

Abstract
Background:
The number of women who select cesarean section due to fear of childbirth has increased. Role play education seems to be a helpful method to remove or reduce the fear of childbirth. Therefore, this study aimed to investigate the effect of role play education on primiparous women's fear of natural delivery and their decision on the mode of delivery.
Materials and Methods:
In this blind clinical trial, 67 primiparous women with natural pregnancy at 34–36 weeks of gestational age and with no indication of cesarean section were selected from the health care centers in Mashhad. They were randomly assigned to two groups who underwent pre-test and post-test with the help of delivery attitude questionnaire to investigate their fear of childbirth and a researcher-made pregnant women's decision investigation questionnaire. Education through role play was conducted in the form of three scenarios during seven stages. The findings were analyzed by Fisher's exact test and independent t-test through SPSS.
Results:
The two groups were significantly different concerning the fear of childbirth after the intervention (P = 0.007), and the fear score showed a higher reduction in the role play group compared to the lecture group. There was a significant difference between the two groups concerning the reduction of elective cesarean section and the decision on the mode of delivery at the time of admission in the labor room (P = 0.000). About 75% in the lecture group and 100% in the role play group selected natural delivery.
Conclusions:
In the present study, the effect of role play was more in making a decision on natural delivery, reducing the fear of childbirth, and reducing the rate of elective cesarean section. It is suggested to use role play method to educate pregnant women to reduce the rate of cesarean sections.
Keywords: Decision, fear of childbirth, lecture, mode of delivery, role play
INTRODUCTION
From the time of Adam's creation, God has gifted humans with delivery to have offspring. It is a spontaneous process that needs no intervention, and cesarean section (CS) is conducted only when natural delivery is contraindicated to protect mother's and infant's health.[1] Nowadays, unfortunately, having a CS has become a culture for escaping pain and has influenced public health. This is when CS imposes more risk to the mother, compared to vaginal delivery, and includes complications such as endomyometritis, bleeding, thromboembolism, preterm labor and mortality (in mother), and respiratory distress syndrome, resistant pulmonary hypertension, and damages like injury, bruise, or other traumas in infant.[2]
The incidence of cesarean delivery (CD) is 10–15% worldwide, while in some Iranian cities it is reported as 47%.[3] Some studies report that 65% of CS conducted in Iran are unnecessary and optional (elective cesarean), which may be due to lake of knowledge, negative attitude toward normal delivery, fetal health, prevention of urogenital lacerations, fear of pain, change in sexual relationships, persistence of spouse, insurance for expenses, and others’ experiences.[4,5,6,7]
Nowadays, in most of the developed countries, it has been tried to reduce CS and its complications by interventions such as physicians’ education and change in their attitude.[8] In Iran, some strategies have been made to reduce CS. For instance, Tavasoli et al. reported a reduction in rate of CS by 15% through mothers’ education and their psychological and mental preparation to have a natural delivery.[9] But despite these interventions, the rate of CS is growing in developing societies.[4]
One of the important factors that play an unnecessary role in increase of CS is fear of childbirth.[5] There are notable evidences on the primary role of fear of childbirth in the demand for CS, as well as the effect of fear on negative experiences of delivery and emergency CS.[10,11] About 36% of Swedish women claimed fear of pain to be the main reason for selecting CS.[12] Prevalence of fear of childbirth has been reported to be 59% in Iran.[11] The main challenge of a pregnant woman that results in their hesitation is taking decision on the mode of delivery.[13] A person whose decision-making is a part of his/her existence experiences fear as a major problem in life. Humans naturally fear of what is going to happen the next day or what he/she can achieve. A mind with fear always wonders and stays in conflict. Can such a mind make efficient decisions?[14]
Fear, anxiety, and pain are three factors that play a key role at the time of delivery. If fear and anxiety are removed, physical and mental peace replaces them.[15] Some reports in Sweden and Finland showed that half of the women experiencing the fear of childbirth cancelled their request for CS and had a successful vaginal delivery after attaining the ability to express their anxiety and fear and having an interview with a trained person.[16]
One of the most effective ways to cope with fear is non-medicational methods including education and giving proper information to the pregnant women. Research showed that an increase in knowledge and information influences individuals’ ability to recognize key points and enhances their understanding and perception.[17,18] Meanwhile, shortage of knowledge causes fear and anxiety which negatively affect decision-making.[19] Melender reported an association between absenteeism of primiparous women in delivery preparation classes and pregnancy anxiety, fear of childbirth, and consequently, a request for CS.[20] Recently, selection of the most efficient educational method with emphasis on learners’ skills, abilities, and active participation has been reported as one of the main and basic principles in health care.[21,22] One of these methods is use of stories and scenarios which are adopted in role play education. Role play is one of the new educational methods that tries to help individuals find their meaning in the social world and get help from a social group to make a decision on the solution of a dilemma.[22] In this method, a more efficient and better learning occurs due to high concentration and emotional relationship.[23] Also, the learners discover human-related issues by facing problematic situations and discussing about these situations.[24]
Nowadays, role play has found numerous applications such as acting as a tool for emotional drain and expression of fears and feelings, and a method for attitude change or formation of insight in referrals and a method for education of new behaviors.[25] Therefore, with regard to high prevalence of CS in Iran and the effect of fear of childbirth on selection of this method, as well as the restricted research in this field and the mode of research (descriptive research), this study aimed to investigate the effect of role play education on primiparous women's fear of natural delivery and their decision on the mode of delivery.
