

Abstract
AIM
To evaluate the effects of chronic smoking on color vision in young subjects.
METHODS
This study included 91 smokers and 88 non-smokers (a total of 179 volunteers) without any ophthalmologic and systemical disorders. The subjects were between 18-40 years of age with a best corrected visual acuity (BCVA) of 20/20, normal anterior and posterior segment examinations and normal intraocular pressure. The color vision of the subjects were evaluated with Farnsworth-Munsell 100 Hue test (FMHT). The total error scores and axis calculation were performed for each subject and the results correlated.
RESULTS
Mean age and the standard deviation was 28±5y in the smokers group, and 26.7±5.5y in the control group (P=0.101). Sex distribution was similar in the two groups (P=0.365). There was no significant correlation between age and FMHT total error scores (P=0.069). Median of FMHT total error scores of smokers and non-smokers were 65 and 50.50, respectively. FMHT total error scores was found significantly higher in smokers than non-smokers (P=0.004). There was no statisticaly significant difference between smoker and non-smoker groups with respect to axis ratio calculation (P=0.611). There was no significant correlation with FMHT total error scores with neither smoking duration nor number of cigarettes smoked per day (P=0.405, P=0.454, respectively).
CONCLUSION
This study suggested that chronic smoking affects the color vision of young smokers but this may not be sector selective.
Keywords: cigarette smoking, color vision defect, vision test
INTRODUCTION
Smoking has many adverse effects on the human health. The association between smoking and visual system has been searched, and it is well known that there are many ophthalmologic diseases and conditions that have been associated with smoking such as cataracts, age-related macular degeneration, retinal ischemia, non-arteritic anterior ischemic optic neuropathy[1]–[5]. Additionally, Graves ophthalmopathy, conjunctival irritation, uveitis, refractive errors, glaucoma, tobacco-alcohol amblyopia are also associated with smoking[6]–[10]. There are a few studies pointing impaired color vision for smokers[11],[12]. Decreased color vision with decreased visual acuity (VA) and scotomas were also reported for smokers[13]. In our previous study we also found a higher total number of errors in the smokers than non-smokers[14].
Thousands of young individuals start smoking every day. Each day about 1000 persons younger than 18 years of age become new daily cigarette smokers which is an alarmingly serious health and socioeconomic problem[15]. The young smokers between the ages of 20 and 30 may be recruited in very important jobs such as military or civil aviation, electrical industry, or traffic signalling where many other lives may depend on the color vision integrity of such young smokers.
In this study we aimed to evaluate effects of smoking on color vision in young smokers with Farnsworth-Munsell 100 Hue test (FMHT) and investigate its correlation with several factors such as age, duration of smoking or sex.
SUBJECTS AND METHODS
Subjects
This study was conducted in 179 volunteers who were working as a staff or a student at Erciyes University School of Medicine in 2012 and 2013. The study was approved by the Institutional Review Board of the University. The research protocol adhered to the tenets of the Declaration of Helsinki for clinical research. Written informed consent was obtained from all the participants after explanation of the purpose and possible consequences of the study.
Methods
The inclusion criteria were: those between the ages of 18-40y without any systemical disease; with a best corrected VA (BCVA) of 20/20; and with normal anterior and posterior segment examination as well as normal intraocular pressure. Exclusion criteria were: those with a refractive error of more than ±2.00 diopters, a history of glaucoma, retinal pathology, previous ocular surgery and partial or total dyschromatopsia. Those with diabetes mellitus, arterial hypertension, chronic alcohol consumption and chronic drug abuse, pregnancy and a family history of dyschromatopsia were also excluded from the study. In the smokers group, subjects were smoking for at least one year. Number of cigarettes smoked each day and duration of smoking were recorded for the smokers. All the subjects were tested with FMHT. FMHT (Luneau, Paris, France), consists of four sub-sectors with a total of 85 caps. One cap subtends an angle of 1.4°. The colors of the caps in the first box are from red to yellowish green, in the second box from yellowish green to turquoise green, in the third box from turquoise green to bluish purple and in the fourth box from bluish purple to red. Subjects were asked to arrange the colors in an order from dark to light in each box.
