

Abstract
Study Design
Retrospective cohort study.
Objective
In older adults with a neuromusculoskeletal complaint, to evaluate risk of injury to the head, neck or trunk following an office visit for chiropractic spinal manipulation, as compared to office visit for evaluation by primary care physician.
Summary of Background Data
The risk of physical injury due to spinal manipulation has not been rigorously evaluated for older adults, a population particularly vulnerable to traumatic injury in general.
Methods
We analyzed Medicare administrative data on Medicare B beneficiaries aged 66–99 with an office visit in 2007 for a neuromusculoskeletal complaint. Using a Cox proportional hazards model, we evaluated for adjusted risk of injury within 7 days, comparing two cohorts: those treated by chiropractic spinal manipulation vs. those evaluated by a primary care physician. We used direct adjusted survival curves to estimate the cumulative probability of injury. In the chiropractic cohort only, we used logistic regression to evaluate the effect of specific chronic conditions on likelihood of injury.
Results
The adjusted risk of injury in the chiropractic cohort was lower as compared to the primary care cohort (hazard ratio 0.24; 95% CI 0.23–0.25). The cumulative probability of injury in the chiropractic cohort was 40 injury incidents per 100,000 subjects, as compared to 153 incidents per 100,000 subjects in the primary care cohort. Among subjects who saw a chiropractic physician, the likelihood of injury was increased in those with a chronic coagulation defect, inflammatory spondylopathy, osteoporosis, aortic aneurysm and dissection, or long-term use of anticoagulant therapy.
Conclusions
Among Medicare beneficiaries aged 66–99 with an office visit risk for a neuromusculoskeletal problem, risk of injury to the head, neck or trunk within 7 days was 76% lower among subjects with a chiropractic office visit as compared to those who saw a primary care physician.
Keywords: Epidemiology, Health Services Research, conservative care, Trauma, Non-Operative Treatment, Manipulation
Introduction
Spinal Manipulation (SM) as performed by chiropractors is an effective option for the treatment of certain types of spinal pain and some headaches.1–4 Because SM involves the application of physical force, there is a potential risk of traumatic injury, should the manipulation be lacking in technical skill or precision, provided to individuals particularly vulnerable to injury, or otherwise misapplied. However, the risk of injury to the head, neck or trunk following SM remains uncertain, particularly for older adults.
A 2012 Cochrane review found that many clinical trials of SM either did not report adverse effects, or were of insufficient power or duration to assess the risk of serious adverse effects.5 A recent trial designed to evaluate the frequency of adverse effects of chiropractic treatment reported no serious events.6 Prospective studies have found that adverse effects associated with chiropractic care and SM are common but tend to be mild, transient and benign.7–12 In 2007 two prospective studies on the safety of cervical SM found no serious adverse events.13,14 Survey studies have identified complications of SM that required medical intervention,15 but the survey instruments tended to suffer from methodological flaws.16
Injuries associated with SM have been reported primarily in the form of case reports and case series studies, and many such incidents have been subsequently analyzed in systematic reviews. In a 2002 systematic review, Ernst estimated the risk of serious adverse events to be between 1 in 400,000 and 1 in 2,000,000 manipulations.17 In a second systematic review in 2007, the same investigator found insufficient evidence to quantify the incidence of serious adverse events associated with SM, but concluded that SM can cause serious complications.8 In 2012 however, a replication of Ernst’s 2007 review found numerous errors and omissions that threatened its validity.18 A 2010 systematic review was unable to draw any conclusions regarding the safety of cervical SM due to a paucity of data and risks of study bias.19 In 2013 an updated Cochrane review of 20 randomized clinical trials found no serious complications associated with SM for acute low back pain.3 Gouveia and colleagues’ 2009 systematic review found that the frequency of serious adverse events associated with chiropractic care varied from .05 to 1.46 per 10,000,000 manipulations, but that a lack of robust data compels the need for further investigation.9
No mechanism by which SM induces injury in normal healthy tissues has been identified,20,21,22 but the likelihood of injury due to manipulation may be elevated in pathologically weakened tissues. An analysis of 140 cases of adverse effects of SM identified coagulation disorder or herniated nucleus pulposus as possible risk factors.23 The Centers for Medicare and Medicaid Services (CMS) have identified certain conditions as contraindications to SM,24 but there is insufficient empirical evidence to positively identify many of these conditions as risk factors for injury due to SM.