MATERIALS AND METHODS
This blind clinical trial was conducted on 67 primiparous women (35 in role play group and 32 in lecture education group) referring to the health care centers in three cities of Mashhad province after obtaining the approval of ethics committee of Mashhad University of Medical Sciences.
As no report has been published in relation to the effect of role play on the fear of childbirth, based on a pilot study, the sample size was calculated to be 32 in each group. Sampling was by cluster sampling conducted among the health care centers of region number three. Two centers were assigned to role play method, two to lecture, and from the remaining centers, three subcenters were assigned to role play and three to lecture method. To prevent bias in education, it was tried to conduct education in identical conditions concerning the place of education, level of noise, educational equipments, time of the day, etc. As the routine educational method in health care centers is lecture, there was no need for a control group. Inclusion criteria were: No experience of acute psychological emotions, delivery and childbirth fear score >28, primiparous, single pregnancy, gestational age of 34–36 weeks, age of 18–35 years, no history of infertility, no indication for CS, and not having passed educational course for delivery methods. Exclusion criteria were: Some medical condition in pregnant woman, diagnosis of abnormal fetus/no possibility for delivery of fetus on sonography, and abnormal volume of amniotic fluid or placenta.
To investigate pregnant women's decision, a researcher-made checklist containing one question and to investigate the fear of childbirth, Harman Childbirth Attitude Questionnaire (CAQ) which was revised by Lowe were adopted.[13] This questionnaire was translated to Persian by Khorsandi et al. using Brislin principles. Firstly, two English language experts separately translated the questionnaire into Persian and two others back-translated that into English. After finalization, the version obtained by the bilingual translator was compared with the original version of the questionnaire. The questionnaire has 14 items rated on a four-point Likert's scale (never, seldom, sometimes, and often). Each item is scored 1–4 with total points of 14–56. The higher point shows more fear. As there was no cut-off point for the fear of childbirth, similar international studies were reviewed to determine the cut-off point and a median score of ≤28 was considered for fear of childbirth.[26] For checking the validity of CAQ questionnaire, content validity, and reliability, Cronbach's alpha and internal consistency of the questionnaire were used (a = 0.84). Validity of the decision-making checklist before intervention, 2 weeks after intervention, and of decision-making on the mode of delivery at admission in the labor were confirmed through content validity and their reliability was obtained by evaluators’ consensus (r = 0.974).
The two groups of lecture and role playing were divided into four subgroups after taking pre-test. The role playing group was divided into two subgroups of 10 subjects each and another two subgroups of 9 subjects each (38 subjects). Each group was instructed in a 90-min session about the advantages and disadvantages of normal delivery and CS. In this method, the researcher with two other co-researchers played three scenarios in seven steps (for each scenario) including warm up, selecting the participant, preparing the scene, preparing observers, play, discussion and evaluation, and generalization to education about the advantages and disadvantages of normal delivery and CS.
