

Abstract
Background:
Dental anxiety is a major barrier for dental care utilization. Hence, identifying anxious individuals and their appropriate management becomes crucial in clinical practice.
Aim:
The study aims to assess dental anxiety, factors influencing dental anxiety, and anxiety towards tooth extraction procedure among patients attending a dental hospital in India.
Materials and Methods:
The study sample consisted of 1,148 consecutive patients aged 18-70 years. The assessment tools consisted of a consent form, history form, a questionnaire form containing the Modified Dental Anxiety Scale (MDAS) which was used to assess the level of dental anxiety, and an additional question on anxiety towards dental extraction procedure.
Results:
Among the study group, 63.7% were men and 36.3% were women. Based on the MDAS score, 45.2% of the participants were identified to be less anxious, 51.8% were moderately or extremely anxious, and 3% were suffering from dental phobia. Mean MDAS total score was 10.4 (standard deviation (SD) = 3.91). Female participants and younger subjects were more anxious (P < 0.001). Subjects who were anxious had postponed their dental visit (P < 0.001). Participants who had negative dental experience were more anxious (P < 0.05). Notably, 82.6% reported anxiety towards extraction procedure. Significant association was seen between anxiety towards extraction procedure and the respondents gender (P < 0.05), age (P < 0.001), education level (P < 0.05), employment status (P < 0.001), income (P < 0.001), self-perceived oral health status (P < 0.05), and their history of visit to dentist (P < 0.05).
Conclusion:
Significant percentage of population was suffering from dental anxiety in this study population. A plethora of factors like age, gender, education level, occupation, financial stability, and previous bad dental experience influences dental anxiety to various levels. Extraction followed by drilling of tooth and receiving local anesthetic injection provoked more anxiety.
Keywords: Dental anxiety, Extraction, Modified Dental Anxiety Scale, Self-report, Tamil population
Introduction
Oral health has a significant impact on the quality of life, appearance, and self-esteem of a person.[1] Dental anxiety affects a significant proportion of people of all ages from different social classes. It remains to be a serious concern for both the dental practitioner and the patient for the provision of routine dental care on a day-to-day basis.[2] Modified Dental Anxiety Scale (MDAS) is commonly used to measure anxiety. This was modified from the original Corah's Dental Anxiety Scale (CDAS). Advantage of the MDAS is because of its brevity, it is simple, easy to complete, and can be used as a cost-effective instrument for population-based research.[3,4] It has been found to be reliable and valid cross culturally, and has been translated into different languages.[5,6,7,8] This scale includes a series of five questions to be presented to the participants and they are asked to rate the level of anxiety they would feel if they were in a particular dental situations.
Tooth extraction is said to provoke more anxiety and is perceived as a stressful experience due to physical and psychological impact.[9] Identifying anxious individuals can enable the dentist to anticipate patient's behavior and be better equipped with measures to help alleviate patient's anxiety.
The current study aims to measure and evaluate factors influencing dental anxiety using MDAS. Due to limited availability of published data concerning anxiety for extraction procedure and its associated sociodemographic variables, we aimed to assess the same among the adult patients attending a dental hospital in Chennai.
Materials and Methods
The study was conducted from March 2012 to February 2013. Approval for the study was obtained from the institutional ethical committee of SRM Dental College and Hospital, Chennai. Convenience sampling was done and 1,148 consecutive patients aged 18-70 years, attending the Outpatient Department with varied dental problems were recruited. Only subjects who were native of Tamil Nadu with Tamil as their mother tongue were requested to participate in the study. The purpose of the study was explained to each patient and both written as well as verbal informed consent were obtained from those who agreed to participate. Those who refused to give informed consent, non-natives of Tamil Nadu or immigrants, those who were undergoing psychiatric therapy, suffering from Generalized Anxiety Disorders (GAD), and completely edentulous patients were excluded from the study.
The patients were asked to fill a history form which was used to obtain information on age, gender, educational qualification (categorized as incomplete/completed school, degree/diploma, postgraduation, and uneducated), occupation (choices were employed, unemployed, student, and retired from work), income (categorized as earning less than 10,000 Indian rupees; earning between 10,001 and 20,000 Indian rupees; more than 20,000 Indian rupees; and no income), details of previous dental visit, duration since the last visit to dentist (options were within last 6 months, last 6 months-1 year, before 1-2 years, and more than 2 years back), previous dental experience, self-perceived oral health status (choices given were excellent, good, fair, and poor), and postponement of dental treatment due to dental anxiety. To assess their level of anxiety the patients were asked to complete the MDAS administered in both Tamil and English language. In addition to MDAS, a question on anxiety towards dental extraction was included in the questionnaire as follows “How anxious would you feel, if you were about to have your tooth/teeth extracted?” and the patients were asked to choose the answer from Likert scale responses such as “not anxious, slightly anxious, fairly anxious, very anxious, or extremely anxious”.