A 2007 systematic review of serious injuries associated with SM found cases of cervical artery dissection, dural tear, nerve injury, disc herniation, hematoma, fracture, cord injury and nerve root injury.8 A 2009 systematic review of the safety of chiropractic care found reports of arterial dissection, myelopathy, vertebral disc extrusion, and epidural hematoma. A 2013 systematic review of serious adverse events following SM found cases of cauda equina syndrome (38%); lumbar disk herniation (30%); fracture (9%); and formation of hematoma or hemorrhagic cyst (8%).25 A 2012 literature review of accidents associated with cervical SM over a 32 year period in China found cases of cord injury or compression, nerve root injury, cervical spine dislocation, and soft tissue injury.26 This report may have overestimated the risks of SM performed by a licensed chiropractor however, because the practice of chiropractic in China is unrecognized and unregulated.
The benefits of chiropractic care in general appear to outweigh the risks.27 However for older adults – a population particularly vulnerable to traumatic injury and its sequelae – the safety of SM has not been rigorously evaluated and the risk of physical injury due to SM remains unknown. In this study we analyzed Medicare claims to evaluate for risk of injury to the head, neck or trunk in older adults. We also examined the association between such injuries and chronic conditions identified by CMS as contraindications to SM. This is the first nationwide population-based study in the US on risk of injury following SM, and the first study of the risks of chiropractic to focus specifically on older adults.
Materials and Methods
We conducted a retrospective cohort study using Medicare administrative data. Our data sources were 100% of Denominator files (for beneficiary demographics), Carrier files (for outpatient claims), and Medicare Provider Analysis and Review (MEDPAR) files (for inpatient claims), as well as Medicare Physician Identification and Eligibility Records (MPIER) files for physician data, for the years 2006–2008. The data files were merged on unique beneficiary identifiers to generate the analytic file. The data were analyzed in accordance with a data user agreement with CMS, and the principal investigator’s institutional review board approved the research plan.
We included all beneficiaries covered under the Medicare B fee for service plan, aged 66–99 and living as of Jan 1st of each year, with at least one allowed Medicare B claim in 2007 for an office visit to either a chiropractor or primary care physician, with an associated ICD-9 diagnosis code for a neuromusculoskeletal (NMS) problem. We defined an NMS problem as any diagnosis that was designated as appropriate for chiropractic care, as determined by CMS. [Appendix] Each included subject was assigned to one of two cohorts, in which subjects used either only chiropractic or only primary care office visits for evaluation and/or care of NMS complaints.
Chiropractic Cohort: Beneficiaries with at least one allowed Medicare B claim in 2007 for chiropractic office visit with SM (CPT code 98940, 98941 or 98942), and with the provider specialty code for chiropractic physicians (35).
Primary Care Cohort: Beneficiaries with at least one allowed Medicare B claim in 2007 for office visit for evaluation and management associated with the provider specialty code for Family Medicine (08), Internal Medicine (11) or General Practice (01). Evaluation and management services were identified by Betos code “M”.
We excluded duplicate claims for the same patient, provider, procedure and date of service. A one year look-back period [Figure 1] served to exclude subjects with a history or concomitant diagnosis at the index office visit of injury to head, neck or trunk. We reasoned that patients diagnosed with injury at the time of the office visit were likely to have sustained the injury before seeing the doctor, in which case the injury could not have been caused by the office visit. We made an exception to these exclusions: we did not exclude subjects with a chiropractic office visit and associated ICD-9 code within the range 839.0 – 839.59. Although medical physicians use this code series to denote traumatic vertebral dislocation (a contraindication to manipulation), chiropractors frequently use these codes to denote a manipulable vertebral subluxation. The one-year look back window also served to identify subjects with chronic conditions that have been identified by CMS as contraindications for SM, [Table 1] and to identify comorbidities for the purpose of calculating Charlson co-morbidity scores for risk adjustment.28 Identification of such chronic conditions required at least two claims more than 7 days apart that documented the same diagnosis.
Figure 1.
