

Abstract
Objective
The purpose of this case series is to describe the use of diagnostic ultrasound (US) in the detection of occult rib and costal cartilage fractures presenting as chest wall pain to a chiropractic clinic.
Clinical features
Three patients presented with chest wall pain and tenderness. Two of the patients presented with acute chest wall injury and 1 carried a previous diagnosis of rib fracture after trivial trauma 2 months earlier.
Intervention and outcomes
Diagnostic US was selected as a non-ionizing imaging tool for these patients after negative digital radiography studies. All fractures were considered isolated as there was no associated injury, such as pneumothorax. Both of the acute cases were followed up to complete healing (evidence of osseous union) using US. All patients eventually achieved pain-free status.
Conclusion
In these cases, US was more sensitive than radiography for diagnosing these cases of acute rib and costal cartilage fractures. Early recognition of rib injury could avoid potential complications from local manipulative therapy.
Key indexing terms: Chiropractic; Diagnostic imaging; Fractures, bone; Fractures, cartilage; Rib fractures; Ultrasonography
Introduction
Fracture of the rib or costal cartilage is a diagnosis that should be excluded even in the setting of trivial trauma to the chest wall. Up to 50% of rib fractures may be missed at radiography, so the true incidence of rib fractures cannot be determined using radiography as the primary diagnostic test.1 Moreover, Palvalen et al reported the incidence and complications of rib fractures due to minimal trauma have been increasing in the last 30 years, especially in the elderly. They suggest this may be due to an increased tendency for falls amongst frail and elderly patients who are surviving to a later age due possibly to advancements in medicine.2 Previous studies have shown diagnostic ultrasound (US) is more sensitive than radiography for the detection of acute rib fractures.3
Although displaced acute rib fractures, healing fractures with callus formation, or those associated with other injuries may be readily identified with radiography, costal cartilage is not visible unless it undergoes physiologic calcification.4 Isolated rib fractures are defined as having no associated injury, regardless of the number of ribs fractured.5
Accurate diagnosis of such rib injuries may positively influence patient outcomes and avoid potential complications. Therefore, the purpose of this case series is to describe the use of US in the detection of radiographically occult rib and costal cartilage fractures. We present a series of 3 fractures, 2 in ribs and 1 in costal cartilage, which were detected by US, but undetectable by digital radiography.
Case Reports
The patients discussed in the following cases each gave written consent to educational usage of their images and clinical data.
Case 1
A 35-year-old man fell and sustained direct trauma to his upper left, anterior chest. The patient presented 1 day following the injury. His symptoms included pain with breathing (especially forced expiration), coughing, sneezing, yawning, and left arm movement. Vital signs were normal. Physical exam revealed pain and tenderness covering a broad area over the left pectoralis major muscle, worse in the mid-clavicular line. Any activation of the pectoralis major muscle increased his pain. There was edema and erythema in the mid-clavicular line. US of the left anterior chest wall was performed for evaluation of the muscle injury and to rule out rib fracture. He was examined with a GE Logiq E9 (GE Healthcare, Milwaukee, WI) ultrasound system using a high frequency linear transducer (ML6-15) operating at 12 MHz utilizing a standardized rib protocol. It consisted of imaging each symptomatic rib and the adjacent asymptomatic ribs in the longitudinal and transverse planes along its entire extent. US examination in the longitudinal plane revealed cortical discontinuity of the left third and the fourth anterior ribs approximately 1.5 cm lateral to the costochondral junction. Overlying hematoma was evident at both fracture sites (Fig 1). Dynamic imaging obtained during the phases of respiration provided increased conspicuity of the cortical offset at the fracture site. Radiography of the chest and left ribs were ordered for confirmation of the fractures and exclusion of a pneumothorax. The images were interpreted as negative for fracture and there were no other complicating factors, such as pneumothorax. Over the next 3 weeks, the patient experienced disturbed sleep and continuation of his presenting symptoms with gradual improvement.
Fig 1.
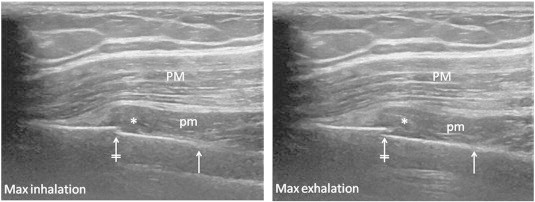
Diagnostic US in the longitudinal plane of a rib during maximal inhalation demonstrating cortical offset (crossed arrow) consistent with a fracture and surrounding hematoma (asterisk) displacing the overlying pectoralis minor muscle (pm) and a portion of the pectoralis major muscle (PM). The costochondral junction (solid arrow) is located medial to the fracture. US of the same rib demonstrates increased cortical offset during maximal exhalation.
