

Abstract
Background:
Hypotension and muscular cramp are the common complications of hemodialysis. Effective control of hemodialysis complications increases the survival time and the quality of life of patients on hemodialysis. Considering that failure to follow a therapeutic plan is one of the most prevalent causes of hemodialysis complications, the present research was conducted to study the effect of two educational methods (family-centered and patient-centered) on some complications that occur during hemodialysis.
Materials and Methods:
This clinical trial was performed from June to November 2012 in the hemodialysis ward of Imam Khomeini Hospital and Tehran Amir Aalam Hospital. Research samples included 60 patients in the age range of 18-65 years who were randomly included in patient-centered education (30 people in even days) and family-centered education (30 people in odd days). Blood pressure and muscle cramp were checked using researcher-made checklist in three stages (before and at the second and fourth week after intervention). Hypotension (before the start of dialysis, at the first, second, and third hour, and at the end hours) and muscle cramp (in the middle of hemodialysis and the end half an hour) were also checked. Data were analyzed using SPSS software, version 16, with Chi-square test, Fisher test, and independent t-test.
Results:
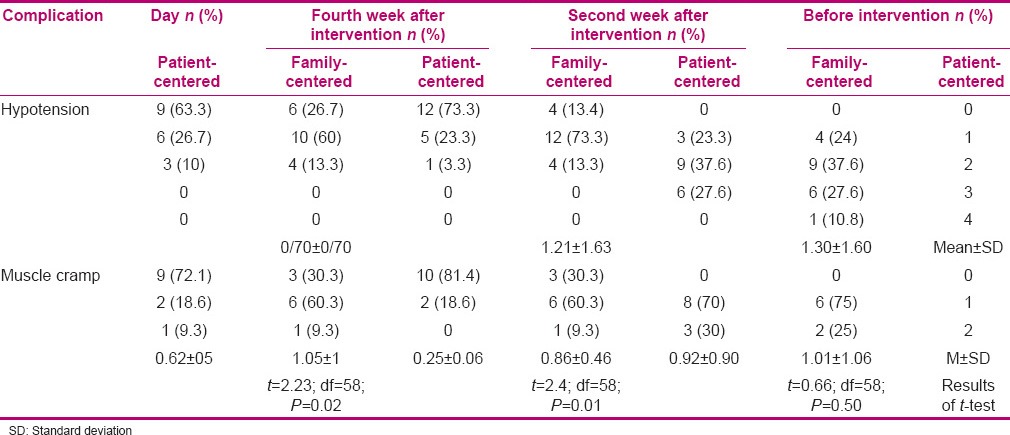
Before intervention, the two groups did not show significant difference in terms of hypotension [with P = 0.91 and variations mean of 1.60 (1.30)] and muscle cramp [with P = 0.50 and variations mean of 1.06 (1.01)]. In the second and fourth week after intervention, there was significant difference between the two groups in terms of hypotension [with P = 0.016 and variations mean of 0.70 (0.70) and P = 0.02 and variations mean of 0.86 (0.62)] and muscle cramp [with P = 0.01 and variations mean of 0.46 (0.86) and P = 0.02 and variations mean of 1 (1.05)].
Conclusions:
Considering that the study results showed that family-centered education was more effective on reduction of hemodialysis complications than patient-centered education, it is recommended that educational interventions relating to therapeutic program should be done in patients under hemodialysis, with participation of families.