Statistical analysis
Data was analyzed using IBM version 20 software. Mean total MDAS score was calculated for all the categorized variables. Independent sample t-test and one-way analysis of variance (ANOVA) was done to compare mean total MDAS score between categories in a group. Spearman rank correlation was done to assess the strength of association between MDAS and anxiety towards extraction. Chi-square test was used to evaluate the association between anxiety towards extraction and the variables.
Results
Among the 1,148 respondents, 63.7% were males and 36.3% were females. Mean age of the participants was 27.9 years (standard deviation (SD) =11.27) and it was seen that majority of the respondents belonged to age group ≤30 years (71.3%). Mean total score for dental anxiety on MDAS was 10.4 (SD = 3.91). Based on the MDAS score, 45.2% of the subjects were identified to be less anxious (5-9 total score), 51.8% were moderately or extremely anxious (10-18 total score), and 3% ≥19 total score) were suffering from dental phobia [Table 1].
Table 1.
Shows descriptive statistics, mean total score MDAS, and statistical test
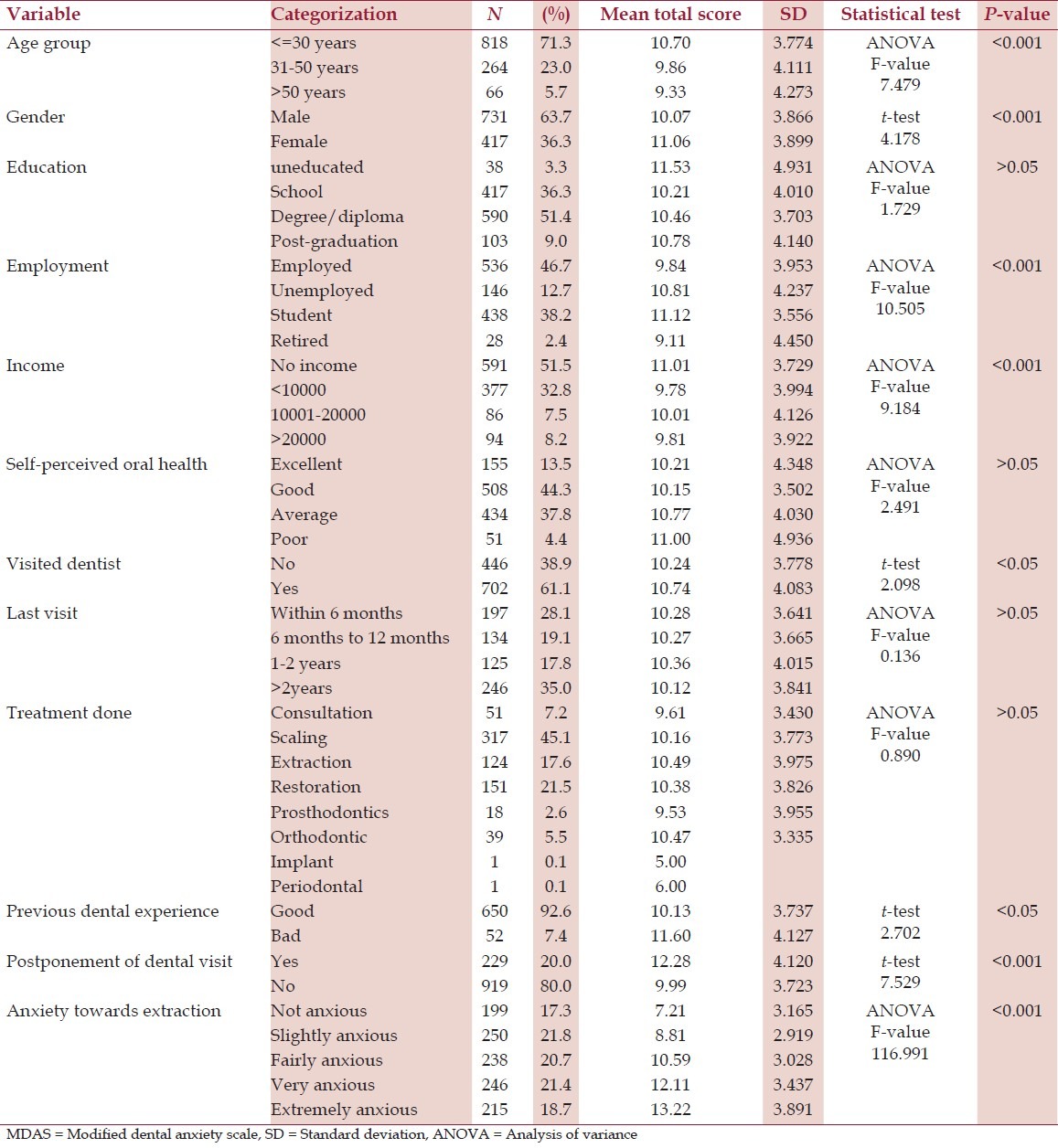
Descriptive statistics and the factors influencing anxiety, with the relevant statistical test - analysis of variance (ANOVA) and t-test (post hoc ANOVA not shown in Table) and P-values are shown in Table 1. Female participants were more anxious than their male counterparts (P < 0.001), further it was noticed that younger subjects were more anxious (P < 0.001) and post hoc showed a significant difference in anxiety level between the samples based on their age groups (P < 0.05). Among the respondents it was seen that students, unemployed, and uneducated participants reported more anxiety towards dental treatment procedures (P < 0.001), post hoc showed a significant difference in anxiety level between those