In the warm-up stage, the researcher narrated two true stories about the individuals who were wondering about the selection of the mode of delivery due to fear of childbirth and asked the participants to voluntarily accept to play the role of pregnant woman with the researcher and two co-researchers. Then the participants helped the researcher to prepare and process the scene (scene preparation was conducted with the needed equipments for role play in two scenarios), and the observers were asked to pay close attention to the scenarios, taking important notes, and discuss them at the end of scenario. In scenarios, the reasons for mothers’ fear of natural delivery and CS were discussed. In the first scenario, one of the participants (a pregnant woman) played the role of a woman who referred to a midwife's office to select the mode of delivery and witnessed the events occurring in the office. Then, she referred to the midwife and consulted with her about her concerns.
The midwife talked to her about the two types of delivery impractically and asked her to express her decision after the scenario about choosing the type of delivery. After choosing the type of delivery, participants discussed the pregnant woman's selection (same researcher gave no help) and justified each other to come to a conclusion. The second scenario was about a woman with a normal delivery and the benefits and complications experienced by her. The next step was similar to the first scenario. In the third scenario, one of the co-researchers defended CS and another defended normal delivery at judge (natural delivery and CS appeared like a human and judge is researcher). After these three scenarios, participants were asked to talk about their friends’/relatives’ experiences of the two types of delivery. Lecture group (two subgroups of 10 subjects each and two subgroups of 9 subjects each) was instructed using PowerPoint presentation, marker, and whiteboard in a 90-min session. At the end of the session, participants’ questions were answered.
Two weeks after administration of educational session in each group (lecture and role play), the CAQ was filled by the pregnant women to measure their fear, and further follow-ups concerning women's decision on delivery mode continued at the time of admission and in the maternity unit. Finally, the researcher recorded the favorite mode of delivery of participants through phone calls.
Data were analyzed by SPSS, and paired t-test, independent t-test, and chi-square were used for analysis.
RESULTS
Participants were aged 24 ± 4 years, of whom 58% were housewives and 14.9% were employees. Educational level of most of the participants (51.4%) was up to high school. Majority of their husbands had an educational level up to junior high school (38.8%) and they were workers (44.3%). Two groups showed no significant differences in terms of age, educational level of pregnant woman and her husband, income, job of pregnant woman and her husband, income, source of information about the type of delivery, insurance, time of referring for pregnancy care, and suggestion of mother, husband, friends, relatives, and gynecologist about the type of delivery (P < 0.05).
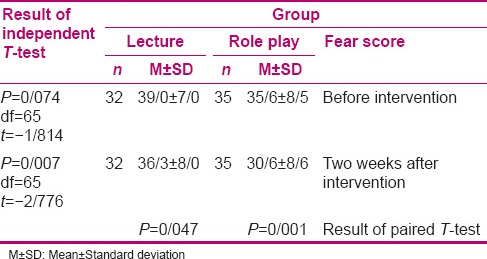
Table 1 shows a significant reduction in the mean score of fear about the mode of delivery after intervention in both groups of role play and lecture, compared to before intervention (P = 0.001 in role play group and P = 0.047 in lecture group). The obtained results also showed a significant difference in the mean score of fear after intervention in both groups of role play and lecture (P = 0.007). This difference was not significant before intervention (P = 0.074) [Table 1].
Table 1.
Comparison of primiparous women's mean scores of fear before and two weeks after intervention in two groups of lecture and role play
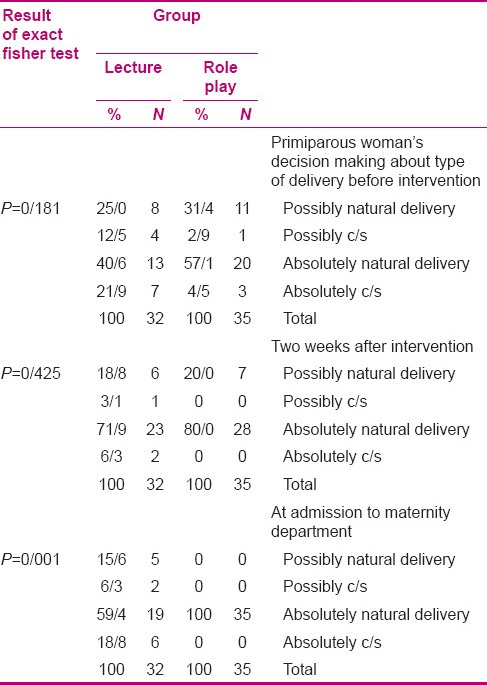
Fischer's exact test was used for comparing the frequency of primiparous woman's decision-making about the type of delivery before, 2 weeks after intervention, and at admission to maternity department. As to the results, no significant difference was found; however, it was significant at admission (P = 0.001) [Table 2].
