

Abstract
Background
The irradiation of head and neck cancer (HNC) often causes damage to the salivary glands. The resulting salivary gland hypofunction and xerostomia seriously reduce the patient’s quality of life.
Purpose
To analyze the literature of actual management strategies for radiation-induced hypofunction and xerostomia in HNC patients.
Methods
MEDLINE/PubMed and the Cochrane Library databases were electronically evaluated for articles published from January 1, 1970, to June 30, 2013. Two reviewers independently screened and included papers according to the predefined selection criteria.
Results
Sixty-one articles met the inclusion criteria. The systematic review of the literature suggests that the most suitable methods for managing the clinical and pathophysiological consequences of HNC radiotherapy might be the pharmacological approach, for example, through the use of cholinergic agonists when residual secretory capacity is still present, and the use of salivary substitutes. In addition, a modified diet and the patient’s motivation to enhance oral hygiene can lead to a significant improvement.
Conclusion
Radiation-induced xerostomia could be considered a multifactorial disease. It could depend on the type of cancer treatment and the cumulative radiation dose to the gland tissue. A preventive approach and the correct treatment of the particular radiotherapeutic patient can help to improve the condition of xerostomia.
Keywords: radiation-induced xerostomia, salivary gland hypofunction, management strategies
Introduction
Xerostomia is a term used to describe the subjective symptoms of a dry mouth deriving from a lack of saliva. A large variety of causes can lead to xerostomia, eg, radiotherapy and chemotherapy,1–4 the chronic use of drugs,5–7 and rheumatic and dysmetabolic diseases.8,9
Saliva is an important host defense component of the oral cavity. Major salivary glands contribute to most of the secretion volume and electrolyte content of saliva (the parotid, submandibular, and sublingual glands, which account for 90% of saliva production), whereas minor salivary glands contribute little secretion volume and most of the blood-group substance.10 Saliva components interact in related functions in the following general areas:
bicarbonates, phosphates, and urea act to modulate pH and the buffering capacity of saliva;
macromolecule proteins and mucins serve to cleanse, aggregate, and/or attach oral microorganisms and contribute to the dental plaque metabolism;
calcium, phosphates, and proteins work together as an antisolubility factor and modulate demineralization and remineralization of tooth surfaces;
immunoglobulins, proteins, and enzymes provide antibacterial action.
Objectively, patients affected by xerostomia have a hypofunction of the salivary output11,12 leading to functional oral disorders such as sore throat, altered taste, dental decay, changes in voice quality, and impaired chewing and swallowing function.13 These factors may ultimately cause reduced nutritional intake and weight loss and significantly affect general health and quality of life of the subjects involved.
Head and neck cancer (HNC) actually includes many different malignancies. The most common type of cancer in the head and neck is squamous cell carcinoma, which originates in the cells that line the inside of the paranasal sinuses, nasal cavity, salivary glands, oral cavity, esophagus, pharynx, and larynx.14 Worldwide, lip and oral cavity cancer along with thyroid cancer has the highest incidence; esophagus cancer is the most aggressive presenting a 4.9% mortality rate (Table 1).
Table 1.
World incidence, mortality, and 5-year prevalence of head and neck cancer
| Cancer | Incidence
|
Mortality
|
5-year prevalence
|
||||||
|---|---|---|---|---|---|---|---|---|---|
| Number | % | ASR (W) | Number | % | ASR (W) | Number | % | Proportion | |
| Lip, oral cavity | 300,373 | 2.1 | 4.0 | 145,328 | 1.8 | 1.9 | 702,149 | 2.2 | 13.5 |
| Nasopharynx | 86,691 | 0.6 | 1.2 | 50,828 | 0.6 | 0.7 | 228,698 | 0.7 | 4.4 |
| Other pharynx | 142,387 | 1.0 | 1.9 | 96,090 | 1.2 | 1.3 | 309,991 | 1.0 | 6.0 |
| Esophagus | 455,784 | 3.2 | 5.9 | 400,156 | 4.9 | 5.0 | 464,063 | 1.4 | 8.9 |
| Larynx | 156,877 | 1.1 | 2.1 | 83,376 | 1.0 | 1.1 | 441,675 | 1.4 | 8.5 |
| Thyroid | 298,102 | 2.1 | 4.0 | 39,769 | 0.5 | 0.5 | 1,206,075 | 3.7 | 23.2 |
Notes: % = risk of getting or dying from the disease before age 75.
Abbreviation: ASR, age-standardized rate.
Similar findings regarding the incidence, mortality, and prevalence of cancer in the European Union have been reported. The highest mortality rate belongs again to esophagus cancer with a predominance of 2.3% (Table 2).
Table 2.
European Union incidence, mortality, and 5-year prevalence of head and neck cancer
| Cancer | Incidence
|
Mortality
|
5-year prevalence
|
||||||
|---|---|---|---|---|---|---|---|---|---|
| Number | % | ASR (W) | Number | % | ASR (W) | Number | % | Proportion | |
| Lip, oral cavity | 43,847 | 1.6 | 4.9 | 14,467 | 1.1 | 1.5 | 121,633 | 1.7 | 28.4 |
| Nasopharynx | 3,267 | 0.1 | 0.4 | 1,494 | 0.1 | 0.2 | 9,283 | 0.1 | 2.2 |
| Other pharynx | 26,585 | 1.0 | 3.2 | 12,583 | 1.0 | 1.4 | 67,590 | 0.9 | 15.8 |
| Esophagus | 34,777 | 1.3 | 3.4 | 29,845 | 2.3 | 2.8 | 38,086 | 0.5 | 8.9 |
| Larynx | 28,336 | 1.1 | 3.1 | 12,248 | 1.0 | 1.2 | 94,193 | 1.3 | 22.0 |
| Thyroid | 37,440 | 1.4 | 5.4 | 3,637 | 0.3 | 0.3 | 149,044 | 2.1 | 34.8 |
Note: % = risk of getting or dying from the disease before age 75.
Abbreviation: ASR, age-standardized rate.
Other less common types of HNCs include salivary gland tumors, lymphomas, and sarcomas.15
The way a particular HNC behaves depends on the primary site in which it arises, and the spread to the lymph nodes in the neck is relatively common.
A patient may receive radiotherapy before, during, or after surgery. Some patients may receive radiotherapy alone without surgery or any other treatment; others may receive radiotherapy and chemotherapy at the same time. The timing of radiotherapy depends on the type of cancer and on the goal of the treatment (cure or palliation). Radiotherapy treats cancer by using doses of high-energy X-rays to destroy the cancer cells while avoiding as much harm as possible to normal cells. The treatment is usually given every weekday with a pause at the weekend; some protocols are based on more than one irradiation a day, and occasionally include therapy during the weekend. The treatment will usually last 3–7 weeks, depending on the type and size of the cancer. Most of the time, patients with HNC treated with radiotherapy receive a dose between 50 Gy and 70 Gy once a day for 5 days a week (2 Gy per fraction);4 on the other hand, if the radiotherapy protocol is just preoperative, the total amount of radiation is usually lower. Conformal radiotherapy is the most common type of radiotherapy used for the treatment of HNC; a special attachment to the radiotherapy machine carefully arranges the radiation beams to match the shape of the cancer, reducing the radiation to the surrounding healthy cells. Another similar type of radiotherapy used against HNC, known as intensity-modulated radiotherapy, allows a more accurate delivery of specific radiation to be distributed to the tumor mass according to its location and severity, sparing the tissue and organs at risk, eg, salivary glands.10
Aims
The aim of the study is to systematically determine the current treatment option for cancer-/radiation-induced xerostomia among patients treated for HNC, and to describe the strategic prevention and management enhancements.
Materials and methods
Systematic review methodology
Search strategy
A first systematic literature search for articles published between January 1, 1970 and June 30, 2013 was conducted in the databases MEDLINE/PubMed and the Cochrane Library, using combinations of the MeSH terms: [Saliva] OR [Salivary Glands] OR [Saliva Flow] OR [Salivation] OR [Salivary Gland Diseases] OR [Xerostomia] OR [Saliva in Xerostomia] OR [Dry Mouth] OR [Oral Dryness] OR [Composition Saliva Xerostomia] AND [Head and Neck Cancer] OR [Radiotherapy] OR [Radiation-induced Xerostomia] OR [Parotid-Sparing Intensity-Modulated Radiotherapy] AND [Quality of Life Analysis-Xerostomia] OR [Management Strategies Salivary Gland Hypofunction] OR [Prevention Xerostomia] OR [Treatment Xerostomia]. The search results were imported into a computerized database Review Manager 5.2. The search results from each of the electronic databases of MEDLINE/PubMed and the Cochrane Library were combined, and duplicated publications were eliminated. Subsequently, an update to include studies published up to June 30, 2013, was performed.
Criteria for selecting studies
After completing the search, articles for review were selected based on:
English language
Original data of cancer therapy protocols
Oral complications associated with cancer therapies
Human.
Exclusion criteria
The reasons for exclusion were defined as follows:
Studies without original and/or actual data
Studies with data from previous publications
Opinion papers
Editorials.