Keywords: Family-centered nursing, hemodialysis, hypotension, Iran, muscular cramp, patient-centered care
INTRODUCTION
With the progress being made in different therapeutic methods and sciences, lifespan of patients with chronic diseases has increased and on the other hand, needs of the chronic patients have increased.[1] One of the diseases causing considerable stress for the patients is end-stage renal disease (ESRD). General incidence of ESRD is 260 cases in million persons per year and increases by 6% every year.[2,3] The most common therapeutic method for these patients is hemodialysis.[4] Although hemodialysis improves the health and increases the survival of patients,[5] it has some complications such as hypotension and muscle cramp.[6] Hypotension is the most common complication during hemodialysis, which occurs in about 20-50% of the patients.[7] This complication not only causes fatigue and lethargy during dialysis,[8] insufficient removal of additional fluids from the body,[9] and emergence and progress of cardiovascular complications,[4] but also increases the need for nursing care for repeated control of hypotension, prescription of liquids and drugs, oxygen therapy, positioning, and reduction of ultrafiltration.[10] Despite recent progresses being made in hemodialysis, muscle cramp is regarded as a big problem in these patients.[11] It is estimated that 33-86% of the patients under hemodialysis experience muscle cramp. This complication increases the creatine phosphokinase level, shortens effective dialysis time,[12] and finally increases the mortality rate in patients;[11] in addition, it is painful and limits the movement of patients.[13]
Studies have shown that hemodialysis complications are majorly due to failure to follow the therapeutic program. Therefore, educating patients with chronic kidney disease is necessary.[14] It is very difficult for many of these patients to follow the therapeutic plan involving diet, liquids, and drug,[15] and studies have shown that 33-50% of the patients under hemodialysis do not observe a liquid diet and the recommended food restrictions.[16] On the other hand, as the recommended diet is usually observed in the house environment, its obedience may be affected by the family.[1] The positive effects of education are as one of the important aspects of nursing activity[17] and the presence of families beside patients increases the sense of participation, respect, and cooperation,[18,19] increases hope and trust,[20] promotes health and welfare of the family,[21] reduces economic expenses,[3] and increases the obedience of patients to the therapeutic program.[22] The effect of educating the family beside patients on reduction of hemodialysis complications has not been studied up to now. Therefore, this study was conducted to compare the effects of two educational methods (family-centered and patient-centered) on reduction of two complications prevalent during dialysis (hypotension and muscular cramp) among the patients undergoing hemodialysis. Considering that there is close relationship between patient and family in our country, the results of this research show that educating the active family members beside the patients on hemodialysis can be effective in reducing hemodialysis complications. Educating patients’ families can be recommended to the educational authorities of hemodialysis sectors as a positive achievement.
MATERIALS AND METHODS
This study is a clinical trial of quasi-experimental type with registration in IRCT No. IRCT201204161599N17 and was conducted between June and November 2012 in patients under hemodialysis treatment referring to Imam Khomeini Hospital and Amir Aalam Hospital affiliated with Tehran University of Medical Sciences. To prevent disclosure of information, patients were divided into even and odd groups by random assignment. Due to access to enough sample size, two hospitals were selected, which were homogenous in terms of personnel, hemodialysis, and the referring patients. To prevent publication of information, patients were randomly divided into even and odd groups by drawing lots. In this study, 30 patients were included in patient-centered group (even days) and 30 patients in family-centered group (odd days). To determine the necessary sample size at a significance level of 0.05 and statistical power of 80% and given that diet obedience rate in the two groups had at least a difference of 25% to be regarded statistically significant, the sample size was estimated to be 30 persons in each group after considering sample loss. Inclusion criteria of this study were age 18-65 years, undergoing hemodialysis thrice a week and 3-4 h at any time, afflicted by hypotension complications or muscle cramp during 2 weeks before intervention, not affected by cardiovascular diseases and musculoskeletal diseases, and not taking antihypertensive and anti-cramp drugs., Inclusion criteria of the family were: The main person who had the highest participation in treatment and spent the longest time with the patient (according to the patient) and had at least a minimum level of education (reading and writing).