Binocular FMHT was performed for all subjects in the same environment under the same illumination conditions. Subjects with refraction error performed the test with their glasses on. Total number of errors of all subjects were recorded. Figure 1A shows an example of FMHT of a smoker and Figure 1B shows an example of a non-smoker subject. FMHT results were also evaluated in a quadrant basis. This analysis allowed red-green and blue-yellow partition of total scores. Red-green partial number of errors were obtained from the addition of sector 2 (caps 13-33) and sector 4 (caps 55-75) and blue-yellow partial number of errors were obtained from the addition of sector 1 (caps 76-12) and sector 3 (caps 34-54). Axis determination was performed according to the report of Smith et al[16] subtracting the square root of red-green partial score (sector 2+4) from the square root of blue-yellow partial score (sector 1+3). Positive values indicate relatively greater number of blue-yellow errors or a blue-yellow axis whereas negative values indicate greater number of red-green errors or red-green axis.
Figure 1. FHMT results of smoking and non smoking subjects.
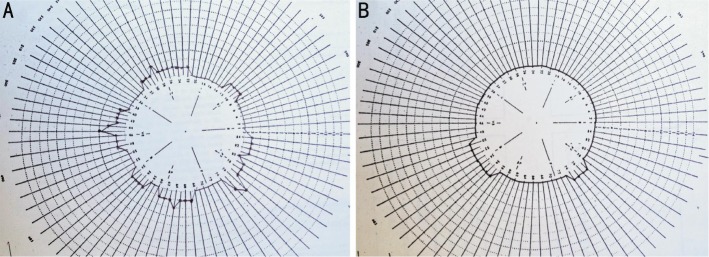
A: FMHT of a smoker. Total number of errors of this subject was 52. Sector 1+3=24 (blue-yellow partial number of errors) and sector 2+4=28 (red-green partial number of errors). B: FMHT of a non-smoker. Total number of errors of this subject was 12. Sector 1+3=7 (blue-yellow partial number of errors), sector 2+4=5 (red-green partial number of errors).
Statistical Analysis
In this study, statistical analysis was performed with non-parametric tests; Mann-Whitney U test, Spearman's correlation tests. Chi-square test was also used. All the calculations were made by the statistical package for the social sciences (SPSS®) version 15.0, on a Windows® based PC; P<0.05 was accepted as statistically significant.
RESULTS
Mean age (±SD) was 28±5y in the smokers group, and 26.7±5.5y in the control group (P=0.101). There were 34 females, 57 males in the smokers group whereas 39 females, 49 males in the control group (P=0.365). There was no statistically significant correlation between age and FMHT total number of errors for the entire population of 179 participants (P=0.069). Median total error score was significantly higher in the smoker group (65; range 12-221) than the control group (50.50; range 6-206; P=0.004). Higher ratio of blue-yellow axis errors were observed for both groups (75.6% for smokers, 71.6% for controls). The difference between the smoker and non-smoker groups was not statistically significant for any of the axes calculated (P=0.611). There was not a statistically significant difference between female and male participants of smokers regarding with median total error scores and also axis calculation.
In the smokers group mean smoking duration was 8.3±4.9y in women and 9.2±5.5y in men. The difference was not statistically significant (P=0.553). Mean number of cigarettes was 12±6 per day in women and 17±8 in men. The difference was statistically significant (P=0.003). There was no significant correlation with FMHT total error scores with neither smoking duration nor number of cigarettes smoked per day in the whole smokers group (P=0.405, P=0.454, respectively).
There were 36 subjects smoking 0-10 cigarettes, 11 subjects smoking 11-19 cigarettes and 44 subjects smoking 20 or more cigarettes per day. There was not a significant correlation between both the total number of errors in the FHMT and axis calculation and the number of cigarettes smoked per day in all subgroups (P=0.284, P=0.739, respectively). There were 52 subjects smoking 10y and less and 39 subjects smoking more than 10y. There was no significant correlation between both the total number of errors in the FHMT and axis calculation and smoking duration in all subgroups (P=0.261, P=0.460, respectively). All statistical parameters related with subgroups according to both smoking duration and number of cigarettes smoked per day were shown at Tables 1 and 2.