In this way, a preliminary set of potentially relevant publications, removing irrelevant citations according to the criteria, was created. Two reviewers (RP and GC) independently screened the registered title and abstracts, and author and references in two separate files (one for included abstracts and one for excluded abstracts) using a screening guide based on eligibility criteria. Studies rejected at this stage or subsequent stages were reported in the table of excluded studies (Table 3). The full text of all potentially eligible studies in at least one screening was retrieved. Reviewers then evaluated the full text for inclusion using a screening guide and a second reviewer (RP) screened all the findings. When disagreement occurred, a third reviewer (IM) was consulted. For each review, the following information was recorded: year, authors, journal, aim, and number of papers reviewed (Table 4); and for clinical trial papers included: year, authors, journal, aim, number of patients, and results (Table 5). All studies meeting the inclusion criteria then underwent validity assessment. Two examiners (RP and GC) read the papers independently. The qualities and relevance of each study were graded as follows: high (+++), medium (++), or low (+) using a study-quality checklist. External validity, internal validity, and study precision were analyzed to obtain an overall assessment of quality. The assessment was used as a basis for the discussion between the two examiners to grade the studies. In the case of disagreement, all authors discussed the paper until a consensus was reached.
Table 3.
Papers excluded
Table 4.
Reviews included
| Reference | Year | Authors | Journal | Aim | Number of papers reviewed | Qualities and relevance of studies included score |
|---|---|---|---|---|---|---|
| 23 | 1977 | Dreizen et al | Postgrad Med | Narrative – To evaluate the main injury of the surrounding tissues during radiotherapy for oral cancer that can have devastating physical and psychological consequences for the patients | 13 | ++ |
| 45 | 1994 | Atkinson and Wu | J Am Dent Assoc | Narrative – To evaluate the three most common known causes (medication, radiotherapy, and Sjögren’s syndrome) of salivary gland dysfunction and their clinical management | 62 | +++ |
| 17 | 1996 | Scully and Epstein | Eur J Cancer B Oral Oncol | Narrative – To discuss the etiopathogenesis and current means available for preventing, ameliorating, and treating radiotherapy complications, as well as indicating research directions | 282 | +++ |
| 1 | 1998 | Bivona | N Y State Dent J | Narrative – To evaluate generally physiopathological features and clinical management of Sjögren’s syndrome | 16 | ++ |
| 61 | 2000 | Dyke | Int J Pharm Compound | Narrative – To evaluate physiopathological features and clinical management of Sjögren’s syndrome | 19 | + |
| 18 | 2000 | Sreebny | Int Dent J | Systematic – This paper reviews the role of saliva, the prevalence of oral dryness, and consequent importance of salivary flow as well as the relationship between xerostomia and salivary gland hypofunction among the causes of oral dryness. Other aspects: association between saliva and Sjögren’s syndrome and esophageal function; use of saliva as diagnostic tool | 134 | +++ |
| 47 | 2002 | Pedersen et al | Oral Dis | Narrative – This paper reviews the role of human saliva and its compositional elements in relation to the gastrointestinal functions of taste, mastication, bolus formation, enzymatic digestion, and swallowing | 161 | + |
| 2 | 2003 | Cassolato and Turnbull | Gerodontology | Narrative – To outline for clinicians the common etiologies, clinical identification, and routine therapeutic modalities available for individuals with xerostomia | 86 | +++ |
| 12 | 2004 | Porter et al | Oral Surg Oral Med Ora Pathol Oral Radiol Endod | Narrative – To create an update of the etiology and management of xerostomia | 229 | +++ |
| 14 | 2008 | Argiris et al | Lancet | Narrative – To review the epidemiology, molecular pathogenesis, diagnosis and staging, and the latest multimodal management of squamous cell carcinoma of the HNC | 153 | +++ |
| 63 | 2008 | Sagar | Curr Treat Options Oncol | Narrative – To describe the effectiveness of acupuncture to control the symptoms of cancer patients, with an evidence-based approach | 59 | ++ |
| 55 | 2010 | Ramos-Casals et al | JAMA | Systematic – To summarize evidence on primary Sjögren’s syndrome drug therapy from randomized controlled trials | 74 | + |
| 10 | 2010 | Jensen et al | Support Care Cancer | Systematic – To assess the literature for management strategies and economic impact of salivary gland hypofunction and xerostomia induced by cancer therapies and to determine the quality of evidence-based management recommendations | 154 | +++ |
| 10 | 2010 | Jensen et al | Support Care Cancer | Systematic – To assess the literature for prevalence, severity, and impact on quality of life of salivary gland hypofunction and xerostomia induced by cancer therapies | 203 | +++ |
| 66 | 2010 | O’Sullivan and Higginson | Acupunct Med | Systematic – To systematically review evidence on clinical effectiveness and safety of acupuncture in irradiation-induced xerostomia in patients with HNC | 51 | +++ |
| 41 | 2013 | Radvansky et al | Am J Health Syst Pharm | Narrative – To evaluate current strategies for preventing and managing radiation-induced dermatitis, mucositis, and xerostomia, with an emphasis on pharmacologic interventions | 52 | ++ |
| 67 | 2013 | Zhuang et al | Integr Cancer Ther | Systematic – To evaluate the preventive and therapeutic effect of acupuncture for radiation-induced xerostomia among patients with HNC | 46 | +++ |
Notes: +++, high level; ++, medium level; +, low level.
Abbreviation: HNC, head and neck cancer.
Table 5.
Clinical trial papers included
| Reference | Year | Authors | Journal | Aim | Number of patients | Results | Qualities and relevance of studies included score |
|---|---|---|---|---|---|---|---|
| 35 | 1974 | Brown et al | J Dent Res | To assess the effects of radiation-induced xerostomia on the human oral microflora | 30 | Cariogenic microorganisms gain prominence at the expense of non-cariogenic microorganisms in concert with saliva shutdown | +++ |
| 49 | 1974 | Chen and Webster | Cancer | One hundred and one cases of head and neck cancer were subjected to oral culture for Candida albicans before, during, and l month after radiotherapy | 101 | Thirty percent of the patients had a positive culture before radiotherapy. During the course of radiotherapy, almost half of the negative patients turned positive. The severity of the acute radiation reaction of the oropharyngeal mucosa was not related to the apparent presence or absence of C. albicans. Amphotericin B (1 cm3 [100 mg] four times daily) converted about one-third of the positive patients to negative | ++ |
| 24 | 1975 | Ben-Aryeh et al | Int J Oral Surg | Flow rate, pH, electrolytes, protein, and phosphate evaluation of whole saliva in 15 healthy individuals and 15 patients with malignant tumors in the head and neck region before and during irradiation therapy | 30 | The most significant finding was the increased sodium content. Irradiation reduces the reabsorption ability of the tubuli, causing the sodium content of the saliva to increase | ++ |
| 25 | 1976 | Dreizen et al | Cancer | Saliva and serum electrolyte concentrations were monitored in 30 patients given a course of xerostomia-producing cancer radiotherapy | 30 | The xerostomic saliva was more concentrated and had a greater salinity than the pretreatment saliva in each instance. In contrast, none of the serum electrolytes measured was significantly altered by the subtotal salivary shutdown | ++ |
| 28 | 1981 | Abelson and Mandel | J Dent Res | To evaluate the impact of the saliva on plaque in vivo, following exposure to a sucrose substrate, in ten caries-resistant and ten caries-susceptible subjects under varying conditions of salivary access | 20 | The study results indicate that saliva plays a major role in mediating plaque pH and qualitatively reflects caries status | + |
| 36 | 1981 | Keene et al | Caries Res | To evaluate the prevalence of Streptococcus mutans in both preradiation and irradiation patients | 39 | S. mutans were detected in 82% of the irradiated patients and 100% of the preradiotherapy patients. In the irradiated group without current caries, S. mutans prevalence was inversely related to the number of elapsed years postradiotherapy | +++ |
| 34 | 1981 | Izutsu et al | Oral Surg Oral Med Oral Pathol | Albumin concentrations were measured in whole and parotid saliva samples collected from patients who were undergoing various cancer treatment protocols and had a high incidence of stomatitis | 7 | The salivary albumin increases always preceded and often occurred in the absence of stomatitis, suggesting that the whole saliva albumin level may be a useful measure and predictor of this condition | ++ |
| 26 | 1981 | Marks et al | Int J Radiat Oncol Biol Phys | To establish a dose–response curve for the human parotid, selective measurements of right and left parotid salivary flow were done for 15 age-matched control patients whose parotids were not irradiated, 17 patients who had both parotids irradiated, and 12 whose parotids were irradiated by unilateral electron beam technique | 46 | In this study there clearly exists a dose–response correlation for the late effects of radiation on parotid salivary flow. Indeed, parotid salivary flow progressively decreased with increasing doses of radiation. A change in the pH of saliva that, especially at high doses, becomes acidic was found | +++ |
| 33 | 1986 | Makkonen et al | Oral Surg Oral Med Oral Pathol | To analyze the radiation-induced changes in the flow rate and protein composition of stimulated whole saliva in eleven patients treated for malignant conditions of the head and neck | 11 | It is concluded that the observed qualitative changes in whole saliva components are net effects caused by the cancer itself, radiotherapy given, systemic diseases, or medications, as well as mucosal inflammations | +++ |
| 11 | 1987 | Fox et al | J Am Dent Assoc | Describes the responses to a questionnaire of oral findings and QOL in patients with reduced saliva flow. Moreover, an objective measurement of the major saliva output unstimulated and stimulated | 100 | In this study there exists a correlation between clinical symptoms and low-rate salivary flow. The questionnaire clearly helps to identify xerostomic patients and allows appropriate management to begin | ++ |
| 37 | 1988 | Hase and Birkhed | Arch Oral Biol | The aim was to study the effect of different salivary secretion rates on glucose clearance in saliva and on pH change in dental plaque in man, in normal and hyposalivation conditions | The pH changes in dental plaque after the mouth rinse with glucose at extremely low secretion rate were significantly more pronounced than the normal flow rate. Thus, the salivary secretion rate affects both the glucose clearance in saliva and the pH changes in dental plaque in man | + | |
| 16 | 1991 | Maciejewski et al | Radiother Oncol | To evaluate the effects and efficacy of the application of 2% silver-nitrate solution for several days before radiotherapy in 16 patients treated for squamous cell carcinoma of the oral cavity or oropharynx | 16 | The application of solutions and astringents is effective in modifying the development of acute side effects of radiotherapy and to decrease signs, symptoms, and suffering by modulating the biological status of critical normal tissue before the onset of radiotherapy. Unfortunately, their application before radiotherapy has not given significant results in order to promote reparative processes | +++ |
| 29 | 1993 | Lingström and Birkhed | Acta Odontol Scand | To evaluate plaque pH and oral retention after consumption of starchy snack products at normal and low salivary secretion rate | 10 | All products resulted in greater pH falls and remained at a low level for a longer period during low secretion rate. There were no differences in concentration of carbohydrates in saliva after consumption of starchy snack products. Low secretion rate increased the oral retention for all products | ++ |