In case patients were candidates of kidney transplantation during the study or their pharmaceutical and dietary plans were changed by the physician, they were excluded from the study. Personal information of the patients included demographic information and information relating to disease. Observational checklist was used for recording blood pressure and muscular cramp. To determine the scientific validity of the researcher-made questionnaires, content validity method was used. In this regard, data collection instrument was prepared after review of books, new and relevant scientific papers, similar research, internet sites, and views of supervisors and advisors and then given to 10 members of the faculty board of Tehran University of Medical Sciences for content validity. After collecting their views, corrective views and suggestions of the professors were applied with the guidance of supervisor and advisor. Reliability of the questionnaire was estimated at 0.75 with Cronbach's coefficient alpha and reliability of the observational checklist was confirmed with concurrent observation and coefficient of concordance of 1. Personal information of the patients consisted of two parts: Demographic information and information relating to disease. During two consecutive weeks, blood pressure of patients was studied and recorded at five time intervals (immediately before dialysis, and at the first hour, second hour, third hour, and end hour of dialysis) and muscle cramp was also studied and recorded at two time intervals (in the middle and end half an hour of dialysis). Education was performed in two groups (patient-centered and family-centered) as face-to-face education on the bed of patients, considering the educational needs of patients in diet, physical exercise plan, and pharmaceutical program.
The research method was such that the study was conducted after performing administrative stages and receiving license from the ethical committee of the university, after introducing him/her and mentioning the goals of the research to the research units (eligible based on inclusion criteria), and attracting their attention and receiving their informed consent. Before the start of the intervention, blood pressure was recorded for two consecutive weeks, 3 days a week for 5 times a day (before dialysis, and at 1 h, 2 h, 3 h, and end hour of dialysis) using blood pressure observational checklist and the patient was included in the study with the first incidence of hypotension in each one of the stages. In this study, hypotension during dialysis was defined as systolic pressure of the patients reduced by more than 30% compared with the period before dialysis or below 100 mmHg, or diastolic pressure below 60 mmHg.[6,23] Muscle cramp was recorded with a two-point scale, i.e. yes or no, 2 weeks before dialysis, thrice a week and twice a day (in the middle and end half an hour of dialysis) and the patient was included in the study with the first incidence of muscle cramp. The above complications were studied personally by the researcher. At the end of the second week, the intervention started. In this way, education was performed in two groups (patient-centered and family-centered) in a face-to-face manner with the patients. In the patient-centered group, educational content was presented to the patients themselves and in the family-centered group, one member of the family attended the educational sessions, in addition to the patient. The number of educational sessions was four, with each taking 30-45 min. In the first session, kidney disease, the reason for affliction with kidney disease, the mechanism of hemodialysis device, the number of hemodialysis sessions, etc., were explained. In the second session, explanation on nutrition (correct diet, importance of diet observance, permissible amount of food, food restriction, etc.) was given. In the third session, motor program (importance of regular physical exercise and its rate) and pharmaceutical program (administration of drugs, their side effects, the reason for prescription considering orders of the related physician) were explained. At the end of the sessions, pamphlet relating to each session was given to the participants. A phone number was given to the participants to contact if necessary and get their questions answered. After performing the intervention, blood pressure and muscle cramp were studied in the second week and fourth week after intervention in both groups. In this way, blood pressure of the patients was studied for 1 week, 3 days a week and 5 times a day (immediately before dialysis, at the first hour, second hour, and third hour, and after dialysis) and muscle cramp was also studied for 1 week, 3 days a week and twice a day (in the middle and end half an hour of dialysis when most cramps occur). Data were analyzed using SPSS software, version 16, with Chi-square test, Fisher test, and independent t-test.
RESULTS
Thirty persons were included in each group in the study and none of them were excluded. Mean age of the patients was 47.41 (10.31) years in the patient-centered group and 48.16 (9.21) years in the family-centered group. Other demographic data are presented in Table 1. It is necessary to note that both groups were homogenous in terms of demographic variables, except for the marital status and lifestyle which did not have relationship with obedience and were not regarded as intervening variables based on independent t-test (relationship between marital status and diet: P = 0.49, pharmaceutical: P = 0.11, motor: P = 0.49; relationship between lifestyle and diet: P = 0.31, pharmaceutical: P = 0.25, motor: P = 0.16). The most common cause in the patient-centered group (43.3%) and family-centered group was diabetes and most of the patients in the patient-centered group (46.7%) and family-centered group (43.3%) had been dialyzed for 1-5 years. Frequencies of hypotension and muscle cramp are shown in Table 2.