Table 2.
Comparing frequency of primiparous woman's decision making about type of delivery before, two weeks after intervention and at admission to maternity department
Chi-square test showed no significant difference in the frequency of mode of delivery (pregnant women's function) in the two groups (P = 0.117) [Table 3].
Table 3.
Comparison of frequencies of primiparous women's mode of delivery in two groups of role play and lecture

DISCUSSION
The obtained results showed that education through role play is effective on reduction of fear of childbirth and increase of natural delivery. Although there was no significant difference in the mode of delivery in the present study (P = 0.117), the rate of elective CS in the lecture group was fivefold more compared to that in the role play group. The goal of antepartum education is to reduce mother's request for elective CS, which was achieved in the present study.
As no study was found on the effect of role play on pregnant women's decision-making and fear, the results will be compared with the effects of other educational methods on fear and selecting the type of delivery.
In the present study, the mean score of fear was higher in the lecture group after intervention, compared to the role play group. Ryding states that the fear of delivery in third trimester can be associated with the occurrence of emergency CS.[12] Johnson and Stlid showed no difference in the fear of delivery between women with natural delivery and those with elective or emergency CS,[27] revealing the effect of fear of childbirth in various cultures. Saisto et al., in a study on the effect of group therapy in reducing the fear of childbirth, reported that 85% of women cancelled their request for CS after intervention.[16] Mehdizadeh et al., in a study on the effect of delivery preparation classes on reduction of CS, obtained similar results.[28] Meanwhile, Fahami, in a study on the effect of Lazmar exercises on the outcome of primiparous women's pregnancy, found no significant difference in the rate of CS between the two educational groups of Lazmar technique and control.[15] A person whose decision-making is a part of his/her existence experiences fear as a major problem in his/her life. A fear-captivated mind is always wondering and in conflict,[14] and is the main concern of pregnant women which brings about hesitation in decision-making on their mode of delivery. Being bombarded with negative information and losing power, they experience high fear, which reduces their ability of correct decision-making.[13] Therefore, decisions can be more confidently made if fear is decreased.
Khorsandi et al., in a study on the effect relaxation on reduction of CS, showed that relaxation is effective on reducing the fear of childbirth and increasing natural delivery.[26] In Khorsandi's study, the mean scores of childbirth fear in relaxation and control (receiving conventional care) groups were 40.71 (6.23) and 39.35 (6.96), respectively, before intervention and 38.03 (9.27) and 29.82 (7.18), respectively, after intervention. The difference between the present study and that of Khorsandi et al. was that in their study, each group separately received educational program (including nine 90-min sessions) from the second trimester and used actual play, role play, lecture, and educational CD for education on relaxation, but the control group received only routine care. Meanwhile, in the present study, role play method was conducted just in one group to reduce pregnant women's fear of childbirth and the education included one 90-min session. Then, the obtained results were compared with those of lecture method of education. In the present study, the difference in fear score was significant in the two groups of role play and lecture, and the score of pregnant women's fear was reduced leading to a reduction in an elective CS request at admission in the maternity unit and, consequently, a lower number of elective CSs. Therefore, the present study managed to obtain acceptable results with less time consumed in educating mothers and lower educational costs, compared to the study of Khorsandi. Nowadays, role play has applications such as emotional drain, expression of fears and feelings, attitude change, making an insight in referrals, and education of new behaviors.[25] In the present study, role play could drive pregnant women to select the best mode of delivery by giving them a way to empty their emotions and reduce their fear.
In the lecture group, 25% of women probably and 40.6% absolutely selected natural delivery before intervention. Two weeks after intervention, the possibility of a decision on natural delivery was reduced by 6.2% and its absoluteness increased by 31.3%. But at the time of admission in the labor ward, this possibility decreased by 3.2%, the absoluteness of natural delivery decreased by 12.5%, and the decision on CS increased, compared to before intervention. On the contrary, in role play group, 31.4% and 57.1% of women before intervention would possibly and absolutely select natural delivery, respectively. two weeks after intervention, 11.4% decrease of probable decision and 22.9% increase to absolute decision were observed. At the time of admission in the labor ward, all possibilities for a natural delivery changed to absoluteness. Therefore, role play could change pregnant women's hesitation to decisiveness.