Follow-up US examinations at 1-week intervals2 and then 2-week intervals2 demonstrated interval hematoma organization, callus formation, and eventual US evidence of osseous union. This information was utilized to inform the patient about his clinical status and to indicate when fracture healing was achieved. The US appearance of his fracture was used to guide his level of activity and his return to regular activity, both at work and during athletics.
Case 2
A 28-year-old male presented with a history of a fractured lower left rib that was sustained while wrestling 2 months prior. It was diagnosed clinically in the emergency department at that time. The patient was told that no treatment could be provided, and he declined diagnostic imaging. At physical exam in our clinic, there was exquisite tenderness and pain in his lower left anterior chest wall that radiated to his mid-back. He had experienced little improvement with no treatment since the incident. The pain was provoked by specific movements and prevented him from assuming certain recumbent positions. Radiography of the chest and left ribs were ordered and interpreted as negative without complications. US was recommended for further investigation of the pain site and revealed a fracture of the left costal cartilage at T8 with surrounding hematoma (Fig 2). The US appearance of normal costal cartilage is shown for comparison. Four-week follow-up was requested but was unavailable at the time of this publication.
Fig 2.
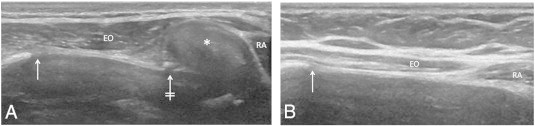
(A) US in the longitudinal plane of the costal cartilage. Disruption of the cartilage (crossed arrow) is demonstrated with overlying hematoma (asterisk). (B) US of a normal costal cartilage in the longitudinal plane. The osseous portion of the rib ends at the costochondral junction (solid arrow). The rectus abdominus muscle (RA) is seen medially and the external oblique muscle (EO) is seen laterally.
Case 3
A 24-year-old male presented to our clinic with left anterior chest pain following direct trauma 1 week prior. Physical exam revealed bruising over the left pectoralis major muscle, edema and localized pain with light palpation. Radiography of the chest and left ribs were ordered and interpreted as negative with no complications. US was ordered 3 weeks later due to ongoing pain and demonstrated cortical discontinuity of the left second anterior rib approximately 1.7 cm lateral to the costochondral junction with callus formation, but no osseous bridging (Fig 3). Three-week follow-up US exam revealed bridging of the callus indicating fracture healing.
Fig 3.
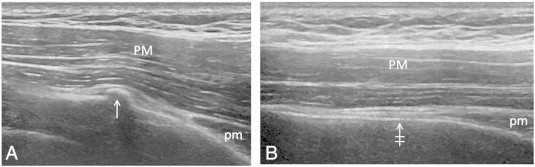
(A) US in the longitudinal plane of a rib demonstrates cortical disruption with early callous formation (arrow). The pectoralis minor (pm) and major (PM) muscles can be seen overlying the rib. (B) US in the longitudinal plane of a normal rib demonstrates the normal continuous cortex of the bone (crossed arrow).
Discussion
A review of the literature revealed descriptions of the utility of US in the diagnosis of rib and costal cartilage fractures,6–8 but these studies were all performed in an allopathic setting. To our knowledge, this is the first published case series of US diagnosis of these fractures in the setting of a chiropractic clinic. These patients were presenting for palliative care, which would likely have consisted of manipulation of the thoracic spine had no fractures been detected.