who were employed and unemployed (P < 0.05). Evaluation of economic status with anxiety level revealed that respondents who had no income or were dependent on another family member financially were more anxious than those who were financially independent, there was highly significant variance (P < 0.001) among samples based on their income and post hoc showed a significant difference in anxiety between no income group and high income group (P < 0.05). It was also seen that extremely anxious subjects had postponed their dental visit (P < 0.001). Similarly, samples that had negative dental experience were more anxious and significant difference (P < 0.05) was seen in anxiety level between those who have had previous good or bad dental experience.
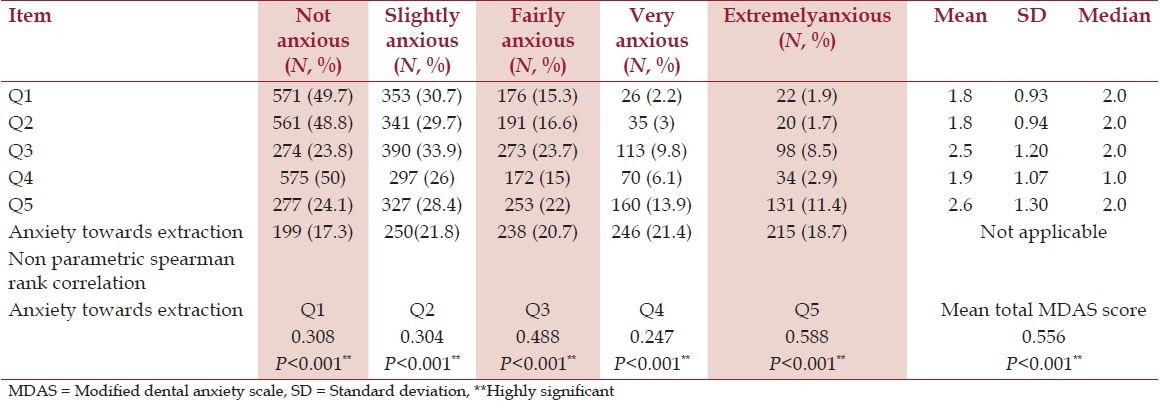
The mean, standard deviation, and median of the five anxiety-provoking stimuli were evaluated on MDAS. On analysis it was observed that 49.7% of the respondents were not anxious regarding their dental visit, 49% felt that they would not be anxious while sitting in the waiting room for their appointment, 76% felt that getting their tooth drilled or receiving local anesthetic injection would make them anxious, and 11.4% felt that they would be extremely anxious if they have to receive injection in their mouth. On assessment of extraction as an anxiety-provoking stimuli, it was seen that majority of the participants, that is, 82.6% reported anxiety and among them 18.7% felt that they would be extremely anxious if they have to extract their tooth. Spearman rank correlation analysis between MDAS and anxiety towards extraction procedure showed a highly significant correlation (P < 0.001) [Table 2]. Among the stimuli assessed in this study, it was identified that extraction followed by drilling of tooth and receiving local anesthetic injection provoked more anxiety in descending order.