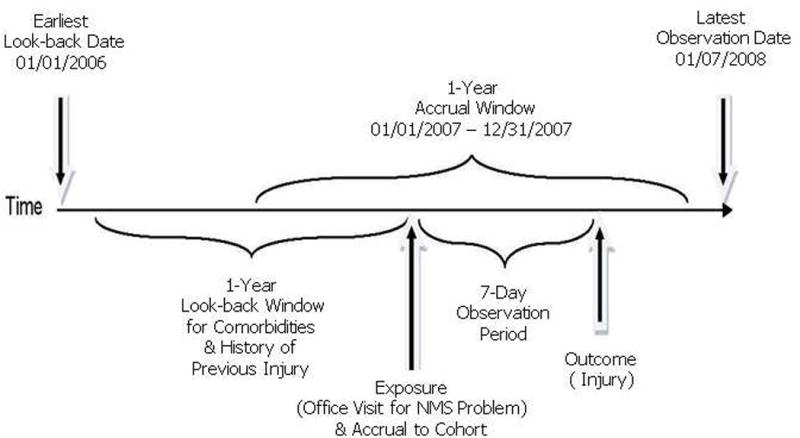
Cohort Accrual
Table 1.
Subject Characteristics
| Cohort | Primary Care | Chiropractic |
|---|---|---|
| Subjects | 5,669,032 | 1,000,571 |
|
| ||
| Age Category in Years (%) | ||
| 66–69 | 18.71 | 28.12 |
| 70–74 | 22.48 | 29.21 |
| 75–79 | 22.11 | 22.03 |
| 80–84 | 18.91 | 13.31 |
| 85–99 | 17.79 | 7.34 |
|
| ||
| Gender (%) | ||
| Female | 67.24 | 55.00 |
| Male | 32.76 | 45.00 |
|
| ||
| Race (%) | ||
| White | 87.62 | 97.07 |
| Black | 7.36 | 1.32 |
| Other Race | 5.02 | 1.61 |
|
| ||
| Charlson Co-morbidity Score | 1.56 | 1.00 |
|
| ||
| Chronic Condition – Identified as Contraindication to Spinal Manipulation (%) | ||
| Bone Neoplasm – head, spine, pelvis or rib cage (ICD-9 170.0, 170.2–3, 170.6, 213, 213.2–3 & 213.6) |
0.03 | 0.02 |
| Coagulation defect (ICD-9 286–286.9) |
0.6 | 0.34 |
| Occlusion and stenosis of precerebral artery (ICD-9 433–433.91) |
1.89 | 1.72 |
| Inflammatory spondylopathy (ICD-9 720–720.9) |
0.54 | 0.33 |
| Osteoporosis (ICD-9 733–733.19) |
4.13 | 2.42 |
| Myelopathy (ICD-9 336–336.9 |
0.08 | 0.03 |
| Intervertebral disc disorder with myelopathy (ICD-9 722.7–722.73) |
0.28 | 0.15 |
| Aortic aneurysm and dissection (ICD-9 441–441.9) |
0.81 | 0.77 |
| Cauda equina syndrome (ICD-9 344.6–344.61) |
0.06 | 0.04 |
| Long-term use of anticoagulant therapy (ICD-9 V58.61) |
1.32 | 1.08 |
= statistically significant association (p<.05)
The hazard (observation) period for identifying outcomes was a 7 day window following each exposure to office visit for an NMS problem. The primary outcome measure was diagnosis of injury to head, neck or trunk within 7 days of office visit, diagnosed in an emergency department or as the primary diagnosis associated with a hospital admission. We identified injury outcomes by the following ICD-9 codes, categorized by type of injury: Dislocation/Soft Tissue Injury: 839.0–839.59, 839.61–839.69, 846.0–846.3, 846.8–846.9, 847.0–847.4, 848.5; Fracture: 805.0–806.9, 807–807.1, 808–808.9; Injury to Brain or Spinal Cord: 430, 850–854.1, 952–952.9; Injury to Blood Vessels: 441.1, 441.3, 441.6, 443.21, 443.24, 900–900.9, 901.0, 902.0; Injury to Nerves: 953–953.9, 954.0–954.1, 954.8–954.9, 956.0.