| 32 | 1993 | Valdez et al | Cancer | To evaluate whether the sialogogue pilocarpine given during radiotherapy may reduce the severity of xerostomia and salivary dysfunction. The patients, requiring head, neck, or mantle radiotherapy, took either 5 mg of pilocarpine or placebo four times daily for 3 months, beginning the day before radiotherapy. Subjective complaints and salivary functions were assessed | 10 | The stimulation with pilocarpine may reduce the severity of salivary dysfunction and associated oral symptoms during radiotherapy | ++ |
| 60 | 1997 | Bagheri et al | Eur J Clin Pharmacol | To compare the effects of yohimbine, an alpha-2 adrenoceptor antagonist, and anethole trithione, a reference drug in the treatment of dry mouth, in patients treated with psychotropic drugs (tricyclic antidepressants or neuroleptics) and suffering from xerostomia | 10 | The study results show that under experimental conditions, yohimbine, but not anethole trithione, stimulates salivary secretion after a 5-day treatment in patients receiving antidepressants or neuroleptics and suffering from dry mouth | + |
| 48 | 1997 | Ramirez-Amador et al | Oral Med Oral Pathol Oral Radiol Endod | To quantitate oral Candida colonization, assessing symptoms, and response to antifungal management, especially Candida, and evaluate the influence of smoking and dentures | 46 | When salivary glands are included in the field of radiation, xerostomia occurs causing progressive increases in oral Candida colonization. Because 17.4% developed clinical candidiasis during radiotherapy and the question of fungal resistance remains speculative, a recommendation for the prophylactic use of antifungal medication is unresolved | +++ |
| 31 | 1998 | Almståhl and Wikström | J Dent Res | To evaluate the effect of hyposalivation on the oral microflora | 38 | The results indicated that a low salivary secretion rate mainly promotes a flora associated with the development of caries | +++ |
| 38 | 1998 | Ravald and List | Swed Dent J | The investigation is designed to study caries and periodontal conditions in a selected group of patients with primary Sjögren’s syndrome. Clinical examination includes registrations of dental caries, restorations, and periodontal condition | 21 | The patients with primary Sjögren’s syndrome face a high risk of developing both coronal and root caries due to xerostomia. The periodontal conditions are similar to those found in patient groups in general dentistry | ++ |
| 13 | 1999 | De-Graeff et al | Oral Oncol | To describe prospectively the QOL and mood in patients with oral or oropharyngeal cancer treated with surgery radiotherapy | 75 | After treatment, a gradual improvement in emotional functioning occurred. Surgical treatment for oral or oropharyngeal cancer results in significant deterioration of physical functioning and symptoms during the first year, especially when combined with radiotherapy | +++ |
| 59 | 1999 | Hamada et al | Am J Med Sci | To evaluate the efficacy of AT, a cholagogue, for xerostomia signs management | 49 | The results indicate that AT sufficiently stimulates salivation and improves xerostomia | +++ |
| 39 | 2001 | Almståhl et al | Oral Microbiol Immunol | To compare lactoferrin, amylase, and MUC5B concentrations in stimulated whole saliva collected from subjects with radiation-induced hyposalivation, subjects with primary Sjögren’s syndrome, and subjects with hyposalivation of unknown origin or due to medicines. In addition, the data in relation to the presence of selected microbial species that have been associated with oral disorders were analyzed | 75 | The saliva composition in subjects with hyposalivation of unknown origin or due to medicines was close to that in the healthy controls. All three hyposalivation groups tended to display a decrease in the concentrations of MUC5B and amylase. None of the microbial species analyzed correlated with concentration of MUC5B in saliva | +++ |
| 20 | 2001 | Burlage et al | Radiother Oncol | It was studied whether differences in acute radiosensitivity exist between parotid and submandibular/sublingual glands | 18 | The results revealed that salivary flow rates decreased dramatically during the first 2 weeks of radiotherapy. Neither recovery nor significant differences were observed between the production of saliva from the parotid and submandibular/sublingual glands during the 13-week observation period | +++ |
| 21 | 2001 | Epstein et al | Head Neck | To assess the QOL, oral function, and oral symptoms in a cohort of patients during and after radiotherapy, by QLQ-C30, with an added oral symptom and function | 20 | The EORTC QLQ-C30 questionnaire with the oral assessment addendum provides a measure of the QOL and oral function in head and neck cancer patients and may provide useful outcome measures for assessment of oral care prevention and management strategies in these patient populations | ++ |
| 9 | 2001 | Moore et al | Oral Surg Oral Med Oral Pathol Oral Radiol Endod | The study evaluates the prevalence of dry-mouth symptoms (xerostomia), the prevalence of hyposalivation in this population, and the possible interrelationships between salivary dysfunction and diabetic complications | 676 | Subjects with type 1 diabetes who had developed neuropathy more often reported symptoms of dry mouth as well as symptoms of decreased salivary flow rates | + |
| 42 | 2002 | Wijers et al | Head Neck | The first aim of the study was to evaluate the degree of xerostomia in 39 long-term survivors* treated between 1965 and 1995 by conventional 2D radiotherapy and currently without evidence of disease. The second aim was to develop a concise instrument to evaluate the subjective aspects of xerostomia | 39 | In this survey, 64% of the long-term survivors*, after treatment by conventional 2D radiotherapy for a malignancy in the head and neck region, still experienced a moderate-to-severe degree of permanent xerostomia | ++ |
| 56 | 2004 | Hendrickson et al | J Emerg Med | A report of a case of unintentional overdose of oral pilocarpine tablets that resulted in bradycardia, mild hypotension, and muscarinic symptoms in a patient with Sjögren’s syndrome | 1 | ++ | |
| 53 | 2004 | Koseki et al | Oral Dis | To investigate oral symptoms and clinical parameters in dry eye patients | 224 | The sensation of a dry mouth and changes in oral soft tissues, dental caries, and oral Candida frequently occurred in dry eye patients | ++ |
| 30 | 2006 | Eliasson et al | Eur J Oral Sci | To investigate the secretion rate from palatal, buccal, and labial glands, and to analyze the IgA concentrations in relation to age, sex, circulatory disease, diabetes, medication, smoking, and pregnancy | 142 | The results did not suggest any effect of aging on the secretion capacity of minor salivary glands, but the IgA concentration seemed to increase with age. Women had lower buccal and labial saliva secretion rates, and lower levels of IgA in buccal saliva, than men. For whole saliva, resting, but not stimulated, saliva secretion rates were reduced with age, and the secretion rate of stimulated whole saliva was lower in women than in men | + |
| 57 | 2007 | Chambers et al | Int J Radiat Oncol Biol Phys | To assess the safety of long-term cevimeline treatment of radiation-induced xerostomia in patients with head and neck cancer; and to assess the efficacy of cevimeline in these patients | 255 | Cevimeline 45 mg three times daily was generally well tolerated over a period of 52 weeks in subjects with xerostomia secondary to radiotherapy for cancer in the head and neck region | +++ |
| 57 | 2007 | Chambers et al | Int J Radiat Oncol Biol Phys | To study the efficacy and safety of cevimeline in two double-blind trials enrolling patients with head and neck cancer in whom xerostomia developed after radiotherapy | 500 | Cevimeline was well tolerated by patients with xerostomia after radiotherapy for head and neck cancer, and oral administration of 30–45 mg of cevimeline three times daily increased unstimulated salivary flow | +++ |
| 4 | 2009 | Brand et al | Br Dent J | To assess the severity of xerostomia in HSCT patients and to investigate the association of xerostomia with other chronic oral complications | 89 | HSCT patients have more severe xerostomia, which is associated with other oral complaints | + |
| 8 | 2009 | Busato et al | Oral Surg Oral Med Oral Pathol Oral Radiol Endod | To evaluate the impact of xerostomia on the QOL of adolescents with DM1 | 56 | Xerostomia is frequent and has a negative impact on QOL of adolescents with DM1 | +++ |
| 54 | 2010 | Tomiita et al | Mod Rheumatol | To evaluate the efficacy and safety of orally administered pilocarpine hydrochloride for juvenile-onset Sjögren’s syndrome patients | 5 | The results of this study suggest that orally administered pilocarpine is safe and effective for treating xerostomia in juvenile-onset Sjögren’s syndrome patients | + |
| 40 | 2010 | Almståhl et al | Arch Oral Biol | To analyze the frequency of different Lactobacillus spp. in relation to the pH-lowering potential of the plaque | 30 | There were large intra- and interindividual variations in frequencies of Lactobacillus spp. and Lactobacillus counts, but no specific species could be related to plaque acidogenicity | +++ |
| 52 | 2010 | Almeida and Kowalski | Braz J Otorhinolaryngol | To report on the experience with pilocarpine on the treatment of xerostomia in thyroid cancer patients submitted to adjuvant RIT | 84 | Pilocarpine seems to relieve xerostomia complaints in thyroid cancer patients because it is able to stimulate salivary flow, but the observed side effects made the patients refuse long-term therapy continuation | +++ |
| 43 | 2011 | Sher et al | Int J Radiat Oncol Biol Phys | A retrospective study of all patients treated at the Dana-Farber Cancer Institute for HNCUP with IMRT between August 2004 and January 2009. The primary endpoint was overall survival; the secondary endpoints were locoregional and distant control, and acute and chronic toxicity | 24 | In a single-institution series, IMRT-based chemoradiotherapy for HNCUP was associated with superb overall survival and locoregional control. The xerostomia rates were promising, but the aggressive therapy was associated with significant rates of esophageal stenosis | ++ |
| 7 | 2011 | Villa et al | J Am Dent Assoc | To estimate the prevalence of the subjective perception of dry mouth in dental patients in Italy, to relate these estimates to the patients’ ages and sexes, and to determine whether xerogenic medications taken by these patients were associated with complaints of xerostomia | 1,201 | The authors found that medication use and age were highly significant risk factors for dental patients reporting xerostomia | ++ |
| 6 | 2011 | Villa and Abati | Aust Dent J | To examine the symptoms and risk factors associated with self-reported xerostomia | 601 | Participants reported having dry mouth in 19.6% of cases. Older individuals were significantly more likely to report dry mouth, and the prevalence of xerostomia increased with advancing age. The prevalence of xerostomia in patients taking one or more drugs was significantly higher compared to medication-free patients, and increased with increasing numbers of medications used. Finally, individuals with a nervous or mental disorder, or who wore removable dentures, were five times more likely to develop xerostomia than patients without mental disorder or dentures | ++ |
| 44 | 2012 | Schoenfeld et al | Int J Radiat Oncol Biol Phys | To analyze the recent single-institution experience of patients with salivary gland tumors who had undergone adjuvant IMRT, with or without concurrent chemotherapy | 35 | Treatment of salivary gland malignancies with postoperative IMRT was well tolerated with a high rate of local control. Chemoradiotherapy resulted in excellent local control in a subgroup of patients with adverse prognostic factors and might be warranted in select patients | ++ |
Notes: +++, high level; ++, medium level; +, low level.