Studies have shown US to be superior to radiography in the detection of acute rib3,6,7 and costal cartilage8 fractures. At US, rib injuries may display a disruption of the normally continuous echogenic cortex of the rib, disruption of the costochondral junction, or fracture of the costal cartilage.3 In a study by Griffith et al US detected 10 times as many fractures in 6 times as many patients as radiography and 11% of those fractures were located in the costal cartilage or at the costochondral junction.3 Turk et al diagnosed rib fractures by US in 18/20 patients who had negative radiography, but continuing pain. Their study showed that US had a sensitivity of 78% compared to 12% for radiography in the detection of rib fractures, including costal cartilage fractures.6 Additionally, a fracture of the costal cartilage is not radiographically visible unless it involves a densely calcified cartilage.8 For these reasons, fractures of the costal cartilage probably occur with greater frequency than is currently recognized and therefore often go undiagnosed.8
As demonstrated in Fig 2, the costal cartilage is readily visualized utilizing US, as its echogenicity approaches that of cortical bone. Other advantages of US include the absence of ionizing radiation inherent in radiography, computed tomography (CT), and scintigraphy, the ability to examine each rib parallel to its long axis (not possible with CT), and lack of interference from respiratory motion, which is a limitation of MRI.3 The first case demonstrated an example of the dynamic imaging capability of US in which respiratory phases enhance fracture edge detection. Another consideration for the use of US, instead of radiography, is that children are more sensitive to harms of ionizing radiation, so the pediatric population would be more safely imaged with US.9,10
Many rib injuries have additional complications of trauma. In Bandsihar's study, 31.1% of rib fracture patients had pulmonary contusions and 19.6% had pneumothorax.11 Although it was not utilized in the cases presented, US has been shown to be effective in the detection of pneumothorax and pleural effusions.12 An immediate diagnosis would allow proper treatment and could avoid such pulmonary complications.7
Prompt recognition could also avoid potential complications from local manipulative therapy. Informed by a radiographic examination that was interpreted as negative, it is possible a clinician could utilize manipulation in the treatment of a patient with an occult rib or costal cartilage fracture. In our institution, it has become common practice to refer negative radiographic studies in chest wall trauma cases for US examination. Further investigation by US often yields a fracture diagnosis and, in some cases, precludes the need for more expensive advanced imaging studies. Knowledge of a radiographically occult fracture will inform on the risks of manipulation of the thoracic spine. Compression of the thoracic cage during manipulation could potentially exacerbate an occult fracture and cause pulmonary complications. Treatment instead could be directed toward pain relief and prevention of pulmonary complications and include limitation of physical activity, analgesics such as medications, or complementary and alternative medicine.7,13 Even in the absence of pulmonary complications, fractures of the rib or costal cartilage cause pain, which may result in time lost from work and reduced quality of life.7 Immediate treatment may allow for quicker recovery and higher patient satisfaction. One study showed that 65% of patients with rib fractures were able to return to work without difficulty with overall length of disability of 27 ± 26 days.11 Unrecognized or untreated rib fractures cause a substantial increase in morbidity and mortality, especially in the elderly or if complications are present.11 Barnea et al showed morbidity of 38% and mortality of 8% in elderly patients even with isolated rib fractures and no associated injuries.5
Patients 1 and 3 were re-examined periodically in their course of care with US until healing was achieved. The patients used this status to gauge their return to full physical activity. Following a fractured rib with serial US is safe as it does not employ ionizing radiation, especially in more radiation sensitive populations, such as children or pregnancy. Callus formation is easily visualized on US and predates its appearance on radiography. The same is true for fracture union.14
It was previously stated that US has been shown to be superior in the detection of rib and costal cartilage fractures. Our case series showed identical results. Our case series, however, was unique in that it detected occult fractures in patients who were presenting to a chiropractic clinic for evaluation of chest wall pain. Manipulation may have been performed if fractures were excluded at radiography, potentially complicating the fractures and raising medico-legal risk factors.
Currently, American College of Radiology (ACR) Appropriateness Criteria does not recommend US examination in the workup of rib fractures. Part of the reasoning is that detection of a rib fracture by US would not significantly impact patient care.15 While this may be true in an allopathic setting, the potential application of manipulation to any part of the thoracic cage could negatively impact a fractured rib, so it seems that it may play a greater role in a manual therapy setting.
Future research should be directed at studying the routine use of US in the imaging algorithm after negative radiographic studies to assess cost-savings compared to more expensive advanced imaging modalities. In addition, the assessment of the presumptive risk facing a clinician who employs manual therapy in the setting of a radiographically occult chest wall fracture warrants investigation. In the setting of a chiropractic clinic with readily-available US, we assert that it should be included in the workup of even minor thoracic wall trauma.
Limitations
There are limitations to this case report. Generalization of the diagnostic findings represented in this case series may not necessarily be applied to other patients or the population. Also, although it seems highly reasonable, it is only speculation that local manipulation could have exacerbated the condition of the patients.