In Fathian's study, behavioral intent model (based on this theory, people firstly make decision and behave based on rational and logical review of available information, and secondly, people consider the outcomes and results of their function before making a decision) was found to be effective in changing pregnant women's attitude toward normal delivery, in comparison with routine pregnancy care (P = 0.007). In Fathian's study, 74.3% of pregnant women of the experimental group (25.7% absolute and 48.6% probable) and 71.4% of the control group (30.0% absolute and 41.4% probable) intended to undergo normal delivery before intervention. After intervention, normal delivery intention was 92.9% in the experimental group and 49.8% in the control group. So, intention to normal delivery has increased by 18.6% in the experimental group and has decreased by 21.6% in the control group.[29] This could be indicated as insufficient routine pregnancy care which has decreased by approaching to delivery time.
The difference between the present study and Fathian's study is that in our study, pregnant women's decision-making was studied in three sections (before intervention, 2 weeks after intervention, and at admission) while Fathian studied it before and after intervention. At admission, many factors could affect the decision on the type of delivery. In this study, although increase in decision-making for normal delivery after intervention in role play in comparison with behavioral intent model was 11.5–18.6%, this increase led to 100% final decision for normal delivery, which remained 100% up to admission in the maternity department, while Fathian did not compare the effect of behavioral intent model after intervention and at admission.
In Fathian's study, the type of delivery performed in the two groups was not significant (P = 0.002); however, the elective CSs in the presence and absence of midwifery problems were not studied. In the present study, although no significant difference was found in the type of performed delivery (P = 0.17), the elective cesarean section in the lecture group was 5 times as much as in the role play group. The aim of education during pregnancy period was to bring about a decrease in elective cesarean by mothers, which was achieved in this study.
Lashgari et al. conducted a study entitled “Effect of training programs of pregnant women on their delivery type selection: A single blind, randomized control trial.” The test group used different structural methods such as film, booklet/lecture notes, visiting the maternity department and interviewing the women who had delivery. Results showed significant different between the test and control (no education) groups in term of the type of delivery selected (P = 0.03).[30] Education could increase the decision taken toward normal delivery to 14%; however, in the present study, role playing could increase the decision for normal delivery to 100%, which remained unchanged up to time of delivery. In fact, the role play method could increase the decision for normal delivery in a short time (90 min) in comparison with the study of Lashgari (180 min) and sustain the decision made. In Lashgari's study, pregnant women's decision at admission to the maternity department was not studied, so there was no data to be compared in this part.
In Rahimi Kian et al.'s study entitled “The effect of education based on Health Belief Model on selecting type of delivery,” the test group used different structural methods such as lecture, question and answer, film presentation of normal delivery and CS, and pamphlets about normal delivery and CS. The results showed a significant difference between the two groups in terms of the type of delivery selected (P = 0.001) (control group received routine pregnancy care). Health Belief Model led to 96.9% selecting normal delivery and 3.1% selecting cesarean.[31] As Rahimi Kian did not report the rate of normal delivery and CS before intervention, there was no data to compare with the present study.
Although the educational intervention of Rahimi Kian, Fathian, and Lashgari could increase the rate of normal delivery, none of them studied the sustainability of this decision at the beginning of labor that is the main situation for decision-making, and finally, the type of performed delivery. Of the strengths of the present study is 100% decision-making for normal delivery, sustained decision up to admission to the maternity department, and decrease in elective cesarean in the role play group in comparison with the lecture group.
In role play education, it is tried to help people find their internal meaning in the social world and get help from it to make a decision while facing a dilemma.[22] The methods, which need active involvement, including role play, increase the individuals’ association to the message and lead to individuals’ emotional drain.[32] Therefore, this issue can be one of the reasons for an increase in pregnant women's decision to undergo natural delivery and reduction of elective CS in role play method, compared to lecture method.