The cohort of patients who had been free of disease for 5 years or longer.
Abbreviations: EC, ethylenedicysteine; ECD, N,N′-1,2-ethylenediylbis-l-cysteinediethylester; AT, anethole trithione; QLQ, Quality of Life Questionnaire; IgA, immunoglobulin A; HSCT, hematopoietic stem cell transplantation; QOL, quality of life; DM1, type 1 diabetes mellitus; RIT, radioactive iodine therapy; HNCUP, head and neck squamous cell carcinoma; IMRT, intensity-modulated radiotherapy; 2D, two-dimensional; EORTC, European Organization for Research and Treatment of Cancer; QLQ-C30, Quality of Life Questionnaire.
Results
The electronic searches identified about 1,000 titles and abstracts, and after reviewing the titles, 411 studies were evaluated. Subsequently, during the review of the abstract, 336 studies were excluded. The final analysis included 70 articles that conformed to the criteria for the present review (Figure 1). Although animal studies have been excluded, important information regarding the experimental results on two of the papers was considered useful and therefore they were discussed.
Figure 1.
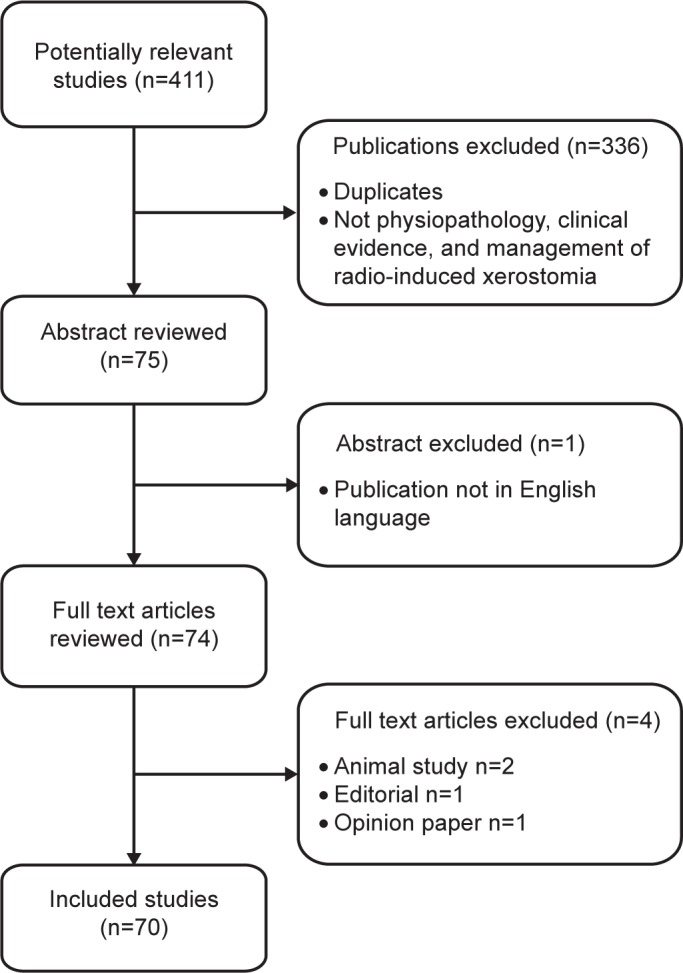
Search flowchart.
Physiopathological and clinical consequences in cancer therapy
Each of the reviews concerning the physiopathological and clinical consequences are listed in Table 6.
Table 6.
Reviews included related to physiopathological and clinical consequences in cancer therapy
| Reference | Year | Authors | Journal | Aim | Number of papers reviewed | Qualities and relevance of studies included score |
|---|---|---|---|---|---|---|
| Physiopathological consequences | ||||||
| 17 | 1996 | Scully and Epstein | Eur J Cancer B Oral Oncol | Narrative – To discuss the etiopathogenesis and current means available for preventing, ameliorating, and treating these complications, as well as indicating research directions | 282 | +++ |
| 18 | 2000 | Sreebny | Int Dent J | Systematic – This paper reviews the role of saliva, the prevalence of oral dryness, and consequent importance of salivary flow as well as the relationship between xerostomia and salivary gland hypofunction among the causes of oral dryness. Other aspects: associations between saliva and Sjögren’s syndrome and esophageal function; use of saliva as diagnostic tool | 134 | +++ |
| Radiation-induced changes of saliva | ||||||
| 23 | 1977 | Dreizen et al | Postgrad Med | Narrative – To evaluate the main injury to surrounding tissues during radiotherapy for oral cancer that can have devastating physical and psychological consequences for the patients | 13 | ++ |
| Radiotherapy clinical consequences | ||||||
| 45 | 1994 | Atkinson and Wu | J Am Dent Assoc | Narrative – To evaluate the three most common known causes (medication, radiotherapy, and Sjögren’s syndrome) of salivary gland dysfunction and their clinical management | 62 | +++ |
| 47 | 2002 | Pedersen et al | Oral Dis | Narrative – This paper reviews the role of human saliva and its compositional elements in relation to the gastrointestinal functions of taste, mastication, bolus formation, enzymatic digestion, and swallowing | 161 | + |
| 41 | 2013 | Radvansky et al | Am J Health Syst Pharm | Narrative – To evaluate current strategies for preventing and managing radiation-induced dermatitis, mucositis, and xerostomia, with an emphasis on pharmacologic interventions | 52 | ++ |
Notes: +++, high level; ++, medium level; +, low level.
Physiopathological consequences
A total of six articles reported the physiopathological effects of radiotherapy on salivary glands parenchyma: one systematic review, one narrative review, one pilot study, one animal experimentation study, and one cohort study.16–20 Radiotherapy-induced xerostomia could be considered a multifactorial disease. On the one hand, the damage to the oral cavity has been strongly related to the radiation dose, fraction size, volume of irradiated tissue, fractionation scheme, and type of ionizing irradiation, but on the other, it may be difficult to distinguish changes caused by radiotherapy itself from those related to the malignant disease, the concomitant systemic diseases, and the medication needed for the treatment of the cancer.16,17
The salivary glands are superficially located compared to most head and neck tumors, and thus, the ionizing radiation has to pass through the salivary glands to effectively treat the tumor.18 Tissues with a rapid turnover rate are more susceptible than tissues with a slow one and even with the most accurate therapeutic protocol, X-rays cause unwanted changes in non-tumoral tissues. Despite the fact that salivary gland cells turnover is slow, production and quality of saliva change after radiation, so they are not as radioresistant as they are supposed to be.19 There are differences among the various types of salivary glands; in fact, the submandibular gland is less radiosensitive than the parotid gland.20 From this point of view, the most severe and irreversible forms of salivary gland hypofunction result from the damage/loss of salivary acinar cells, giving rise to rapid and predictable compositional changes, and reduction in saliva production and in the quality of the flow.