Conclusion
In this case series, US was more sensitive for detecting acute, isolated fractures of the rib and costal cartilage than conventional radiography. Ultrasound should be considered when focal pain is present following even trivial chest trauma and radiography is interpreted as negative for fracture.
Funding Sources and Conflicts of Interest
No funding sources were reported for this study. One of the patients reported in this manuscript is an author, however this has no bearing on the results of this case series.
References
- 1.Bulger E.M., Arneson M.A., Mock C.N., Jurkovich G.J. Rib fractures in the elderly. J Trauma. 2000;48(6):1040–1046. doi: 10.1097/00005373-200006000-00007. [discussion 6–7] [DOI] [PubMed] [Google Scholar]
- 2.Palvanen M., Kannus P., Niemi S., Parkkari J., Vuori I. Epidemiology of minimal trauma rib fractures in the elderly. Calcif Tissue Int. 1998;62(3):274–277. doi: 10.1007/s002239900429. [DOI] [PubMed] [Google Scholar]
- 3.Griffith J.F., Rainer T.H., Ching A.S., Law K.L., Cocks R.A., Metreweli C. Sonography compared with radiography in revealing acute rib fracture. AJR Am J Roentgenol. 1999;173(6):1603–1609. doi: 10.2214/ajr.173.6.10584808. [DOI] [PubMed] [Google Scholar]
- 4.Ontell F.K., Moore E.H., Shepard J.A., Shelton D.K. The costal cartilages in health and disease. Radiographics. 1997;17(3):571–577. doi: 10.1148/radiographics.17.3.9153697. [DOI] [PubMed] [Google Scholar]
- 5.Barnea Y., Kashtan H., Skornick Y., Werbin N. Isolated rib fractures in elderly patients: mortality and morbidity. Can J Surg J. 2002;45(1):43–46. [PMC free article] [PubMed] [Google Scholar]
- 6.Turk F., Kurt A.B., Saglam S. Evaluation by ultrasound of traumatic rib fractures missed by radiography. Emerg Radiol. 2010;17(6):473–477. doi: 10.1007/s10140-010-0892-9. [DOI] [PubMed] [Google Scholar]
- 7.Kara M., Dikmen E., Erdal H.H., Simsir I., Kara S.A. Disclosure of unnoticed rib fractures with the use of ultrasonography in minor blunt chest trauma. Eur J Cardiothorac Surg. 2003;24(4):608–613. doi: 10.1016/s1010-7940(03)00383-x. [DOI] [PubMed] [Google Scholar]
- 8.Malghem J., Vande Berg B., Lecouvet F., Maldague B. Costal cartilage fractures as revealed on CT and sonography. AJR Am J Roentgenol. 2001;176(2):429–432. doi: 10.2214/ajr.176.2.1760429. [DOI] [PubMed] [Google Scholar]
- 9.Hubner U., Schlicht W., Outzen S., Barthel M., Halsband H. Ultrasound in the diagnosis of fractures in children. J Bone Joint Surg (Br) 2000;82(8):1170–1173. doi: 10.1302/0301-620x.82b8.10087. [DOI] [PubMed] [Google Scholar]
- 10.Williamson D., Watura R., Cobby M. Ultrasound imaging of forearm fractures in children: a viable alternative? J Accid Emerg Med. 2000;17(1):22–24. doi: 10.1136/emj.17.1.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bansidhar B.J., Lagares-Garcia J.A., Miller S.L. Clinical rib fractures: are follow-up chest X-rays a waste of resources? Am Surg. 2002;68(5):449–453. [PubMed] [Google Scholar]
- 12.Koh D.M., Burke S., Davies N., Padley S.P. Transthoracic US of the chest: clinical uses and applications. Radiographics. 2002;22(1):e1. doi: 10.1148/radiographics.22.1.g02jae1e1. [DOI] [PubMed] [Google Scholar]
- 13.Okada K., Kawakita K. Analgesic action of acupuncture and moxibustion: a review of unique approaches in Japan. Evid Based Complement Alternat Med. 2009;6(1):11–17. doi: 10.1093/ecam/nem090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Craig J.G., Jacobson J.A., Moed B.R. Ultrasound of fracture and bone healing. Radiol Clin North Am. 1999;37(4):737–751. doi: 10.1016/s0033-8389(05)70126-3. [ix] [DOI] [PubMed] [Google Scholar]
- 15.American College of Radiology ACR Appropriateness Criteria® 1995. http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/RibFractures.pdf [updated 2011; cited 2014 January 7]. Available from.