Table 1.
Demographic data of the patients under hemodialysis in the two groups
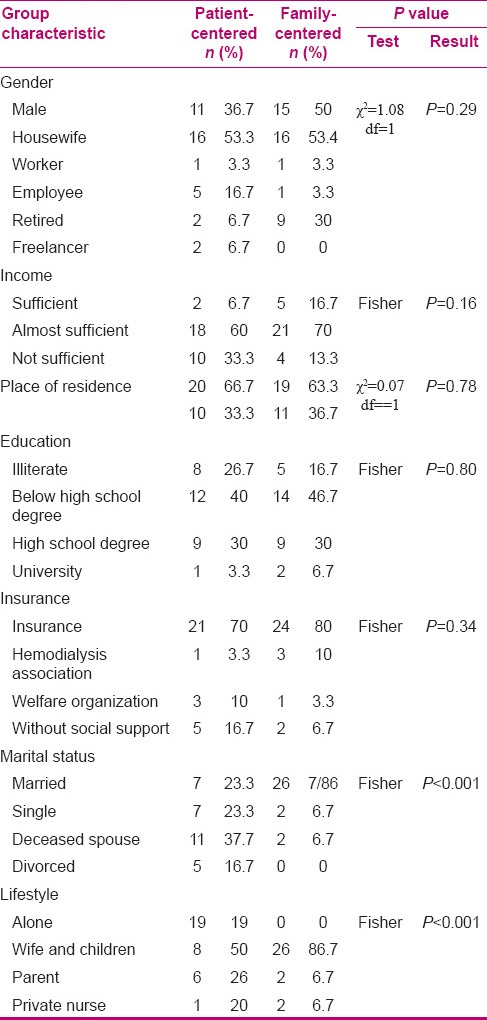
Table 2.
Comparison the effects of education on the frequencies of hypotension and muscle cramp in the two groups
DISCUSSION
Of the major problems of treatment with hemodialysis is the complications occurring during dialysis, such as hypotension and muscle cramp, which reduce the efficiency of dialysis and life quality and extensively increase the mortality rate of patients.[24]
Research findings show that the highest frequency of hypotension was 2 in both groups during 2 weeks before intervention and the highest rate of hypotension occurred in the end hour of hemodialysis. Therefore, the two groups did not have significant difference in terms of hypotension frequency and were homogenous. But in the second and fourth weeks after intervention, education of patients and their families significantly reduced the frequencies of hypotension. Thus, 73.3% and 63.3% did not suffer from the above complication in the family-centered group in the second and fourth weeks after intervention, respectively, while 73.3% and 60% of the patients in the patient-centered group had sudden hypotension in the second and fourth weeks after intervention, respectively. Tabrizi et al. also conducted a study on the effect of planned nursing care on the prevention of hemodialysis complications; for studying the complications, the complications checklist was used and they concluded that the planned nursing care during dialysis significantly reduced hypotension from 66.7% to 10% (P < 0.001).[25] In the present study, the complications checklist was used and family-centered education led to observance of therapeutic program at home (particularly fluid intake restrictions) and, consequently, prevention of hypotension during hemodialysis. Salehi Taly et al. conducted a research on the effect of dietary education on laboratory indices and weight gain between two dialysis sessions and concluded that dietary education was effective on the index of phosphor and weight gain between two sessions and there was significant difference between the two groups (P = 0.001).[26] The above study is similar to the present study in terms of face-to-face educational method and dietary educational content; also, in the above research, attempt was made to prevent weight gain between two dialysis sessions based on diet and increase of ultrafiltration and incidence of complications such as hypotension. Wan-na et al. in a study focusing on hypotension during dialysis and its nursing cares, concluded that health education (diet and fluid restriction) to the patients under hemodialysis reduced the percentage of hypotension from 68.5% to 23.6% (P < 0.05).[27] A study which was conducted by Jihong on hypotension prevention and nursing care of the patients under hemodialysis concluded that prevention was the main key to treatment of hypotension during hemodialysis. In this study, dietary education to patients reduced hypotension from 57.6% to 15.7%, which is in line with the present research.[28]