Radiation-induced changes in saliva
Nineteen articles analyzed the effects of the radiotherapy on salivary flow and composition, and the changes in microbial population: one narrative review, four randomized controlled trials, nine cohort studies, and five cross-sectional studies.21–40
Salivary flow
One of the main problems resulting from tissue damage generated by radiotherapy is the reduction of salivary flow. The radiation level necessary to cause severe dysfunction to gland tissue is >52 Gy. Below this threshold, the radiation damage generally has a transient and reversible duration.12 Routinely, HNC patients receive a total of 50–70 Gy, the radiation dose normally used to destroy malignant cells, which very often leads to the onset of chronic xerostomia.21 The major reduction in salivation after radiotherapy is observed in the period from the onset of radiotherapy to 3 months after completion. During radiotherapy, the first 10 days are the worst ones as a massive decrease in saliva production occurs; especially in the first week, it could reduce by 50%–60%.22 After this period, the flow rate is reduced by <10% of the initial conditions.23
Chemical and immunochemical alterations
Radiotherapy can also induce alterations in electrolytes and antibacterial systems. Salivary electrolyte levels are altered, with an increase in the concentrations of sodium, chloride, calcium, and magnesium, while potassium is only slightly affected.24 Saliva also reduces the buffering capacity in irradiated patients due to a reduction of bicarbonate concentration in parotid saliva.25,26 Saliva becomes, moreover, highly viscous, and reduces its pH from about 7.0 to 5.025,27 with slow recovery to the neutral pH in dental plaque after a sugar rinse.28,29 The permanence of the acidic pH in dental plaque was related to the reduced buccal gland saliva flow30 as the secretion from the buccal glands, closely delivered to the teeth surfaces, could affect the dental plaque more than the whole saliva during resting conditions.
Changes also involve the nonimmune and immune antibacterial systems. The concentrations of immunoproteins (eg, secretory immunoglobulin A), lysozyme, and lactoferrin are increased, as well as the serum and non-salivary components.31–34 However, the decrease in salivary flow rate is greater than the increase in immunoprotein and lysozyme levels, and this results in significant immunoprotein deficit. Since the reduction of the oral clearance, immunologic mechanisms and buffering capacity of saliva are altered, and the host protection decreases giving rise to changes in the oral flora.35
Microbial changes
All of these radiation-induced changes cause a different oral flora growth and acidogenic, cariogenic microorganisms are more present than non-cariogenic microorganisms. Unfortunately, even if there is an increase in immunoprotein and lysozyme levels, a significant immunoprotein deficit occurs due to the decrease in salivary flow rate. Streptococcus mutans, Lactobacillus spp., and Candida spp. are the most prevalent in the plaque of irradiated patients.30,36–38 In a longitudinal study, Brown et al assessed the effects of radiation-induced xerostomia on the human oral microflora and on the subsequent development of dental caries.35 Five intraoral specimens consisting of resting saliva, gingival sulcus fluid, dental plaque, lingual swabs, and stimulated whole saliva were collected from each patient two times during 1 week before radiation, one time per week during radiotherapy, at 3-month intervals during the first postradiation year, and at 6-month intervals thereafter. During irradiation, the development of xerostomia was matched by a parallel and pronounced shift in certain microbial populations at each intraoral site assessed. The most prominent changes were the increase in S. mutans and species of Lactobacillus, Candida (primarily Candida albicans), and Staphylococcus, with parallel decreases in Streptococcus sanguis and species of Neisseria and Fusobacterium. Microbial differences were relatively minimal between the groups of patients receiving radiotherapy who used a fluoride gel and a nonfluoride gel during the irradiation period. However, there was a more rapid decrease in the level of S. sanguis in the plaque of the patients using the nonfluoride gel compared with those patients using the fluoride gel, and the subsequent development of dental caries differed greatly. The increased number of Lactobacilli was correlated to a high acidic potential of the plaque and the use of fluoride was associated with a protective effect in the prevention of dental decay during xerostomia.
The findings that a high frequency, number, and proportion of Lactobacillus spp. occur in irradiated patients were strengthened by a study of Almståhl et al who analyzed the saliva oral microbiota in subjects with hyposalivation using a rinsing technique and a cultivation technique. Results indicated that the salivary secretion rate, pH, and buffer capacity were the more important factors in the increase in Lactobacillus spp. A marked increase in C. albicans was also characteristic of the irradiated patients.39
In a more recent study, Almståhl et al evaluated the frequency of different Lactobacillus spp. in relation to the pH-lowering potential of the supra-gingival plaque in irradiated patients in comparison to primary Sjögren’s syndrome patients and controls with normal salivary secretion.40 The irradiated subjects had finished their bilateral radiation treatment (64.6 Gy) 3–5 years before participating in the study. Interproximal plaque pH was measured by the microtouch method30 before and up to 60 minutes after a 10% sugar rinse.29 The measurements were performed at two sites: in the anterior and in the premolar/molar region. Data indicated that the most common species were Lactobacillus fermentum, Lactobacillus rhamnosus, and Lactobacillus casei. In anterior sites, both the hyposalivated group subjects with high Lactobacillus counts had an increased plaque acidogenicity compared to those with low counts. In posterior sites, subjects with high Lactobacillus counts had a lower final pH compared with those with low counts. Authors concluded that hyposalivation patients often harbor several different Lactobacillus spp. in their supragingival plaque. There were, however, large differences in number and proportion of Lactobacilli between individuals and between anterior and posterior dental sites, but no specific species could be related to plaque acidogenicity.
Radiotherapy clinical consequences
In eleven articles, the clinical consequences that may arise as a result of HNC radiotherapy have been described: three narrative reviews, one randomized clinical trial, one animal experimentation study, four cohort studies, and two cross-sectional studies.20,36,41–50 Radiotherapy can cause some temporary side effects. Although these may be worse if the treatment is combined with chemotherapy, they gradually disappear after the treatment has finished. Most radiotherapy side effects occur toward the middle and end of the course of treatment and continue during the first couple of weeks after the treatment. The effects can be mild or more troublesome, depending on the dose of radiotherapy and the length of treatment. Thus, the quantitative and qualitative salivary changes predispose the irradiated patient to a variety of problems.
Radiotherapy in HNC is inevitably associated with damages to the oral tissues and, in addition, the clinical consequences of radiotherapy include also dermatitis and osteoradionecrosis.41 In fact, salivary glands are often involved and, as a result, patients may have a salivary gland hypofunction, even if 3D planning and unilateral irradiation have considerably reduced the side effects by minimizing the dose to normal tissues. However, the final degree of damage to gland tissue depends on individual patient characteristics, such as pretreatment already done, age, and sex.
Xerostomia may affect 80% of the patients who need radiotherapy as a primary treatment, as an adjunct to surgery, in combination with chemotherapy, or as palliation.42–44 Hyposalivation represents the biggest acute side effect in HNC radiotherapy and, in general, is always associated with oral function problems, such as chewing and swallowing, or caries at a later stage. Normally, during radiotherapy, salivary composition may change and it becomes more viscous than usual, so its color may turn yellow, brown, or even white (Figure 2). Furthermore, salivary glands with high flow rates before the initiation of radiotherapy show less reduction in salivary flow rate. As a consequence of the reduction in the rate of saliva flow, which is correlated to the amount of radiation given to the patient, oral complications occur.20
Figure 2.

Viscous appearance of the saliva in a radiotherapeutic patient.
The buccal mucosa has a dry and sticky appearance (Figure 3). The normally moist, glistening appearance of the oral cavity is often replaced with a thin, pale, cracked appearance that is more susceptible to gingivitis and bleeding. Another frequent acute side effect is oral mucositis, which can be experienced by >50% of patients receiving HNC radiotherapy. Some typical side effects are onset of erythema, edema, and pain in the oral mucosa.41 Patients may also exhibit a dry irritated tongue with an erythematous appearance of the dorsal surface, the hard or soft palate, the commissures of the mouth, and under-removable prostheses.43 Furthermore, the lack of saliva may lead to angular cheilitis, cracked lips (Figure 4), periodontal disease, aching of the mouth, and halitosis.
Figure 3.

Dry and sticky appearance of oral mucosa in a radiotherapeutic patient.
Figure 4.

Cheilitis and cracked lips, and teeth cervical caries in a radiotherapeutic patient.
When part or all of the mouth is treated, the sense of taste may change quickly during the radiotherapy, and some patients may even either lose their sense of taste completely or find that everything tastes the same (usually rather metallic or salty). Changes in taste are correlated to the direct irradiation of the taste buds, and also to the reduction in salivary flow rate that alters the ionic composition of saliva that is related to the sensation of taste.46
Moreover, the loss of saliva compromises mastication and nutrition. Some patients lose their appetite as a general effect of radiotherapy. Dryness of the mouth and lips can cause discomfort, ranging from a mild irritation to a severe burning sensation with difficulties in normal eating habits, particularly eating spicy or acidic food. A sore, dry mouth can also make eating and swallowing difficult because moistening of food is insufficient and oral mucosa surfaces are not wet and not lubricated enough.47
Furthermore, an insufficient lubrication, due to a diminished salivary output, causes intolerance to prosthetic appliances, so more friction is present between the mucosa and the resin that can injure the delicate irradiated epithelial layer. In addition, the inadequate presence of saliva weakens the stability of prostheses in the mouth. Ulceration is more likely because the dry mucosa is more vulnerable to trauma.
A further complication that tends to occur later in irradiated patients is the increased risk of developing dental caries and oral infections, due to the alterations in the saliva flow and consequently in oral microflora.36 The decay is most often recurrent or primary and located at sites generally not usually susceptible to caries such as the cervical margins, incisal margins, or the tips of teeth (Figure 4).
Another issue is the high incidence of yeast infections during xerostomia.48 An example being the C. albicans infection, which is very common in both dentate and edentulous individuals and allows a colonization of oral mucosae49 increasing the risk of oral mucosal infections.50
Another acute side effect of radiotherapy is dermatitis, which can be experienced by up to 95% of patients.41 The skin over the face and neck is very likely to gradually redden or darken and become sore. At the same time, the mouth and throat become sore and inflamed after a couple of weeks of treatment and mouth ulcers may occur; the voice may also become hoarse.