It is suggested to conduct further studies on the effect of role play education on pregnant women's fear of childbirth and selection of mode of delivery, and compare it with other educational methods in order to use the most efficient educational method to reduce elective CS.
CONCLUSION
Our results emphasize on the effect of role play education in reducing the fear of childbirth and unnecessary CS. Application of active educational methods such as role play, accompanied with lecture method, is suggested to reduce primiparous women's fear of childbirth and, consequently, reduce unnecessary CS.
ACKNOWLEDGMENTS
Special thanks to participants, co-researchers (Ms Golzar, Ms Karami, and Ms Mirzaee), and respected staff of Masshad Health Center No. 3. Authors thank MUMS Vice-presidency for research for providing full financial support for this study. This study is an MSc thesis.
Footnotes
Source of Support: This work has been funded by Vice-Chancellor for Research, Mashhad University of Medical Sciences, Mashhad, Iran with code of 88822
Conflict of Interest: Nil.
REFERENCES
- 1.Cunningham F, Leveno K, Gilstrap L, Hauth J, Wenstrom K. 22nd ed. New York, NY: The McGraw-Hill Professional Publishing; 2005. Williams obstetrics; p. 590. [Google Scholar]
- 2.Quadros L. Caesarean section controversy. Brazilian obstetricians are pressured to perform caesarean sections. BMJ. 2000;320:1073. [PubMed] [Google Scholar]
- 3.Sharifirad G, Fathian Z. Survey of pregnant women view than vaginal and cesarean delivery based on behavioral intention model. J Illam Univ Med Sci. 2007;1:19–23. [Google Scholar]
- 4.Nuri T. Midwifery, MSc Thesis. Iran: Tehran University of Medical Sciences; 2004. Reasons of cesarean choice in pregnant women refer to Rasht health centers. [Google Scholar]
- 5.Salmani N. Assessment of the pregnant women view's in relation to affecting causes in select of delivery method in shohada kargar hospital of Yazd. J Orumiye Nurs Midwifery Fac. 2007;5:156–61. [Google Scholar]
- 6.Mohammaditabar S, Kiani A, Haidari M. Assessmen of nulliparous women tendencies to choose the type of delivery. J Babol Univ Med Sci. 2009;3:54–9. [Google Scholar]
- 7.Negahban T, Ansari A. whether the fear of delivery can be predict the emergency caesarean among the primigravida women? J Nurs Midwifery Tehran Med Sci. 2008;14:73–81. [Google Scholar]
- 8.Gunnervik C, Josefsson A, Sydsjo A, Sydsjo G. Attitudes mode of birth among Swedish. Midwifery. 2010;26:38–44. doi: 10.1016/j.midw.2008.04.006. [DOI] [PubMed] [Google Scholar]
- 9.Tavasoli M. Health Education MSc Thesis. Iran: University Tarbiat Modarres; 2001. The effects of education on elective cesarean reduce in pregnant women. [Google Scholar]
- 10.Eriksson C, Westman G, Hamberg K. Content of childbirth related fear in Swedish women and men-Analysis of an open ended question. J Midwifery Women's Health. 2006;51:112–8. doi: 10.1016/j.jmwh.2005.08.010. [DOI] [PubMed] [Google Scholar]
- 11.Zafarghandi N, Hadavand SH, Torkestani F, Zaeri F, Variji M. Evaluation of anxiety and fear of labor in postpartum period. J Med Counc Islamic Republic Iran. 2005;2:155–160. [Google Scholar]
- 12.Ryding EL, Wijma B, Wijma K, Rtdhstorm H. Fear of childbirth during pregnancy may increasing the risk of emergency caesarean section. Acta Obstet Gynecol Scand. 1998;77:542–7. [PubMed] [Google Scholar]
- 13.Lowe NK. Self efficacy for labour and childbirth fears in nulliparous pregnant women. J Psychosom Obstet Gynecol. 2000;21:219–24. doi: 10.3109/01674820009085591. [DOI] [PubMed] [Google Scholar]
- 14.Murita AQ. Rise of Japan. In: Rajab Zadeh H., translator. Tehran: Soroush Publications; 1995. pp. 312–3. [Google Scholar]
