

Abstract
Background: Acquired immune deficiency syndrome (AIDS) was firstly reported from California and soon became a pandemic in the world. This disease poses serious threats to humans’ health. In this study, we intended to examine the characteristics of HIV-positive patients who referred to the Behavioral Diseases Consultation Center (BDCC) in Shiraz, Iran.
Methods: This was a cross-sectional descriptive study. HIV-positive patients, referring toBDCC of Shiraz University of Medical Scienceswere the population under the study. The data, collected through a checklist, were encoded and entered in to the SPSS 19. Then descriptive statistics such as mean, median, standard deviation and range were used to describe the variables. Also, the relationships between the variables were tested using X2 test.
Results: The mean and median age of the HIV-positive patients were 39 + 8.7 and 38years, respectively.Nearly327 (65.4%) of the studied population were male and 173 (34.6%) were female. With respect to marital status, 225 (45%) participants were married, 133 (27%) were single, 91 (18.2%) were divorced and 49 (9.8%) were widowed. Also, 265(53%) of the participants were infected through injection drug use, 198 (39.6%) through sexual route, 7 (1.4%) through blood and blood products, 6 (1.2%) through tattoos and 21 (4.2%) by other routes. Most of the participants had a HIV-positive history in their family, and 145 (29%) mentioned that their wives were HIV-positive. Moreover, 320 (62.7%) of the participants had a positive history of drug use, 176 (35.2%) did not have a history of drug abuse, and the status of 10 (2%) participants was not recognized.
Conclusion: Although the results of this study highlighted that injection addiction remains the major transmission route inIran, the role of sexual transmission should be acknowledged in the future.
Keywords: HIV, AIDS, Descriptive study, Epidemiologic Characteristics, Shiraz, Iran
Introduction
AIDS was firstly reported from California and soon became a pandemic in the world. (1). Undoubtedly, AIDS has been the greatest scourge of human society since World War II (2). AIDS, which is one of the dangerous communicable diseases caused by Human Immunodeficiency Virus (HIV), can severely endanger the protective powers of the body against infections and rare cancers(3, 4). The spectrum of this disease consist of light viremia to severe immunodeficiency diseases and life-threatening infections(5, 6).Center for Disease Control and Prevention in the United States defined AIDS as a deep disorder in the immune system, as the result of depletion in helper T cells, in which the host is prone to affliction with severe opportunistic infections or malignant disease(7).
Because the initial incidence of the disease took place among homosexuals and intravenous drug abusers in the United States, it was expected that AIDS be limited to a particular social group, or a particular geographic region of the world. Nonetheless, as to a new occurrence of this infection in Africa via heterosexual diseases, AIDS has been recognized as a global problem and no race, nation, gender or age is safe from the infection (8, 9).
In Iran, like other Asian countries, the number of people living with HIV and being diagnosed with AIDS has been increased(10). The prevalence of AIDS in Iran consists of three waves. In the first wave in 1987, AIDS emerged through infected blood products. The second wave of this disease occurred by shared needles among drug users in 1996-1997. Currently, in the third wave of AIDS, sexual promiscuity and lack of commitment to ethical behaviors may seriously threaten the community’s health or safety(11).
Among the total registered AIDS patientssince1986 in Iran, the followings have been accounted for transmission of HIV, respectively: injection trough shared tools in drug abusers (69.7%), sexual relationships (8.4%), receiving blood and blood products (1.2 %) and mother to child transmission (.6%). Also, 20.1% of these cases are ranked as unrecognized transmission modes. In 2008, it was reported that injection drug addiction (76.8%), sexual relationships (13.6%) and mother to child transmission (.8%) accounted for transmission routes of AIDS in Iran with the exception of8.8% of the diagnosed patients who showed unrecognized transmission route; in addition, no transmission was reported from blood product (12). Statistics for these transmission routes in 2010have changed to the followings: injection drug addiction (66.1%), sexual relationships (20.8%), mother to child transmission (2.5%), unrecognized (10.6%), with no new cases of blood product transfusion. According to the latest reports, the total number of HIV patients who were detected in Iran until the end of December 2011was equal to 23,497; of whom, 91.3% were male and 8.7% were female. In addition, 3168 patients entered the AIDS stage and 4419 died. Nearly46% of the HIV-positive patients were in 25-34 age groups. However, based on estimations in 2003, there were 30000-40000 HIV-positive patients in Iran; this number reached 80000 in 2007 and will continue to exceed126000 in 2015 (13).There are no vaccines or medicines for the absolute treatment of AIDS. This disease has evolved rapidly in recent years and the number of patients has dramatically increased due to lack of awareness, lack of proper care, and lack of centralized services (14).