Table 2.
Frequency distribution (percentage), mean, median, and standard deviation of the questions assessed in the study. Correlation between anxiety towards extraction and MDAS scale
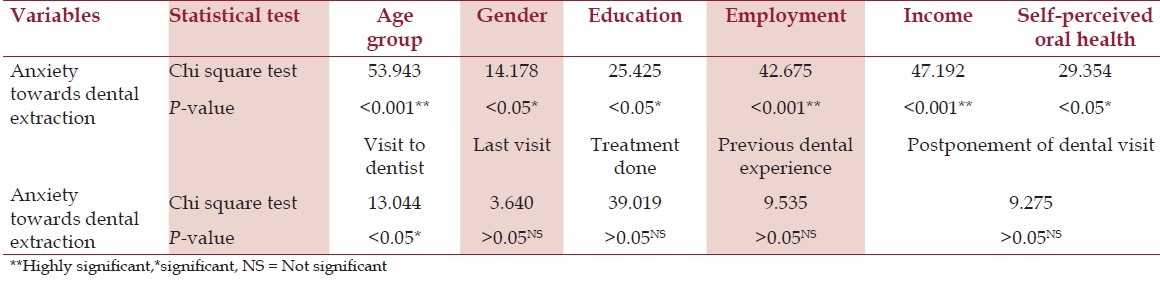
Chi-square analysis was done for factors influencing anxiety concerning extraction of tooth. Significant association was seen with the respondents gender (P < 0.05), age group (P < 0.001), education level (P < 0.05), employment status (P < 0.001), and income (P < 0.001). The subjects self-perceived oral health status and their visit to dentist were also significantly associated (P < 0.05) with anxiety towards extraction. Analysis showed that increased anxiety for extraction was associated with higher mean total MDAS score, variance, and post hoc was also highly significant within the groups (P < 0.001) [Table 3].
Table 3.
Association between anxiety towards extraction and the variables analyzed using chi-square test
Discussion
Findings of the present study and from different states of India like Gujarat and Haryana indicate that there is a higher prevalence of dental anxiety among the Indian population when compared with that of Western countries.[10,11,12] This could be attributed to multiple factors like poor oral health awareness, ignorance about dental treatment procedures, superstitious and false beliefs about dental treatment, cultural differences, and views from members of the family (highly regarded in this society, hence any unpleasant dental experience will influence others attitude towards dental therapy). It was observed that among those who participated in the study, only 3% were suffering from dental phobia which was in agreement with the other Indian studies.[11,13,14] Dentally phobic individuals were considerably fewer in this population in comparison with industrialized countries like UK, Turkey, and North Ireland.[4,5,15]
Comparison between genders to evaluate the prevalence of dental anxiety showed that female subjects were more anxious than male counterparts, plausible explanation for such observation could be attributed to the fact that women usually admit their fears readily than men, have lower tolerance to pain, and exhibit higher level of neuroticism.[10,11,14,16] It was seen that younger participants were more anxious, and with increasing age there seems to be a decrease in the level of anxiety; such a trend has been reported widely from several studies,[11,16] but refuted by Tunc et al.,[5] Thomson et al.,[17] and Nair et al.[14] Decline in anxiety with age could be due to age-dependent cerebral deterioration, factors like extinction or habituation, adaptive resignation towards the inevitable, increased ability to cope with experience, ageing process itself, more exposure to debilitating diseases, and treatment.[18]
Subjects who were uneducated, unemployed, and financially dependent scored high on the anxiety scale; it could be argued that educated people cope better and rationalize a situation rather than avoiding it and also lower socioeconomic conditions leads to poor physical health, more psychological problems like depression and anxiety, less access to healthcare, and hence more fear and anxiety.[10] It is hypothesized that, anxious individuals and those with past negative dental experience usually postpone their visit to dentist, similar behavior was seen among this study population; thereby, concurring with the observations of Nicolas et al.,[12] Acharya,[13] and Kumar et al.[19]
Oosterink and colleagues administered a questionnaire describing 67 potentially anxiety-provoking dental stimuli and their results indicated that invasive stimuli like surgical procedures were rated as the most anxiety-provoking and noninvasive stimuli were the least anxiety provoking.[20] Similar observation by Naidu and Lalwah[21] among a sample of West Indian adults indicated that half the participants were extremely anxious for drilling of tooth, injections, and extraction. Previous unpleasant experience with injections and extractions seemed to influence the anxiety levels.[21,22,23]
Dubey et al., in their study reported that prevalence of tooth loss is high among adults in India and over half of the general population had experienced tooth loss with greater prevalence of tooth mortality in rural, low socioeconomic status people when compared with urban residents.[24] Observational study by George et al.,[25] among adults in Chennai showed 45.5% prevalence of permanent tooth loss, in addition people belonging to lower socioeconomic status had more number of missing teeth. In developing countries like India, more patients opt for tooth removal due to multiple factors like ignorance, lower socioeconomic status, time restraints, high cost for restoration of tooth, irregular and symptomatic dental visit, and poor oral health awareness. In clinical practice, it is not uncommon to encounter patients who interrupt extraction procedure despite adequate anesthesia, hence failure to identify anxiety leads to stressful and embarrassing situation for the dentist. Liau et al.,[26] in their study reported that high anxiety, younger age, and traumatic dental history were correlated with greater increase in heart rate during the administration of local dental anesthesia for tooth removal. An astounding finding was that 82.6% of the subjects in this study were anxious regarding extraction procedure, this is in agreement with the findings of Nair et al.,[14] Naidu and Lalwah,[21] Liau et al.,[26] and among the stimuli assessed extraction had the highest rating.