- 15.Fahami F, Masoufar S, Davazdahemami SH. The effect of Lamaze practices on the outcome of pregnancy and labour in primipara women. Iranian J Nurs Midwifery Res. 2007;12:111–4. [Google Scholar]
- 16.Saisto T, Salmela-Aro K, Kononen T, Nurmi JE, Halmesmaki E. A controlled trial of intervention in fear of childbirth. Obstet Gynecol. 2001;98:820–6. doi: 10.1016/s0029-7844(01)01552-6. [DOI] [PubMed] [Google Scholar]
- 17.Lewis J, Leach J. Discussion of socio-scientific issues: The role of science knowledge. Int J Sci Educ. 2006;28:1267–87. [Google Scholar]
- 18.Prokop P, Lešková A, Kubiatko M, Diran C. Slovakian students’ knowledge of and attitudes toward biotechnology. Int J Sci Educ. 2007;29:895–907. [Google Scholar]
- 19.Rodríguez Yunta E, Valdebenito Herrera C, Misseroni A, Fernández Milla L. Attitudes towards genomic research in four Latin American countries. [Last accessed on 2008 Sep24];Electron J Biotechnol. 2005 8:238–48. Available from: http://www.ejbiotechnology.info/content/vol8/issue3/full/9/bip/ [Google Scholar]
- 20.Melender R. Experiences of fears associated with pregnancy and childbirth: A study of 329 pregnant women. Birth. 2002;29:101–11. doi: 10.1046/j.1523-536x.2002.00170.x. [DOI] [PubMed] [Google Scholar]
- 21.Saghravanian M. Mashhad: Nursing and Midwifery Faculty, University of Medical Science; 2003. The effect of programmed instruction and lecture on students cognetive domain. [Google Scholar]
- 22.Joyce BR, Weil M, Calhoun E. Models of the aching. In: Behrangi MR, translator. 7th ed. Tehran: Kamale Tarbiat Publications; 2004. [Google Scholar]
- 23.Saberian M, Hajiaghajani S. Tehran: Salemi Publications; 2006. The process of curriculum planning in medical science; pp. 43–54. [Google Scholar]
- 24.Cacioppo J, Petty R, Kao C, Rodriguez R. Central and peripheral routes to persuasion: An individual difference perspective. J Pers Soc Psychol. 1986;51:1032–43. [Google Scholar]
- 25.Goldfried NR. New York: Holt, Reinhart, and Winston; 1976. Division; G.c. Clinical behavior Therapy. [Google Scholar]
- 26.Khorsandi M, Ghofranipour F, Hidarnia A, Faghihzadeh S, Vafaei M, Rousta F, et al. The effect of childbirth preparation classes on childbirth fear and normal delivery among primiparous women. Arak Univ Med Sci J. 2008;11:29–36. [Google Scholar]
- 27.Johnson R, Slade P. Does fear of childbirth during pregnancy predict emergency caesarean section? BJOG. 2002;109:1213–21. doi: 10.1046/j.1471-0528.2002.01351.x. [DOI] [PubMed] [Google Scholar]
- 28.Mehdizadeh A, Roosta F, Kamali Z, Khoshgoo N. Evaluation of the effectiveness of antenatal preparation for childbirth courses on the health of the mother and the newborn. J Iran Univ Med Sci. 2003;35:455–62. [Google Scholar]
- 29.Fathian Z, Sharifi Rad G, Hasanzade A, Fathian Z. Study of the effects of Behavioral Intention Model education on reducing the cesarean rate among pregnant women of Khomeiny-Shahr. J East Medico. 2006;9:123–31. [Google Scholar]
- 30.Lashgari M, Delavari S, Markazi Moghaddam N, Gorouhi F. Effect of training programs of pregnant women on their delivery type selection: A single blind, randomized control trial. J Tehran Army Univ Med Sci. 2005;3:679–84. [Google Scholar]
- 31.Rahimi Kian F, Miralimohamadi M, Abbas M, Abuzar Gazaforudi K, Salmani Barugh N. Effect of Health Belief Modell education on chosen delivery method. J Nurs Midwifery. 2008;14:25–32. [Google Scholar]
- 32.Abedian Z, Navaee M, Jafarisani H, Ebrahimzadeh S. Comparison of the effect of two teaching methods of role playing and lecture on primigravida women's knowledge, attitude and decision making in relation to type of delivery. J Obstet Gynecol Infertil. 2012;14:25–35. [Google Scholar]