Public fear of HIV disease has affected many aspects of social life of these patients because 88% of the patients are aged 20 to 49, and the detection of HIV can cause family breakdown, decline in economic activities and may also lead to family poverty (15, 16). While AIDS remains a major health problem, it has become a complex social and economic emergency case to be attended. Because AIDS often afflicts seniors as the active group of the community and create obstacles for the private sector development and the public, it can impede a nation’s development and thus push the developing countries into deterioration(17). Due to the potential risks of HIV infection for human communities, fighting against this disease was reflected in the millennium development program (18). Therefore, in this study, we aimed to epidemiologically depict the characteristics of HIV-positive patients who referred to BDCC of Shiraz University of Medical Sciences. Surely, highlighting the image of AIDS's features in the society can be of great help in making policies against this dread fulepidemic.
Methods
This was a cross-sectional descriptive study. HIV-positive patients who referred to BDCC of Shiraz University of Medical Sciences were the population of this study. To collect data, a checklist specifically designed for this purpose, was used. This checklist consisted of two sections: the first section included demographic variables; andthe second part was based on specialized variables such as history of addiction and drug abuse, history of HIV in the family, disease transmission, ART therapy states, stage of the disease, CD4 counting, duration of drug consumption and drug addiction.
Due to the confidentiality of the patients’ information anddifficulty accessing thisinformation, nearly 500 patients were included in the study. The required data were obtained from the patients’ medical folders. Also, we interviewed HIV-positive patients if their folders were incomplete.
The collected data for this research were encoded and entered into the SPSS 19 using descriptive statistics such as mean, median, standard deviation and range. Moreover, the relationship between the qualitative variables was found using X2 test.
Results
The mean age of the studied patients was 39±8.7, ranging from 8 to 70 years. As demonst rated by Graph 1,327 (65.4%) participants were male and 173 (34.6%) were female. As presented in Graph 2 ,225 (45%) of the participants were married, 133 (27%) were single, 91 (18.2%) were divorced and 49 (9.8%) were widowed. Most of the HIV-positive patients were in the 26-45 age range.
Graph (1) .
Gender of the Studied Cases
Graph (2) .
Marital Status of the Studied Cases
With respect to clinical aspects, 272 patients (54.4%) had been under ART treatment and 228 (45.6%) had not. Also, 385 patients (77%) were in the nonclinical phase and 115 (23%) experienced the clinical phase. With regards toCD4 counting, 194 patients (38.8%) hadCD4<200, 175 (35%) had CD4 between 200 to 350, 57 patients (11.4%) had CD4 between 350 to 500 and 74 of them (14.8%) had more than 500 CD4.
Considering the transmission mode, 265 patients (53%) were afflicted with HIV through injection drug addiction, 198 (39.6%) and 7 patients (1.4%) through blood and blood products respectively, 6 patients (1.2%) through tattoo, and 21 (4.2%) through other modes; the frequencies are demonstrated in Table 1. Also, 145 (29%) participants had HIV-positive cases in their family; and the majority of them declared that their wives were HIV-positive.
Table 1 . Transmission Mode .
| Transmission mode | Frequency | Percent |
| Injection | 265 | 53.3 |
| Sexual | 198 | 39.6 |
| Blood | 7 | 1.4 |
| Tattoo | 6 | 1.2 |
| Other Routes | 21 | 4.2 |
| Unrecognized Subjects | 3 | 0.6 |
| Total Subjects | 500 | 100 |
With respect to addiction history, it has been demonstrated that 320 participants (62.7%) had the history of narcotic use and 176 did not. Also, the background of 10 participants (2%) was unrecognized. Most addictive substances used were opium (225 patients), heroin (195 patients), and hashish and crystal were the next in order. Most addictive-history positive patients (289) mentioned that they had a history of more than 10 years of substance use. Intravenous drug addiction by 220 patients (44%) was the prevailing form of substance use in this study.