Table 1. Statistical parameters according to subgroups of cigarettes smoked per day.
| Subgroups of number of cigarettes smoked per day | n | FMHT total scores P | Axis calculation P |
| 0-10 | 36 | 0.284 | 0.739 |
| 11-19 | 11 | ||
| 20 and more | 44 |
FMHT: Farnsworth-Munsell 100 Hue test.
Table 2. Statistical parameters according to subgroups of duration of smoking.
| Subgroups of duration of smoking | n | FMHT total scores P | Axis calculation P |
| 10y and less | 52 | 0.261 | 0.460 |
| More than 10y | 39 |
FMHT: Farnsworth-Munsell 100 Hue test.
DISCUSSION
Adverse effects of smoking on the retina have been shown in many studies, causing color vision disturbances, visual field defects and even blindness. Exact mechanism is still unknown but several hypotheses have been suggested[17]–[19]. Reduced antioxidants, increased free radicals and lipid peroxidation were suggested as the etiopathogenetic mechanism[20],[21]. Another suggested mechanism is reduced choroidal blood supply, ischemia, hypoxia and micro-infarcts leading to macular degeneration[22]. Furthermore, smoking can cause a reduction in the carotenoids, lutein and zeaxhantin which are antioxidants[23]. Those mechanisms may affect cone receptor cells which have a high density in the fovea thus can lead to color vision disturbances.
The risk of becoming a smoker among young adults who have never smoked is high; 14% will become smokers between the ages of 18 and 24y[24]. This is a serious health and socioeconomic problem. The young smokers between the ages of 20 and 30y may be recruited in very important jobs such as military or civil aviation, electrical industry, or traffic signalling where many other lives may depend on the color vision integrity of such young smokers.
Smoking affects ocular vascular system by reducing retinal blood flow and can cause irregularites in the small retinal vessels[25]. There are limited number of publications in the scientific literature about the effects of smoking on color vision. Erb et al[11] compared color vision with Roth-28 Hue test of 20 subjects smoking less than 20 cigarettes per day with non-smokers. Although they did not find any difference between these groups, there was a significantly higher total error scores in the 32 subjects smoking more than 20 cigarettes than non-smokers. The authors suggested that this was related to accumulation of toxic substances in the retinal pigment epithelium. In our study we found that there was no correlation between the total number of errors and the number of cigarettes smoked per day or between the duration of smoking.
Voke and Fletcher[26] showed that carbon monoxide and cigarette smoking can be the cause of red-green dyschromatopsia. On the other hand, some authors suggested that toxic neuropathy related to smoking affects especially red-green color vision[27].
In our study, we found that although there was a significant difference between total number of errors of smokers and non-smokers, we did not find any significant difference between the groups with respect to red-green and blue-yellow sectors. We suggest that a diffuse pathology rather than a sector selective pathology may be involved in chronic smokers.
Although there are limited number of studies associated with this topic in the literature, the results of our study must be evaluated within the context of its limitations. The main limitation of the study is that the groups have a relatively small sample size. In addition, this is the first study in the literature evaluating partial (sectorial) scores (red-green or blue-yellow). The age of the participants were also considerably young; however, we aimed at avoiding the influence of age related additional retinal pathologies which could affect the results. The other limitation is the intellectual level of cases; all of the participants were choosen from the university personnel with higher intellectual level.
In conclusion, our study shows that smoking has an adverse effect on the color vision of smokers evidenced by increased total number of errors found in the FMHT, however this may not be necessarily sector selective in young subjects. Further studies which would include subjects who gave up smoking after various durations of smoking may also be necessary to clarify the effects of chronic smoking in young subjects.
Acknowledgments
Conflicts of Interest: Arda H, None; Mirza GE, None; Polat OA, None; Karakucuk S, None; Oner A, None; Gumus K, None.
