entity.
Radiographic presentation the gouty arthropathy is non-specific because these crystals are radiolucent. Common plain radiographic findings are soft tissue swelling, calcification and bony erosion. These findings are usually observed during late stages of the disease. Other imaging modalities such as Magnetic Resonance Imaging (MRI) and ultrasound are especially useful in diagnosing intra-articular involvement. Definitive diagnosis of gouty arthritis is made based on joint-aspirate analysis. Presence of weakly-positive birefringent urate crystals under polarized light is confirmatory.
Most authors suggest debridement as the mainstay of treatment. Although arthroscopic debridement may be essential in the treatment of locked knee due to tophi deposition, the paramount treatment for gouty arthropathy is still medical treatment of hyperuricaemia. Chaterjee et al. reported a case of locked knee in a patient declining arthroscopic debridement that was successfully treated by urate-lowering agent and anti-inflammatory drugs (5). Thus, medical treatment can be deployed in cases where arthroscopic surgery is not an option or considered too risky for the affected patient.
References
- 1.Bansal P, Deehan DJ, Gregory RJH. Diagnosing the acutely locked knee. Injury. 2002;33:495–498. doi: 10.1016/s0020-1383(02)00081-5. [DOI] [PubMed] [Google Scholar]
- 2.Amber H, Singh VA, Azura M. Gouty tophi mimicking synovial sarcoma of the knee joint. Turk J Rheumatol. 2012;27(3):208–211. [Google Scholar]
- 3.Kijkunasathian C, Woratanarat P, Saengpetch N. Gouty tophi caused limited knee range of motion: A case report. J Med Assoc Thai. 2009;92(Suppl 6):S264–S267. [PubMed] [Google Scholar]
- 4.Espejo-Baena A, Coretti SM, Fernandez JM, Garcia-Herrera JM, Del Pino JR. Knee locking due to a single gouty tophus. J Rheumatol. 2006;33:193–195. [PubMed] [Google Scholar]
- 5.Chatterjee S, Ilaslan H. Painful knee locking caused by gouty tophi successfully treated with allopurinol. Nat Clin Pract Rheumatol. 2008;4:675–679. doi: 10.1038/ncprheum0945. [DOI] [PubMed] [Google Scholar]