In this research, based on X2 test, assign if cant relationship was found between gender and transmission mode (p<0.001). The major transmission mode was injection drug addiction inmales and it was sexual transmission in females ( Graph 3). Also a significant association was obtained between substances used, the type and transmission mode (p<0.001). Intravenous drug addiction in opium and heroin users were 31.3% and 27.9%, respectively and it was 23.2%for other substances. Although a significant association was observed between marital status and transmission mode (p<0.001), the main transmission in the married participants was sexual relations (20.5%) and it was injection drug addiction (22.1%) in the single participants.
Graph (3) .
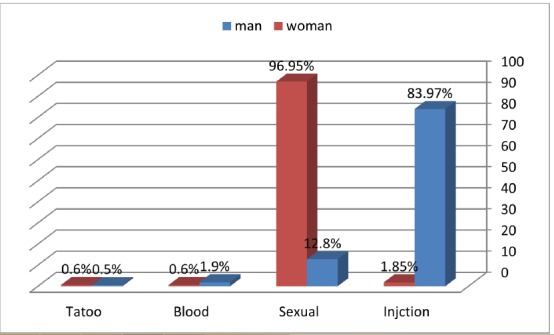
Gender and Transmission Routes
Discussion
Concerns about AIDS have prompted many researchers to study this disease. The main propose of this study was to epidemiologically demonstrate the characteristics of HIV-positive patients. Although most of the HIV-positive patients were male, which is in line with national and global statistics (19),astonishingly, the number of females with HIV was also high (173=34.6%). In this research, it was demonstrated that HIV has afflicted individuals in 26-45 age range. This finding is in line with the national and international average (19). The youths are more likely to develop risky behaviors; hence, preventing these behaviors may reduce the prevalence of AIDS remarkably in this group.
In our findings, it has been demonstrated that the major transmission mode of AIDS is in the same line with the national pattern(19) and injection drug use (53% of the patients) was in contrast with global statistics(9).Some studies (20-28) also found that the mean transmission mode in Iran is injection drug use. In this study, it was revealed that this transmission rate was lower than the national average (around 66%) in Iran (29)). Also, single participants mentioned that they mostly got HIV through injecting drug use. Because Iran has a large number of injecting drug users (21), great consideration should be given to this transmission route in Iran.
Of the participants, 36.9% reported sexual relationships as the transmission route. Most of the infected patients through this route had a HIV- positive wife who had been afflicted with the disease through injection drug use. Some studies(20, 25, 27, 28, 30)have also indicated sexual transmission as the second dominant route of HIV infection. However, statistics for this route is higher than the national statistics(13). In this study, we found that injecting drug use was the most common transmission category in males and sexual transmission was the most common in females. However, it should be noted that most female participants in this study were married. This finding is consistent with the national transmission pattern (19). Moreover,1.2% of our participants got the disease through blood and blood products. Compared with the national rate, this finding is natural, but Katibeh and Hariat (26)found that 11.5% of their participants got infected through transfusion route.
Based on the findings of this study, it seems that the transmission pattern of HIV/AIDS is changing in Iran. Although previously injection addiction accounted for the major transmission route, currently sexual route has possibly been replaced by it. It seems that the emerging pattern of HIV in Iran mostly targets younger people. Therefore, adolescents and young adults should be acquainted with the related preventive measures against HIV. Although AIDS has no vaccine or specific treatment(9), educating people particularly younger individuals about use of safe needles for injecting drugs and changing their addiction habits can help reduce the prevalence and incidence of this disease in the coming years. Controlling AIDS is one of the main items in Millennium development goals; hence, by providing and promoting more preventive measures and educational programs particularly for those at-risk groups, we can achieve our desired goals.
Conclusion
In this study, we examined the characteristics of HIV-positive patients who referred to BDCC. Although the results of this study highlighted that injection addiction remains the major transmission route in Iran, the role of sexual transmission should be acknowledged in the future. Hence, prefect consideration should be given to this changing pattern. Finally, it has been pointed that protection against HIV is a multifaceted task and all community groups should be involved in this collaborative process.