Limitations of the study are cross sectional design, convenience sampling, and self-assessment questionnaire can be biased when eliciting responses and very few anxiety-provoking stimuli were assessed in this study.
Conclusion
Thus, from the current study it can be concluded that dental anxiety was highly prevalent in this population; moreover, among the five anxiety-provoking stimuli assessed it was apparent that dental extraction provoked more anxiety followed by drilling of tooth and injection of local anesthetic agent. Summarily, this research work highlights crucial findings of importance in the field of dental anxiety which could be of significance to dental practitioners and researchers, thereby enabling them to pursue better patient management strategies and policy making.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.McGrath C, Bedi R. The association between dental anxiety and oral health-related quality of life in Britain. Community Dent Oral Epidemiol. 2004;32:67–72. doi: 10.1111/j.1600-0528.2004.00119.x. [DOI] [PubMed] [Google Scholar]
- 2.Eitner S, Wichmann M, Paulsen A, Holst S. Dental anxiety: An epidemiological study on its clinical correlation and effects on oral health. J Oral Rehabil. 2006;33:588–93. doi: 10.1111/j.1365-2842.2005.01589.x. [DOI] [PubMed] [Google Scholar]
- 3.Corah NL. Development of a dental anxiety scales. J Dent Res. 1969;48:596. doi: 10.1177/00220345690480041801. [DOI] [PubMed] [Google Scholar]
- 4.Humphris GM, Morrison T, Lindsay SJ. The Modified Dental Anxiety Scale: Validation and United Kingdom norms. Community Dent Health. 1995;12:143–50. [PubMed] [Google Scholar]
- 5.Tunc EP, Firat D, Onur OD, Sar V. Reliability and validity of the Modified Dental Anxiety Scale (MDAS) in a Turkish population. Community Dent Oral Epidemiol. 2005;33:357–62. doi: 10.1111/j.1600-0528.2005.00229.x. [DOI] [PubMed] [Google Scholar]
- 6.Appukuttan D, Datchnamurthy M, Deborah SP, Hirudayaraj GJ, Tadepalli A, Victor DJ. Reliability and validity of the Tamil version of Modified Dental Anxiety Scale. J Oral Sci. 2012;54:313–20. doi: 10.2334/josnusd.54.313. [DOI] [PubMed] [Google Scholar]
- 7.Coolidge T, Arapostathis KN, Emmanouil D, Dabarakis N, Patrikiou A, Economides N, et al. Psychometric properties of Greek versions of the Modified Corah Dental Anxiety Scale (MDAS) and the Dental Fear Survey (DFS) BMC Oral Health. 2008;8:29. doi: 10.1186/1472-6831-8-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yuan S, Freeman R, Lahti S, Lloyd-Williams F, Humphris G. Some psychometric properties of the Chinese version of the Modified Dental Anxiety Scale with cross validation. Health Qual Life Outcomes. 2008;6:22. doi: 10.1186/1477-7525-6-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rodriguez Vazquez LM, Rubinos Lopez E, Varela Centelles A, Blanco Otero AI, Varela Otero F, Varela Centelles P. Stress amongst primary dental care patients. Med Oral Patol Oral Cir Bucal. 2008;13:E253–6. [PubMed] [Google Scholar]
- 10.Malvania EA, Ajitkrishnan CG. Prevalence and socio demographic correlates of dental anxiety among group of adult patients attending a dental institution in Vadodara city, Gujarat, India. Indian J Dent Res. 2011;22:179–80. doi: 10.4103/0970-9290.79989. [DOI] [PubMed] [Google Scholar]