Discussion
The treatment of xerostomia has four aims: increasing existing saliva flow or replacing lost secretions, the control of the state of oral health, the control of dental caries, and the treatment of possible infections.51
Therapy options in xerostomia depend on the presence of residual secretion or the absence of it. When residual secretory capacity is present, it is advisable to regularly stimulate the salivary glands by mechanical or gustatory stimuli as supportive oral care. The use of sugarless chewing gum or candy-containing xylitol or sorbitol can be recommended as a means of stimulating extra salivary flow to aid caries management and lubrication. Nocturnal oral dryness can be alleviated by applying a small amount of dentifrice on smooth dental surfaces, especially using anti-xerostomia dentifrices that contain three salivary enzymes, lactoperoxidase, glucose oxidase, and lysozyme, specifically formulated to activate intraoral bacterial systems.
The salivary flow can also be stimulated by the use of cholinergic pharmaceutical preparations, such as pilocarpine or cevimeline. These two parasympathomimetic drugs are approved by the Food and Drug Administration for treatment of xerostomia; pilocarpine is approved for Sjögren’s syndrome and radiotherapy-induced xerostomia, while cevimeline seems to be more specific for Sjögren’s syndrome. Pilocarpine, a natural alkaloid, is a parasympathomimetic agent with β-adrenergic effects that activates cholinergic receptors,52 stimulating the residual function of the salivary glands. The recommended dose is 5 mg orally three times a day.53 Severe adverse effects are rare, but side effects associated with the use of the drug are vomiting, sweating, headache, increased urinary frequency, wheezing, watery eyes, and nausea, and gastrointestinal intolerance. Hypotension, rhinitis, diarrhea, and visual disturbances can also occur.54,55 Normally, these are moderate in intensity and last for a short period of time. Patients with asthma, high blood pressure, heart diseases, and in therapy with β-blockers cannot use pilocarpine because this drug is a nonselective antagonist of muscarinic receptors and, therefore, it can interfere with the cardiac and respiratory functions in those patients. For the same reason, pilocarpine, stimulating muscarinic receptors in the central nervous system, can cause onset of agitation, confusion, and parkinsonian-like syndromes.56
Cevimeline is analogous to acetylcholine, which binds to muscarinic acetylcholine receptors in exocrine glands, specifically the M1 and M3 subtypes present, for instance, in the epithelium of the salivary and lachrymal glands, leading to an increase in exocrine gland secretion including saliva and sweat. M2 and M4 receptor sites predominate in cardiac and respiratory tissues. This receptor subtype selectivity is presumed to mitigate the systemic adverse effects of muscarinic–cholinergic stimulation.56 It is rapidly absorbed from the gastrointestinal tract, reaching peak concentrations in approximately 90 minutes without food. The duration of its sialogogic effect seems to be unclear. Clinical trials have shown it to be more effective than placebos in relieving the symptoms of a dry mouth. The recommended dose is 30 mg orally three times a day, but in two clinical trials, it has been shown that the use of cevimeline in treating radiation-induced xerostomia, increasing the dose to 45 mg, was well tolerated by patients, with an increase of unstimulated salivary flow.57,58 This medication is not recommended for patients with uncontrolled asthma, narrow-angle glaucoma, or iritis. Excessive sweating and nausea are the most frequently reported adverse effects with cevimeline. Rhinitis, diarrhea, and visual disturbances, especially at night, can also occur.
Another medication is anethole trithione that is a bile secretion-stimulating drug, or cholagogue. It increases the secretion of acetylcholine and stimulates the parasympathetic nervous system, and so as a result, we have the stimulation of salivation from serous acinar cells. This medication has been used for many years in the treatment of chronic xerostomia, but reports differ regarding its efficacy. While some studies report improvements in salivary flow rates in drug-induced xerostomia, trials in patients with Sjögren’s syndrome show conflicting results. Side effects reported include abdominal discomfort and flatulence. Dosages of 75 mg three times daily may be effective in treating patients with mild-to-moderate symptoms of xerostomia, but further research is needed to establish its safety and efficacy in this setting.59
Yohimbine has also been used in patients with xerostomia and it is an alpha-2 adrenergic antagonist, which induces an increase in cholinergic activity peripherally. In one randomized, double-blind, crossover study, the effect of this medication was compared to that of anethole trithione in patients treated with psychotropic medications. Patients given yohimbine 6 mg three times daily for 5 days showed significantly increased saliva flow (P<0.01) when compared with anethole trithione 25 mg three times daily.60
Human interferon alfa (IFN-α) is currently undergoing clinical trials to determine the safety and efficacy of low-dose lozenges in the treatment of salivary gland dysfunction and xerostomia. In one study, IFN-α lozenges at dosages of 150 IU given three times daily for 12 weeks resulted in a significant increase in stimulated whole saliva (P=0.04) when compared with placebos.61
If some residual function of salivary glands remains, acupuncture could be a good alternative treatment for alleviating radio-induced xerostomia.62 The way this works remains poorly understood, but it seems that acupuncture modulates central nervous system processes,63 increasing the concentration of salivary neuropeptides, which seem capable of modulating the complex process of salivary secretion.64 There are some studies that provide encouraging results, suggesting an effective increase in salivary flow, while others do not detect statistically significant differences in the increase in salivary flow between the treated subjects and controls.65 However, the results of systematic reviews do not indicate the efficacy of acupuncture in the treatment of xerostomia due to the current lack of relevant randomized clinical trials.64–67
When stimulation of salivary secretion fails, patients can be given palliative oral care in the form of application of mouthwashes and saliva substitutes. Although the daily use of a mouthwash or one of the saliva substitutes that are formulated to mimic natural saliva, is strongly recommended, they do not stimulate salivary gland production. Commercially available products come in a variety of formulations including solutions, sprays, gels, and lozenges. In general, they contain an agent to increase viscosity, such as carboxymethylcellulose or hydroxypropylmethylcellulose, hydroxyethylcellulose, and polyglycerylmethacrylate,65 minerals such as calcium and phosphate ions and fluoride, preservatives such as methyl or propylparaben, and flavoring and related agents.
Also homeopathic remedies such as olive oil, aloe vera gel, and rape oil spray may be effective alternatives in the palliative management of xerostomic patients.68,69
In order to minimize problems related to the absence of or reduced secretion of saliva, all patients should be encouraged to take an active role in the management of their xerostomia; so a daily mouth examination, checking for red, white, or dark patches, ulcers, or tooth decay, is highly recommended.
Patients with reduced saliva should also be encouraged to consider visiting their dentist more frequently because they have got a greater susceptibility to dental problems. Teeth should be cleaned at least twice a day, so brushing and flossing regularly and the daily use of fluoride and chlorhexidine rinses may also be useful in preventing caries by reducing amounts of Streptococcus and Lactobacillus in the mouth. For daily use, a special dentifrice (eg, children’s toothpaste or anti-xerostomia dentifrices) is recommended, since the taste of a regular dentifrice may be too strong for these patients.