Acknowledgements
The authors would like to thank the authorities as well as the personnel of Shiraz Behavioral Counseling Center and the patients who kindly cooperated in this study. The authors are also grateful to the Research gate Consulting Center of Shiraz University of Medical Sciences and Ms. N Shokrpour for her cooperation in improving the use of English in the manuscript.
Ethical issues
The study was approved by the Ethics Committee of the Shiraz University of Medical Sciences.
Cite this article as: Alimohamadi Y, Tabatabaee H, AfsarKazerooni P, Vahedi S, Enaami M, Teimourizad A. Epidemiologic characteristicsof HIV-positive patients referring to behavioral diseases consultation center in Shiraz, Iran.Med J Islam Repub Iran 2014 (14 December). Vol. 28:147.
References
- 1. World Heath Organization. Scaling up antiretroviral therapy in resource limited setting: guideline for a public health approach. Geneva: World Heath Organization 2005.
- 2.Fan HY, Conner RF, Villarreal LP. AIDS: science and society. Jones & Bartlett Learning. 2007 [Google Scholar]
- 3. Fauci AS, Braunwald E, Fauci A, Kasper D. Viral diseases. In: Fauci AS, Clifford L, editors. Harrison's principles of internal medicine 5th ed. New York: McGraw-Hill Medical New York; 2001.
- 4. Monahan F, Sands J, Marek J, Neighbors M, Phipps W. Medical-surgical nursing: health and illness perspectives. Philadelphia: Mosby; 2002.
- 5. Yaghobi R. HIV Infection. Tehran: Afshari publishing center; 1992.
- 6.Bastami F, Zareban E, Beiranvand A, Vahedi S. Effect of Educational Pamphlet on Knowledge and Attitude of Non-Medical Students about AIDS in University of Zabol in 2008. Health System Research. 2013;8(6) [Google Scholar]
- 7. Center for Disease Control and Prevention. About HIV/AIDS. Center for Disease Control and Prevention,; December 18, 2013; Available from: http://www.cdc.gov/hiv/basics/whatishiv.html.
- 8.Morison L. The global epidemiology of HIV/AIDS. British Medical Bulletin. 2001;58(1):7–18. doi: 10.1093/bmb/58.1.7. [DOI] [PubMed] [Google Scholar]
- 9.Simon V, D Ho D, Abdool Karim Q. HIV/AIDS epidemiology, pathogenesis, prevention, and treatment. Lancet. 2006;368:489–504. doi: 10.1016/S0140-6736(06)69157-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mohammadpour A, Parsa Yekta Z, Nikbakht Nasrabadi AR, Mohraz M. Coming to Terms With a Diagnosis of HIV in Iran: A Phenomenological Study. Association of Nurses in AIDS Care. 2009;20(4):249–59. doi: 10.1016/j.jana.2009.03.003. [DOI] [PubMed] [Google Scholar]
- 11. Center for Disease Control HIV / AIDS and Risky Behaviors. Hidden Harm,Bulletin of the Center for Disease Control HIV / AIDS and Risky Behaviors. Summer 2010.
- 12. Sedaghat A, Akbari M. Reporting on HIV and AIDS activities and achievements of the Islamic Republic of Iran. Tehran: Ministry of Health,Centre for Communicable Diseases Management; 2009.
- 13. National AIDS Committee Secretariat. On Monitoring of the United Nations General Assembly Special Session on HIV and AIDS-On Monitoring of the United Nations General Assembly Special Session on HIV and AIDS. March, 2012.
- 14. Declaration of Commitment on AIDS. Newyork: United Nations; 2001.