REFERENCES
- 1.Solberg Y, Rosner M, Belkin M. The association between cigarette smoking and ocular diseases. Surv Ophthalmol. 1998;42(6):535–547. doi: 10.1016/s0039-6257(98)00002-2. [DOI] [PubMed] [Google Scholar]
- 2.Lindblad BE, Hakansson N, Wolk A. Smoking cessation and the risk of cataract: a prospective cohort study of cataract extraction among men. JAMA Ophthalmol. 2014;132(3):253–257. doi: 10.1001/jamaophthalmol.2013.6669. [DOI] [PubMed] [Google Scholar]
- 3.Velilla S, Garcia-Medina JJ, Garcia-Layana A, Dolz-Marco R, Pons-Vazquez S, Pinazo-Duran MD, Gomez Ulla F, Arevalo JF, Diaz-Llopis M, Gallego-Pinazo R. Smoking and age-related macular degeneration: review and update. J Ophthalmol. 2013;2013:895147. doi: 10.1155/2013/895147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Klein R, Cruickshanks KJ, Nash SD, Krantz EM, Nieto FJ, Huang GH, Pankow JS, Klein BE. The prevalence of age-related macular degeneration and associated risk factors. Arch Ophthalmol. 2010;128(6):750–758. doi: 10.1001/archophthalmol.2010.92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wiersinga WM. Smoking and thyroid. Clin Endocrinol (Oxf) 2013;79(2):145–151. doi: 10.1111/cen.12222. [DOI] [PubMed] [Google Scholar]
- 6.Ozer HT, Gunesacar R, Dinkci S, Ozbalkan Z, Yıldız F, Erken E. The impact of smoking on clinical features of Behçet's disease patients with glutathione S-transferase polymorphisms. Clin Exp Rheumatol. 2012;30(3 Suppl):S14–17. [PubMed] [Google Scholar]
- 7.Roesel M, Ruttig A, Schumacher C, Heinz C, Heiligenhaus A. Smoking complicates the course of non-infectious uveitis. Graefes Arch Clin Exp Ophthalmol. 2011;249(6):903–907. doi: 10.1007/s00417-010-1597-1. [DOI] [PubMed] [Google Scholar]
- 8.Wise LA, Rosenberg L, Radin RG, Mattox C, Yang EB, Palmer JR, Seddon JM. A prospective study of diabetes, lifestyle factors, and glaucoma among African-American women. Ann Epidemiol. 2011;21(6):430–439. doi: 10.1016/j.annepidem.2011.03.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gryzbowski A. Present knowledge on the effects of smoking tobacco on the eye diseases. Przegl Lek. 2008;65(10):724–727. [PubMed] [Google Scholar]
- 10.Lois N, Abdelkader E, Reglitz K, Garden C, Ayres JG. Environmental tobacco smoke exposure and eye disease. Br J Ophthalmol. 2008;92(10):1304–1310. doi: 10.1136/bjo.2008.141168. [DOI] [PubMed] [Google Scholar]
- 11.Erb C, Nicaeus T, Adler M, Isensee J, Zrenner E, Thiel HJ. Colour vision disturbances in chronic smokers. Graefes Arch Clin Exp Ophthalmol. 1999;237(5):377–380. doi: 10.1007/s004170050247. [DOI] [PubMed] [Google Scholar]
- 12.Bimler D, Kirkland J. Multidimensional scaling of D15 caps: color-vision defects among tobacco smokers? Vis Neurosci. 2004;21(3):445–458. doi: 10.1017/s0952523804213116. [DOI] [PubMed] [Google Scholar]
- 13.Chisholm IA. Quantitative assessment of colour vision in tobacco amblyopia. Proc R Soc Med. 1970;63(8):792. doi: 10.1177/003591577006300824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Arda H, Oner A, Gumus K, Karaca C, Karakucuk S, Mirza E. Evaluation of colour vision in smokers with the Farnsworth-Munsell 100 hue test: preliminary results. Journal of Retina-Vitreous. 2010;18(2):139–142. [Google Scholar]