Dentures and acrylic appliances should not be worn during sleep and they should be kept clean by soaking them overnight in chlorhexidine. Sometimes, lubricants, Vaseline and/or glycerin based, put on the lips and under dentures, may relieve drying, cracking, soreness, and mucosal trauma.61
Patients with decreased salivary flow should also be made aware of the necessity to comply with suggested oral hygiene regimens after exposure to acid-producing food sources. Recommendations for professional and home fluoride treatments should be considered carefully for patients with salivary dysfunction, especially those with high caries rates and exposed root surfaces. A modified diet can be useful to minimize the effects of xerostomia; for instance, they should avoid sugary or acidic foods and also avoid dry, spicy, astringent, or excessively hot or cold foods that are more irritating, while eating foods such as carrots or celery may also help patients with residual salivary gland function. The addition of flavor enhancers such as herbs, condiments, and fruit extracts may make food more palatable to patients complaining of their food tasting bland, papery, salty, or otherwise unpleasant; at the same time, taking frequent sips of water throughout the day and sucking on ice chips are helpful.70
Conclusion
The resulting salivary gland hypofunction and xerostomia arising from radiotherapy for HNC can cause a serious diseased condition. The stomatologic complications could depend on the type of cancer treatment and the cumulative radiation dose to the gland tissue. They can be reversible or irreversible, transient, or enduring. The best approach to manage the radiotherapeutic patient begins with a careful clinical assessment of the individual case, followed by preventive therapy aimed to reduce oral complications when possible. Therefore, the clinician must keep this kind of patients under careful control in order to palliate the symptoms of xerostomia and improve their quality of life.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Bivona PL. Xerostomia. A common problem among the elderly. N Y State Dent J. 1998;64:46–52. [PubMed] [Google Scholar]
- 2.Cassolato SF, Turnbull RS. Xerostomia: clinical aspects and treatment. Gerodontology. 2003;20:64–77. doi: 10.1111/j.1741-2358.2003.00064.x. [DOI] [PubMed] [Google Scholar]
- 3.Waltimo T, Christen S, Meurman JH, Filippi A. Dental care of patients with leukemia. Schweiz Monatsschr Zahnmed. 2005;115:308–315. [PubMed] [Google Scholar]
- 4.Brand HS, Bots CP, Raber-Durlacher E. Xerostomia and chronic oral complications among patients treated with haematopoietic stem cell transplantation. Br Dent J. 2009;207:E17. doi: 10.1038/sj.bdj.2009.977. [DOI] [PubMed] [Google Scholar]
- 5.Gupta A, Epstein JB, Sroussi H. Hyposalivation in elderly patients. J Can Dent Assoc. 2006;72:841–846. [PubMed] [Google Scholar]
- 6.Villa A, Abati S. Risk factors and symptoms associated with xerostomia: a cross-sectional study. Aust Dent J. 2011;56:290–295. doi: 10.1111/j.1834-7819.2011.01347.x. [DOI] [PubMed] [Google Scholar]
- 7.Villa A, Polimeni A, Strohmenger L, Cicciù D, Gherlone E, Abati S. Dental patients’ self-reports of xerostomia and associated risk factors. J Am Dent Assoc. 2011;142:811–816. doi: 10.14219/jada.archive.2011.0269. [DOI] [PubMed] [Google Scholar]
- 8.Busato IM, Ignácio SA, Brancher JA, Grégio AM, Machado MA, Azevedo-Alanis LR. Impact of xerostomia on the quality of life of adolescents with type 1 diabetes mellitus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:376–382. doi: 10.1016/j.tripleo.2009.05.005. [DOI] [PubMed] [Google Scholar]
- 9.Moore P, Guggenheimer J, Etzel JK, Weyant RJ. Trevor orchard type 1 diabetes mellitus, xerostomia, and salivary flow rates. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:281–291. doi: 10.1067/moe.2001.117815. [DOI] [PubMed] [Google Scholar]
- 10.Jensen SB, Pedersen AM, Vissink A, et al. Salivary Gland Hypofunction/Xerostomia Section, Oral Care Study Group, Multinational Association of Supportive Care in Cancer (MASCC)/International Society of Oral Oncology (ISOO) A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: prevalence, severity and impact on quality of life. Support Care Cancer. 2010;18:1039–1060. doi: 10.1007/s00520-010-0827-8. [DOI] [PubMed] [Google Scholar]
- 11.Fox PC, Bunch KA, Baum BJ. Subjective reports of xerostomia and objective measures of salivary gland performance. J Am Dent Assoc. 1987;115:581–584. doi: 10.1016/s0002-8177(87)54012-0. [DOI] [PubMed] [Google Scholar]
- 12.Porter SR, Scully C, Hegarty AM. An update of the etiology and management of xerostomia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;97:28–46. doi: 10.1016/j.tripleo.2003.07.010. [DOI] [PubMed] [Google Scholar]
- 13.De Graeff A, De Leeuw JR, Ros WJ, Hordijk GJ, Blijham GH, Winnubst JA. A prospective study on quality of life of patients with cancer of the oral cavity or oropharynx treated with surgery with or without radiotherapy. Oral Oncol. 1999;35:27–32. doi: 10.1016/s1368-8375(98)00049-9. [DOI] [PubMed] [Google Scholar]
- 14.Argiris A, Karamouzis MV, Raben D, Ferris RL. Head and neck cancer. Lancet. 2008;371:1695–1709. doi: 10.1016/S0140-6736(08)60728-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Globocaniarcfr [homepage on the Internet] Lyon. International Agency for Research on Cancer; World Health Organization; 2012. [Accessed May 1, 2014]. [updated January 9, 2014]. Available from: http://globocan.iarc.fr/Default.aspx. [Google Scholar]
- 16.Maciejewski B, Zajusz A, Pilecki B, et al. Salivary Gland Hypofunction/Xerostomia Section, Oral Care Study Group, Multinational Association of Supportive Care in Cancer (MASCC)/International Society of Oral Oncology (ISOO) Acute mucositis in the stimulated oral mucosa of patients during radiotherapy for head and neck cancer. Radiother Oncol. 1991;22:7–11. doi: 10.1016/0167-8140(91)90063-m. [DOI] [PubMed] [Google Scholar]
- 17.Scully C, Epstein JB. Oral health care for the cancer patient. Eur J Cancer B Oral Oncol. 1996;32:281–292. doi: 10.1016/0964-1955(96)00037-1. [DOI] [PubMed] [Google Scholar]
- 18.Sreebny LM. Saliva in health and disease: an appraisal and update. Int Dent J. 2000;50:140–161. doi: 10.1111/j.1875-595x.2000.tb00554.x. [DOI] [PubMed] [Google Scholar]
- 19.Vissink A, Kalicharan D, S-Gravenmade EJ, et al. Acute irradiation effects on morphology and function of rat submandibular glands. J Oral Pathol Med. 1991;20:449–456. doi: 10.1111/j.1600-0714.1991.tb00437.x. [DOI] [PubMed] [Google Scholar]
- 20.Burlage FR, Coppes RP, Meertens H, Stokman MA, Vissink A. Parotid and submandibular/sublingual flow during high dose radiotherapy. Radiother Oncol. 2001;61:271–274. doi: 10.1016/s0167-8140(01)00427-3. [DOI] [PubMed] [Google Scholar]
- 21.Epstein JB, Robertson M, Emerton S, Phillips N, Stevenson-Moore P. Quality of life and oral function in patients treated with radiation therapy for head and neck cancer. Head Neck. 2001;23:389–398. doi: 10.1002/hed.1049. [DOI] [PubMed] [Google Scholar]
- 22.Franzén L, Funegård U, Ericson T, Henriksson R. Parotid gland function during and following radiotherapy of malignancies in the head and neck. A consecutive study of salivary flow and patient discomfort. Eur J Cancer. 1992;28:457–462. doi: 10.1016/s0959-8049(05)80076-0. [DOI] [PubMed] [Google Scholar]
- 23.Dreizen SA, Daly TE, Drane JB, Brown LR. Oral complications of cancer radiotherapy. Postgrad Med. 1977;61:85–92. doi: 10.1080/00325481.1977.11712115. [DOI] [PubMed] [Google Scholar]
- 24.Ben-Aryeh H, Gutman D, Szargel R, Laufer D. Effects of irradiation on saliva in cancer patients. Int J Oral Surg. 1975;14:205–210. doi: 10.1016/s0300-9785(75)80027-5. [DOI] [PubMed] [Google Scholar]
- 25.Dreizen S, Brown LR, Handler S, Levy BM. Radiation-induced xerostomia in cancer patients. Effect on salivary and serum electrolytes. Cancer. 1976;38:273–278. doi: 10.1002/1097-0142(197607)38:1<273::aid-cncr2820380141>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]
- 26.Marks JE, Davis CC, Gottsman VL, Purdy JE, Lee F. The effects of radiation of parotid salivary function. Int J Radiat Oncol Biol Phys. 1981;7:1013–1019. doi: 10.1016/0360-3016(81)90152-8. [DOI] [PubMed] [Google Scholar]
- 27.Ben-Aryeh H, Miron D, Berdicevsky I, Szargel R, Gutman D. Xerostomia in the elderly: prevalence, diagnosis, complications and treatment. Gerodontology. 1985;4:77–82. doi: 10.1111/j.1741-2358.1985.tb00373.x. [DOI] [PubMed] [Google Scholar]
- 28.Abelson DC, Mandel ID. The effect of saliva on plaque pH in vivo. J Dent Res. 1981;60:1634–1638. doi: 10.1177/00220345810600090101. [DOI] [PubMed] [Google Scholar]
- 29.Lingström P, Birkhed D. Plaque pH and oral retention after consumption of starchy snack products at normal and low salivary secretion rate. Acta Odontol Scand. 1993;51:379–388. doi: 10.3109/00016359309040589. [DOI] [PubMed] [Google Scholar]
- 30.Eliasson L, Birkhed D, Osterberg T, Carlén A. Minor salivary gland secretion rates and immunoglobulin A in adults and the elderly. Eur J Oral Sci. 2006;114:494–499. doi: 10.1111/j.1600-0722.2006.00413.x. [DOI] [PubMed] [Google Scholar]