- 11.Marya CM, Grover S, Jnaneshwar A, Pruthi N. Dental anxiety among patients visiting a dental institute in Faridabad, India. West Indian Med J. 2012;61:187–90. [PubMed] [Google Scholar]
- 12.Nicolas E, Collado V, Faulks D, Bullier B, Hennequin M. A national cross-sectional survey of dental anxiety in the French adult population. BMC Oral Health. 2007;7:12. doi: 10.1186/1472-6831-7-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Acharya S. Factors affecting dental anxiety and beliefs in an Indian population. J Oral Rehabil. 2008;35:259–67. doi: 10.1111/j.1365-2842.2007.01777.x. [DOI] [PubMed] [Google Scholar]
- 14.Nair MA, Shankarapillai R, Chouhan V. The dental anxiety levels associated with surgical extraction of tooth. Int J Dent Clin. 2009;1:20–3. [Google Scholar]
- 15.Humphris G, Freeman R, Campbell J, Tuutti H, D'Souza V. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int Dent J. 2000;50:370–6. doi: 10.1111/j.1875-595x.2000.tb00570.x. [DOI] [PubMed] [Google Scholar]
- 16.Sanikop S, Agrawal P, Patil S. Relationship between dental anxiety and pain perception during scaling. J Oral Sci. 2011;53:341–8. doi: 10.2334/josnusd.53.341. [DOI] [PubMed] [Google Scholar]
- 17.Thomson WM, Locker D, Poulton R. Incidence of dental anxiety in young adults in relation to dental treatment experience. Community Dent Oral Epidemiol. 2000;28:289–94. doi: 10.1034/j.1600-0528.2000.280407.x. [DOI] [PubMed] [Google Scholar]
- 18.Locker D, Liddell AM. Correlates of dental anxiety among older adults. J Dent Res. 1991;70:198–203. doi: 10.1177/00220345910700030801. [DOI] [PubMed] [Google Scholar]
- 19.Kumar S, Bhargav P, Patel A, Bhati M, Balasubramaniyam G, Duraiswamy P, et al. Does Dental anxiety influence oral health related quality of life. Observations from a cross sectional study among adults in Udaipur district, India? J Oral Sci. 2009;51:245–54. doi: 10.2334/josnusd.51.245. [DOI] [PubMed] [Google Scholar]
- 20.Oosterink FM, de Jongh A, Aartman IH. What are people afraid of during dental treatment. Anxiety-provoking capacity of 67 stimuli characteristic of the dental setting? Eur J Oral Sci. 2008;116:44–51. doi: 10.1111/j.1600-0722.2007.00500.x. [DOI] [PubMed] [Google Scholar]
- 21.Naidu RS, Lalwah S. Dental anxiety in a sample of West Indian adults. West Indian Med J. 2010;59:569–72. [PubMed] [Google Scholar]
- 22.Brukiene V, Aleksejuniene J, Balciuniene I. Is dental treatment experience related to dental anxiety. A cross-sectional study in Lithuanian adolescents? Stomatologija. 2006;8:108–15. [PubMed] [Google Scholar]
- 23.Ekanayake L, Dharmawardena D. Dental anxiety in patients seeking care at the university dental hospital in Sri Lanka. Community Dent Health. 2003;20:112–6. [PubMed] [Google Scholar]
- 24.Dubey RK, Gupta DK, Shetty P. Current status of edentulousness in India: Systematic review. Chhattisgarh J Health Sci. 2013;1:72–6. [Google Scholar]
- 25.George B, John J, Saravanan S, Arumugham IM. Prevalence of permanent tooth loss among children and adults in a suburban area of Chennai. Indian J Dent Res. 2011;22:364. doi: 10.4103/0970-9290.84284. [DOI] [PubMed] [Google Scholar]
- 26.Liau FL, Kok SH, Lee JJ, Kuo RC, Hwang CR, Yang PJ, et al. Cardiovascular influence of dental anxiety during local anesthesia for tooth extraction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:16–26. doi: 10.1016/j.tripleo.2007.03.015. [DOI] [PubMed] [Google Scholar]