- 15.Substance Abuse and Mental Health Services Administration (SAMHSA), HHS, Calculated based on data in National Household Survey on Drug Abuse, 2001 Preventing tobacco use among youth and young adults: a report of the surgeon general, 2012. http://www.surgeongeneral.gov/library/reports/preventing-youth-tobacco-use/
- 16.Smith VC, Pokorny J, Pass AS. Color-axis determination on the Farnsworth-Munsell 100-Hue test. Am J Ophthalmol. 1985;100(1):176–182. doi: 10.1016/s0002-9394(14)75002-0. [DOI] [PubMed] [Google Scholar]
- 17.Smith W, Assink J, Klein R, Mitchell P, Klaver CC, Klein BE, Hofman A, Jensen S, Wang JJ, de Jong PT. Risk factors for age related macular degeneration: pooled findings from three continents. Ophthalmology. 2001;108(4):697–704. doi: 10.1016/s0161-6420(00)00580-7. [DOI] [PubMed] [Google Scholar]
- 18.Cong R, Zhou B, Sun Q, Gu H, Tang N, Wang B. Smoking and the risk of age-related macular degenaration: a meta analysis. Ann epidemiol. 2008;18(8):647–656. doi: 10.1016/j.annepidem.2008.04.002. [DOI] [PubMed] [Google Scholar]
- 19.Neuner B, Komm A, Wellmann J, Dietzel M, Pauleikhoff D, Walter J, Busch M, Hense HW. Smoking history and the incidence of age-related macular degenaration--results from the Muenster Aging and Retina Study (MARS) cohort and systemiatic review and meta analysis of observational longitudinal studies. Addict Behav. 2009;34(11):938–947. doi: 10.1016/j.addbeh.2009.05.015. [DOI] [PubMed] [Google Scholar]
- 20.Chow CK, Thacker RR, Changchit C, Bridges RB, Rehm SR, Humble J, Turberk J. Lower levels of vitamin C and carotenes in plasma of cigarette smokers. J Am Coll Nut. 1986;5(3):305–312. doi: 10.1080/07315724.1986.10720134. [DOI] [PubMed] [Google Scholar]
- 21.Church DF, Pryor WA. Free-radical chemistry of cigarette smoke and its toxicological implications. Environ Health Perspect. 1985;64:111–126. doi: 10.1289/ehp.8564111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bettman JW, Fellows V, Chao P. The effect of cigarette smoking on the intraocular circulation. AMA Arch Ophthalmol. 1958;59:481–488. doi: 10.1001/archopht.1958.00940050037002. [DOI] [PubMed] [Google Scholar]
- 23.Werner JS, Steele VG. Sensitivity of human foveal color mechanisms throughout the life spen. J Opt Soc Am. 1988;5(12):2122–2130. doi: 10.1364/josaa.5.002122. [DOI] [PubMed] [Google Scholar]
- 24.O'Loughlin JL, Dugas EN, O'Loughlin EK, Karp I, Sylvestre MP. Incidence and determinants of cigarette smoking initiation in young adults. J Adolesc Health. 2014;54(1):26–32. doi: 10.1016/j.jadohealth.2013.07.009. [DOI] [PubMed] [Google Scholar]
- 25.Morgado PB, Chenc HC, Patel V, Herbert L, Kohner EM. The acute effect of smoking on retinal blood flow in subjects with and without diabetes. Ophthalmology. 1994;101(7):1220–1226. doi: 10.1016/s0161-6420(94)31185-7. [DOI] [PubMed] [Google Scholar]
- 26.Voke J, Fletcher R. London: Adam Hilger; 1985. Defective colour vision: fundamentals, diagnosis and management. [Google Scholar]
- 27.Krastel H, Moreland JD. In inherited and acquired colour vision deficiencies. In: Foster D.H., editor. Colour vision deficiencies in ophthalmic diseases. Basingstoke, UK: MacMillan; 1991. pp. 115–172. [Google Scholar]