Within 2 weeks of the study before intervention, the highest frequency of muscle cramp in both groups was 1 and most cramps occurred in the final half an hour of hemodialysis. Therefore, the two groups did not have significant difference in terms of muscle cramp frequency and were homogenous. But in the second and fourth weeks after intervention, family-centered education significantly reduced the frequencies of muscle cramp. So, in the family-centered group, 81.4% and 72.1% did not have the above complication in the second and fourth weeks after intervention, respectively, while in the patient-centered group, 60.3% and 60.3% of the patients had sudden muscle cramp in the second and fourth weeks after intervention, respectively. Hadian et al. conducted a study on the effect of walking on the frequencies and intensity of muscle cramp in patients under hemodialysis and concluded that physical exercise and walking education significantly reduced muscle cramps (10 out of 12 patients did not have muscle cramp in the intervention group) (P = 0.01).[11] In the study by Tabrizi et al. percentage of muscle cramp significantly decreased from 50% to 6.7% with planned nursing care during dialysis (P = 0.001).[25] Yaaghoobi et al. in their study on the effect of isotonic and isometric sports on muscle cramp of the patients under hemodialysis showed that physical exercise prevented and reduced muscle cramp.[29] Heidarzadeh et al. conducted a study on the effect of sport program on physical and mental problems of hemodialysis patients and concluded that 85.6% of the patients with regular physical exercise reported reduction of fatigue and muscular dystrophy and improvement of physical conditions and daily activities.[30] In a systematic review which was performed by Denhaerynck et al. on the incidence and results of failure to follow therapeutic program in patients under hemodialysis, 30-74% of the studied patients had muscle cramps and the reason was attributed to failure to observe therapeutic program based on limited fluids and dietary restriction.[15] In a study by Yun et al. on the effect of family-centered interventions on patients with chronic kidney disease, they concluded that family-centered education significantly reduced hemodialysis complications, in addition to reduction of depression and increase of life satisfaction and self-care, so that it reduced the percentage of hypotension from 76.3% to 23% and muscle cramp from 56.4% to 23.5%.[31] In the study by Yu et al. (2008) on the effect of family-centered intervention on life quality of hemodialysis patients, there was no significant difference found between the albumin level and the life quality of two groups before intervention (P > 0.05), but the patients in family-centered group had higher albumin level and better life quality than those in patient-centered group after intervention (P < 0.05).[32]
In the present study, an inclusion criterion was the incidence of hypotension during dialysis in six hemodialysis sessions (two consecutive weeks), and due to time limitation, the criterion of hypotension was not included in 20% of the dialysis sessions during 1 month. Duration of control and follow-up stages was also short (4 weeks), and more extensive and longer study should be conducted in this regard.
CONCLUSION
Not following the treatment plan due to lack of knowledge and sensitivity of the patients and their families regarding compliance with the treatment plan is one of the major causes of morbidity in patients undergoing hemodialysis. So, providing nursing education with an emphasis on active participation of the patient and family in treatment is recommended. Family members can work together to treat the patient with medical team. Also, it can reduce the economic burden of the family, reduce health care costs, and reduce readmissions of patients.