- 15.Kambou G, Devarajan S, Over M. The economic impact of AIDS in an African country: simulations with a computable general equilibrium model of Cameroon. Journal of African economies. 1992;1(1):109–30. [Google Scholar]
- 16.Ankrah EM. The impact of HIV/AIDS on the family and other significant relationships: the African clan revisited. AIDS care. 1993;5(1):5–22. doi: 10.1080/09540129308258580. [DOI] [PubMed] [Google Scholar]
- 17.Danziger R. The social impact of HIV/AIDS in developing countries. Social Science & Medicine. 1994;39(7):905–17. doi: 10.1016/0277-9536(94)90203-8. [DOI] [PubMed] [Google Scholar]
- 18.Travis P, Bennett S, Haines A, Pang T, Bhutta Z, Hyder AA, Pielemeier NR, Mills A, Evans T. Overcoming health-systems constraints to achieve the Millennium Development Goals. The Lancet. 2004;364(9437):900–6. doi: 10.1016/S0140-6736(04)16987-0. [DOI] [PubMed] [Google Scholar]
- 19. World Health Organization. HIV Surveillance in the WHO Eastern Mediterranean Region, Regional update 2012. 2013.
- 20.Ramezani A, Mohraz M, Gachkar L. Epidemiologic Situation of Human Immuno-deficiency Virus (HIV/AIDS Patients) in a Private Clinic in Tehran, Iran Archives of Iranian Medicine. 2006;9(4) [PubMed] [Google Scholar]
- 21.Rahimi-Movaghar A, Amin-Esmaeilia M, Haghdoostb A-a, Sadeghirad B, Mohraz M. HIV prevalence amongst injecting drug users in Iran: A systematic review of studies conducted during the decade 1998–2007. International Journal of Drug Policy. 2012;23(3):271–8. doi: 10.1016/j.drugpo.2011.09.002. [DOI] [PubMed] [Google Scholar]
- 22.Seyedalinaghi SA, Ostad Taghi Zadeh A, Zaresefat H, Hajizadeh M, Mohamadi SN, Paydary K, Emamzadeh Fard S, Hosseini M. Prevalence of HIV infection and the correlates among beggars in Tehran,Iran. Asian Pacific Journal of Tropical Disease. 2013;3(1):76–8. doi: 10.1016/S2221-1691(14)60210-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Moradi AR, Emdadi A, Soori B, Mostafavi E. Prevalence of Human Immunodeficiency Virus Infection among Injection Drug Users Released from Jail. Addict Health. 2012;14(3-4) [PMC free article] [PubMed] [Google Scholar]
- 24.Sabouri Ghannad M, Arab SM, Mirzaei M, Moinipur A. Epidemiologic Study of Human Immunodeficiency Virus (HIV) Infection in the Patients Referred to Health Centers in Hamadan Province, Iran AIDS Research and Human Retroviruses. 2009;25(3) doi: 10.1089/aid.2008.0143. [DOI] [PubMed] [Google Scholar]
- 25.Rabirad N, Mohammad Nejad E, Reza Hadizadeh M, Begjan J-o, Ehsani SR. The Prevalence of Tb in HIV Patients and Risk Factor With Frequent Referral (Iran, 2009-10) Iranian Red Crescent Medical Journal. 2013;15(1) doi: 10.5812/ircmj.4401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Katibeh M, Shariati B. Cost assessment in patients with HIV/AIDS. Acta Medica Iranica. 2008;46(6) [Google Scholar]
- 27.Davoudi S, Rasoolinejad M, Jafari S, Erfanzadeh M, Foroughi M, Hajiabdolbaghi M, Mohraz M. Prevalence of Hepatitis A Virus Infection in a HIV Positive Community. Acta Medica Iranica. 2010;48(3) [PubMed] [Google Scholar]
- 28.Kashi AH, Yadyad MJ, Hajiabdolbaghi M, Jafari S. Utilization of the Health Ministry recommended services by Iranian HIV/AIDS patients. Tehran University Medical Journal. 2008;66(9) [Google Scholar]
- 29. Ministry of Health. Current statistics on HIV/AIDS infection in Islamic Republic of Iran. Tehran: Center for Disease Management; 2011.
- 30.Ramezani A, Mohraz M, Yadegarinia D, Banifazl M, Gachkar L, Jam S, Aghakhani A, Eslamifar A, Yaghmaie F, Nemati K, Velayati AA. Prevalence of Dyslipidemia and Metabolic Abnormalities in HIV-Infected Patients. Acta Medica Iranica. 2008;47(2) [Google Scholar]