- 31.Almståhl A, Wikström M. Oral microflora in subjects with reduced salivary secretion. J Dent Res. 1998;78:1410–1416. doi: 10.1177/00220345990780080601. [DOI] [PubMed] [Google Scholar]
- 32.Valdez IH, Wolff A, Atkinson JC, Macynski AA, Fox PC. Use of pilocarpine during head and neck radiation therapy to reduce xerostomia and salivary dysfunction. Cancer. 1993;71:1848–1851. doi: 10.1002/1097-0142(19930301)71:5<1848::aid-cncr2820710522>3.0.co;2-f. [DOI] [PubMed] [Google Scholar]
- 33.Makkonen TA, Tenovuo J, Vilja P, Heimdahl A. Changes in the protein composition of whole saliva during radiotherapy in patients with oral or pharyngeal cancer. Oral Surg Oral Med Oral Pathol. 1986;62:270–275. doi: 10.1016/0030-4220(86)90007-1. [DOI] [PubMed] [Google Scholar]
- 34.Izutsu KT, Truelove EL, Bleyer WA, Anderson WM, Schubert MM, Rice JC. Whole saliva albumin as an indicator of stomatitis in cancer therapy patients. Cancer. 1981;48(6):1450–1454. doi: 10.1002/1097-0142(19810915)48:6<1450::aid-cncr2820480629>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 35.Brown LR, Dreizen S, Handler S, Johnston DA. Effect of radiation-induced xerostomia on human oral microflora. J Dent Res. 1974;54(4):740–750. doi: 10.1177/00220345750540040801. [DOI] [PubMed] [Google Scholar]
- 36.Keene HJ, Daly T, Brown LR, et al. Dental caries and Streptococcus mutans prevalence in cancer patients with irradiation-induced xerostomia: 1–13 years after radiotherapy. Caries Res. 1981;15:416–427. doi: 10.1159/000260547. [DOI] [PubMed] [Google Scholar]
- 37.Hase JC, Birkhed D. Salivary glucose clearance, dry mouth and pH changes in dental plaque in man. Arch Oral Biol. 1988;33:875–880. doi: 10.1016/0003-9969(88)90016-7. [DOI] [PubMed] [Google Scholar]
- 38.Ravald N, List T. Caries and periodontal conditions in patients with primary Sjögren’s syndrome. Swed Dent J. 1998;22(3):97–103. [PubMed] [Google Scholar]
- 39.Almståhl A, Wikström M, Groenink J. Lactoferrin, amylase and mucin MUC5B and their relation to the oral microflora in hyposalivation of different origins. Oral Microbiol Immunol. 2001;16:345–352. doi: 10.1034/j.1399-302x.2001.160605.x. [DOI] [PubMed] [Google Scholar]
- 40.Almståhl A, Carlén A, Eliasson L, Lingström P. Lactobacillus species in supragingival plaque in subjects with hyposalivation. Arch Oral Biol. 2010;55:255–259. doi: 10.1016/j.archoralbio.2010.01.007. [DOI] [PubMed] [Google Scholar]
- 41.Radvansky LJ, Pace MB, Siddiqui A. Prevention and management of radiation-induced dermatitis, mucositis, and xerostomia. Am J Health Syst Pharm. 2013;70:1025–1032. doi: 10.2146/ajhp120467. [DOI] [PubMed] [Google Scholar]
- 42.Wijers OB, Levendag PC, Braaksma MM, Boonzaaijer M, Visch LL, Schmitz PI. Patients with head and neck cancer cured by radiation therapy: a survey of the dry mouth syndrome in long-term survivors. Head Neck. 2002;24:737–747. doi: 10.1002/hed.10129. [DOI] [PubMed] [Google Scholar]
- 43.Sher DJ, Balboni TA, Haddad RI, et al. Efficacy and toxicity of chemoradiotherapy using intensity-modulated radiotherapy for unknown primary of head and neck. Int J Radiat Oncol Biol Phys. 2011;80:1405–1411. doi: 10.1016/j.ijrobp.2010.04.029. [DOI] [PubMed] [Google Scholar]
- 44.Schoenfeld JD, Sher DJ, Norris CM, Jr, et al. Salivary gland tumors treated with adjuvant intensity-modulated radiotherapy with or without concurrent chemotherapy. Int J Radiat Oncol Biol Phys. 2012;82:308–314. doi: 10.1016/j.ijrobp.2010.09.042. [DOI] [PubMed] [Google Scholar]
- 45.Atkinson JC, Wu AJ. Salivary gland dysfunction: causes, symptoms, treatment. J Am Dent Assoc. 1994;125:409–416. doi: 10.14219/jada.archive.1994.0059. [DOI] [PubMed] [Google Scholar]
- 46.Spielman AI. Gustducin and its role in taste. J Dent Res. 1998;77:539–544. doi: 10.1177/00220345980770040601. [DOI] [PubMed] [Google Scholar]
- 47.Pedersen AM, Bardow A, Jensen SB, Nauntofte B. Saliva and gastrointestinal functions of taste, mastication, swallowing and digestion. Oral Dis. 2002;8:117–129. doi: 10.1034/j.1601-0825.2002.02851.x. [DOI] [PubMed] [Google Scholar]
- 48.Ramirez-Amador V, Silverman S, Jr, Mayer P, Tyler M, Quivey J. Candidal colonization and oral candidiasis in patients undergoing oral and pharyngeal radiation therapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:149–153. doi: 10.1016/s1079-2104(97)90061-5. [DOI] [PubMed] [Google Scholar]
- 49.Chen TY, Webster JH. Oral monilia study on patients with head and neck cancer during radiotherapy. Cancer. 1974;34:246–249. doi: 10.1002/1097-0142(197408)34:2<246::aid-cncr2820340203>3.0.co;2-j. [DOI] [PubMed] [Google Scholar]
- 50.Samaranayake LP, Lamey PJ. Oral candidosis: 1. clinicopathological aspects. Dent Update. 1988;15(6):227–228. 230–231. [PubMed] [Google Scholar]
- 51.Kuntz R, Allen M, Osburn J. Xerostomia. Int J Pharm Compd. 2000;4:1176–1177. [PubMed] [Google Scholar]
- 52.Almeida JP, Kowalski LP. Pilocarpine used to treat xerostomia in patients submitted to radioactive iodine therapy: a pilot study. Braz J Otorhinolaryngol. 2010;76(5):659–662. doi: 10.1590/S1808-86942010000500021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Koseki M, Maki Y, Matsukubo T, Ohashi Y, Tsubota K. Salivary flow and its relationship to oral signs and symptoms in patients with dry eyes. Oral Dis. 2004;10(2):75–80. doi: 10.1111/j.1354-523x.2003.00987.x. [DOI] [PubMed] [Google Scholar]
- 54.Tomiita M, Takei S, Kuwada N, et al. Efficacy and safety of orally administered pilocarpine hydrochloride for patients with juvenile-onset Sjögren’s syndrome. Mod Rheumatol. 2010;20(5):486–490. doi: 10.1007/s10165-010-0313-7. [DOI] [PubMed] [Google Scholar]
- 55.Ramos-Casals M, Tzioufas AG, Stone JH, Sisó A, Bosch X. Treatment of primary Sjögren syndrome: a systematic review. JAMA. 2010;304(4):452–460. doi: 10.1001/jama.2010.1014. [DOI] [PubMed] [Google Scholar]
- 56.Hendrickson RG, Morocco AP, Greenberg MI. Pilocarpine toxicity and the treatment of xerostomia. J Emerg Med. 2004;26(4):429–432. doi: 10.1016/j.jemermed.2003.09.013. [DOI] [PubMed] [Google Scholar]
- 57.Chambers MS, Jones CU, Biel MA, et al. Open-label, long-term safety study of cevimeline in the treatment of postirradiation xerostomia. Int J Radiat Oncol Biol Phys. 2007;69(5):1369–1376. doi: 10.1016/j.ijrobp.2007.05.024. [DOI] [PubMed] [Google Scholar]
- 58.Chambers MS, Posner M, Jones CU, et al. Cevimeline for the treatment of postirradiation xerostomia in patients with head and neck cancer. Int J Radiat Oncol Biol Phys. 2007;68(4):1102–1109. doi: 10.1016/j.ijrobp.2007.01.019. [DOI] [PubMed] [Google Scholar]
- 59.Hamada T, Nakane T, Kimura T, et al. Treatment of xerostomia with the bile secretion-stimulant drug anethole trithione: a clinical trial. Am J Med Sci. 1999;318:146–151. doi: 10.1097/00000441-199909000-00009. [DOI] [PubMed] [Google Scholar]
- 60.Bagheri H, Schmitt L, Berlan M, Montastruc JL. A comparative study of the effects of yohimbine and anetholtrithione on salivary secretion in depressed patients treated with psychotropic drugs. Eur J Clin Pharmacol. 1997;52:339–342. doi: 10.1007/s002280050298. [DOI] [PubMed] [Google Scholar]
- 61.Dyke S. Clinical management and review of Sjögren’s syndrome. Int J Pharm Compd. 2000;4:338–341. [PubMed] [Google Scholar]
- 62.Johnstone PA, Peng YP, May BC, Inouye WS, Niemtzow RC. Acupuncture for pilocarpine-resistant xerostomia following radiotherapy for head and neck malignancies. Int J Radiat Oncol Biol Phys. 2001;50:353–357. doi: 10.1016/s0360-3016(00)01530-3. [DOI] [PubMed] [Google Scholar]
- 63.Sagar SM. Acupuncture as an evidence-based option for symptom control in cancer patients. Curr Treat Options Oncol. 2008;9:117–126. doi: 10.1007/s11864-008-0063-3. [DOI] [PubMed] [Google Scholar]
- 64.Jedel E. Acupuncture in xerostomia – a systematic review. J Oral Rehabil. 2005;32:392–396. doi: 10.1111/j.1365-2842.2005.01445.x. [DOI] [PubMed] [Google Scholar]
- 65.Jensen SB, Pedersen AM, Vissink A, et al. A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: management strategies and economic impact. Support Care Cancer. 2010;18(8):1061–1079. doi: 10.1007/s00520-010-0837-6. [DOI] [PubMed] [Google Scholar]
- 66.O’Sullivan EM, Higginson IJ. Clinical effectiveness and safety of acupuncture in the treatment of irradiation-induced xerostomia in patients with head and neck cancer: a systematic review. Acupunct Med. 2010;28:191–199. doi: 10.1136/aim.2010.002733. [DOI] [PubMed] [Google Scholar]
- 67.Zhuang L, Yang Z, Zeng X, et al. The preventive and therapeutic effect of acupuncture for radiation-induced xerostomia in patients with head and neck cancer: a systematic review. Integr Cancer Ther. 2013;12:197–205. doi: 10.1177/1534735412451321. [DOI] [PubMed] [Google Scholar]
- 68.Diaz-Arnold AM, Marek CA. The impact of saliva on patient care: a literature review. J Prosthet Dent. 2002;88:337–343. doi: 10.1067/mpr.2002.128176. [DOI] [PubMed] [Google Scholar]
- 69.Momm F, Volegova-Neher NJ, Schulte-Monting J, Guttenberger R. Different saliva substitutes for treatment of xerostomia following radiotherapy. A prospective crossover study. Strahlenther Onkol. 2005;181:231–236. doi: 10.1007/s00066-005-1333-7. [DOI] [PubMed] [Google Scholar]
- 70.Davies A. Clinically proved treatments for xerostomia were ignored. BMJ. 1998;316:1247. [PubMed] [Google Scholar]