ACKNOWLEDGMENT
This article is a part of research approved by Tehran University of Medical Sciences, grant number 91-01-99-17037. We thank all the patients and their families and the dialysis nursing staff who took part in the study.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Hickman RL, Jr, Douglas SL. Impact of chronic critical illness on the psychological out comes of family members. AACN Adv Crit Care. 2010;21:80–91. doi: 10.1097/NCI.0b013e3181c930a3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chauveau P, Nguyen H, Combe C, Chêne G, Azar R, Cano N, et al. Dialyzer Membrane Permeability and Survival in Hemodialysis Patients. Am J Kidnay Dis. 2005;45:565–71. doi: 10.1053/j.ajkd.2004.11.014. [DOI] [PubMed] [Google Scholar]
- 3.Low J, Smith G, Burns A. The impact of end-stage kidnay disease (ESKD) on close person: A literature review. NDT Plus. 2008;5:67–79. doi: 10.1093/ndtplus/sfm046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Abbas G, Rafiquee Z, Shafi T. Relationship of postdialysis serum sodium level and interdialytic weight gain in patients on maintenance hemodialysis. J Coll Physicians Surg Pak. 2007;17:482–5. [PubMed] [Google Scholar]
- 5.Baraz S, Mohamadi E. Comparative study on the effect of two methods of self-care education (direct and indirect) on quality of life and physical problems of hemodialysis patients. Arak Med Uni J. 2006;9:1–16. [Google Scholar]
- 6.Zhou YL, Liu HL, Duan XF, Yao Y, Sun Y, Liu Q. Impact of sodium and ultrafiltration profiling on haemodialysisrelated hypotension. Nephrol Dial Transplant. 2006;21:3231–7. doi: 10.1093/ndt/gfl375. [DOI] [PubMed] [Google Scholar]
- 7.Henrich WL. Hemodynamic instability during hemodialysis: Overview. [Last accessed on 2009 Dec 13]. Available from: http://www.uptodate.com/patients/content/topic.do/
- 8.Shahgholian N, Shafiei F, Amini M, Amini P, Abazari P. The viewpoints of patients, families and medical team on internal barriers toblood glucose level management. Iranian Journal of Nursing and Midwifery Research. 2009;14:155–61. [Google Scholar]
- 9.Aliasgharpour M, Shomali M, Zakerimoghaddam M. Effect of a self efficacy promotion traning programe on the body weight changes in patients undergoing hemodialysis. J Ren Care. 2012;38:155–61. doi: 10.1111/j.1755-6686.2012.00305.x. [DOI] [PubMed] [Google Scholar]
- 10.Santoro A, Mancini E, Basile C, Amoroso L, Di Giulio S, Usberti M. Blood volume controlled hemodialysis in hypotension-prone patients: A randomized, multicenter controlled trial. Kidney Int. 2002;62:1034–45. doi: 10.1046/j.1523-1755.2002.00511.x. [DOI] [PubMed] [Google Scholar]
- 11.Haddian Z. The effect of walking on the frequency and intensity of pain caused by muscle cramps in haemodialysis patients: A pilot study. Iranian Journal of Nursing and Midwifery Research. 2012;13:161–9. [Google Scholar]
- 12.Song JH, Park GH, Lee SY, Lee SW, Lee SW, Kim MJ. Effect of sodium balance and the combination of ultrafiltration profile during sodium profiling hemodialysis on the maintenance of the quality of dialysis and sodium and fluid balances. J Am Soc Nephrol. 2005;16:237–46. doi: 10.1681/ASN.2004070581. [DOI] [PubMed] [Google Scholar]
- 13.Bourbonnais FF, Tousignant KF. The pain experiences of patients on maintenance hemodialysis. Nephrol Nurse J. 2012;39:13–9. [PubMed] [Google Scholar]
- 14.Lingerfelt KL, Thornton K. An educational project for patients on hemodialysis to promote self-management behaviors of end stage renal disease. Nephrol Nurse J. 2011;38:483–8. [PubMed] [Google Scholar]
- 15.Denhaerynck K, Manhaeve D, Dobbels F, Garzoni D, Nolti CH. Prevalence and consequence of nonadherence to hemodialysis regimens. Am J Crit Care. 2007;16:222–35. [PubMed] [Google Scholar]
- 16.Kohno Y, Maruyama MY. Relationship of psychological characteristics and self-efficacy in gastrointestinal cancer survivors. Psychooncology. 2010;19:71–6. doi: 10.1002/pon.1531. [DOI] [PubMed] [Google Scholar]
- 17.Hekmatpou D, Anoosheh MF. Pathology of patient education: A qualitative study. Iran J Nurs Spr. 2007;20:51–60. [Google Scholar]
- 18.Celik G, Annagur BB, Yilmaz M, Demir T, Kara F. Re sleep and life quality of family caregivers affected as much as those of hemodialysis patients? Gen Hosp Psychiatry. 2012;34:518–24. doi: 10.1016/j.genhosppsych.2012.01.013. [DOI] [PubMed] [Google Scholar]
- 19.Mitchell M, Chaboyer W, Burmeister E. Foster M.Positive effects of a nursing intervention on family- centered care in adult critical care. Am J Crit Care. 2009;18:543–52. doi: 10.4037/ajcc2009226. [DOI] [PubMed] [Google Scholar]
- 20.Abrahamian FM, Deblieux PM, Emerman CL, Kollef MH, Kupersmith E, Leeper KV. Health care accociated pneumonia: Identification initial management in the EED. Am J Emerg Med. 2008;26:1–11. doi: 10.1016/j.ajem.2008.03.015. [DOI] [PubMed] [Google Scholar]
- 21.Bland R, Darlington Y. The nature and sourse of hope: Perspective of family caregivers of people with serious mental illness. Perspect Psychiatr Care. 2002;38:61–8. doi: 10.1111/j.1744-6163.2002.tb00658.x. [DOI] [PubMed] [Google Scholar]
- 22.Zolfaghari M, Asgari P, Aliasgharpour M, Haghani H. Can addressing Family education improve adherence of therapeutic regime in hemodialysis patients? In Press. [Google Scholar]
- 23.Tang HL, Wong SH, Chu KH, Lee W, Cheuk A, Tang CM, et al. Sodium ramping reduces hypotension and symptoms during haemodialysis. Hong Kong Med J. 2006;12:10–4. [PubMed] [Google Scholar]
- 24.Meira FS, Poli de Figueiredo CE, Figueiredo AE. Influence of sodium profile in preventing complications during hemodialysis. Hemodial Int. 2010;11:29–32. doi: 10.1111/j.1542-4758.2007.00226.x. [DOI] [PubMed] [Google Scholar]
- 25.Tabrizi M, Najafi M, Samiey S, Einollahi B, Babaei GH. Effect of programmed nursing care in prevention of hemodialysis complications. Iran J Crit Care Nurs. 2009;2:55–9. [Google Scholar]
- 26.Salehi Taly SH, Akbarsharifee T, Gholam Araghi M, HH. Effect of teaching aboute diet regimen on laboratory index and weight gain of hemodialysis patient. IJN. 2003;15:92–9. [Google Scholar]
- 27.Wan-Na F, Mwi-zhen X, Yu-fang Z, Xin Y, Y YH. Nursing of hemodialysis related hypotention. Zhonghua Hu Li Za Zhi. 2011;21:23–6. [Google Scholar]
- 28.Jihong H. Prevention and nursing care of hypotention for patient accepting hemodialysis. Chin Gen Nurs. 2009;19:28–34. [Google Scholar]
- 29.Yaaghoobi M, Mohamadi E. Effects of applying isotonic and isometric exercises on muscles cramp in hemodialysis patients. Kordestan Sci Univ Mag. 2008;2:53–60. [Google Scholar]
- 30.Heidarzadeh M, Zamanzadeh V, Pashaee Maghvan A. The effect of physical exercise on physical and psychological problems. Iranian Journal of Nursing and Midwifery Research. 2009;15:15–21. [PMC free article] [PubMed] [Google Scholar]
- 31.Yun M, Wang ML, Yun XC. The effect of family nursing intervention on chronic renal failure patients. Zhonghua Hu Li Za Zhi. 2011;13:19–22. [Google Scholar]
- 32.Yu RL, Liang XL, Fu X. The Influence of Early-stage Family Intervention on Life Quality of HD Patients from Low Function Families. Zhonghua Hu Li Za Zhi. 2008;4:67–79. [Google Scholar]