For each office visit, we evaluated the number of days to the diagnosis of injury; censoring occurred at seven days, or at the next visit, or at end of study (Jan 07 2008). Subjects were removed from follow-up upon occurrence of their first injury. Evaluation of risk by office visit allowed comparison of risk between cohorts while allowing for the high degree of variability in number, frequency and timing of office visits. Except for fractures and aortic ruptures (which are more likely to be immediately clinically apparent) we excluded subjects who were diagnosed with a traumatic injury on the same day as the office visit, because these patients may have presented with signs or symptoms of the injury as the reason for the visit.
Using a Cox proportional hazards model, we compared chiropractic visits and primary care visits for hazard of injury within seven days of an office visit. The model was adjusted for subject age, gender, race and Charlson comorbidity index. Based upon a range of chronic conditions, the Charlson comorbidity index assigns a composite score that may be used for risk adjustment for comorbid disease. The model was also adjusted for chronic conditions that have been identified as contraindications for SM and may be risk factors for injury due to SM. To estimate the cumulative probability of injury up to seven days for the chiropractic and primary care groups while adjusting for the covariates stated above, we used direct adjusted survival curves, as described by Zhang and colleagues.22,23 We used logistic regression to evaluate the effect of specific chronic conditions on likelihood of injury in the chiropractic cohort only. We performed data analyses in SAS (SAS Institute Inc., Cary, North Carolina).
Results
Of 23,036,767 Medicare Part B beneficiaries, 7,448,430 had either a primary care or chiropractic office visit for an NMS problem in 2007. [Figure 2] After excluding subjects who saw both types of providers (n=481,968), and those with a recent history of trauma (n=296,859), 6,669,603 subjects remained in the study sample. The primary care cohort (n= 5,669,032) was more than five times as large as the chiropractic cohort (n= 1,000,571), but the number of primary care office visits (13,536,595) only exceeded the number of chiropractic office visits (10,532,213) by 29%.
Figure 2.
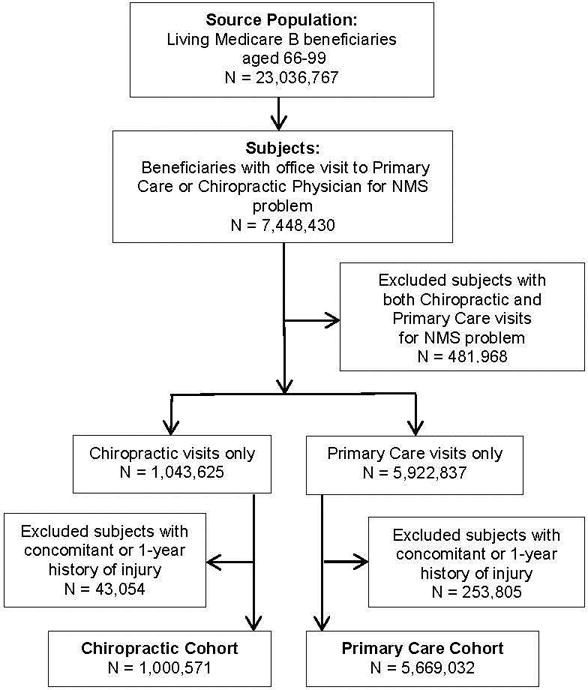
Cohort Selection
The cohorts differed by age, gender, race, co-morbidity score, and chronic conditions. The chiropractic cohort was younger, predominately white and female, healthier as measured by comorbidity score, and contained lower proportions of subjects with chronic conditions. [Table 1] The proportion of subjects in the chiropractic cohort with injuries within seven days of an office visit was 28 per 10,000, as compared to 36 per 10,000 in the primary care cohort. Figure 3 illustrates the adjusted probability of injury for the two cohorts over the 7 day hazard period. The cumulative probability of injury within 7 days was lower in the chiropractic cohort as compared to the primary care cohort (1 vs. 21 injury incidents per 100,000 subjects on Day 0 (day of office visit); 40 vs. 153 injury incidents per 100,000 subjects at Day 7). The unadjusted hazard ratio for risk of injury in the chiropractic cohort as compared to the primary care cohort was 0.19 (95% CI 0.18 – 0.20). With adjustment for differences in patient characteristics, risk of injury in the chiropractic cohort was 76% lower as compared to the primary care cohort (hazard ratio 0.24; 95% CI 0.23–0.25). Male gender, increasing age category, and increased Charlson co-morbidity score were associated with increased risk of injury. [Table 2]
Figure 3.
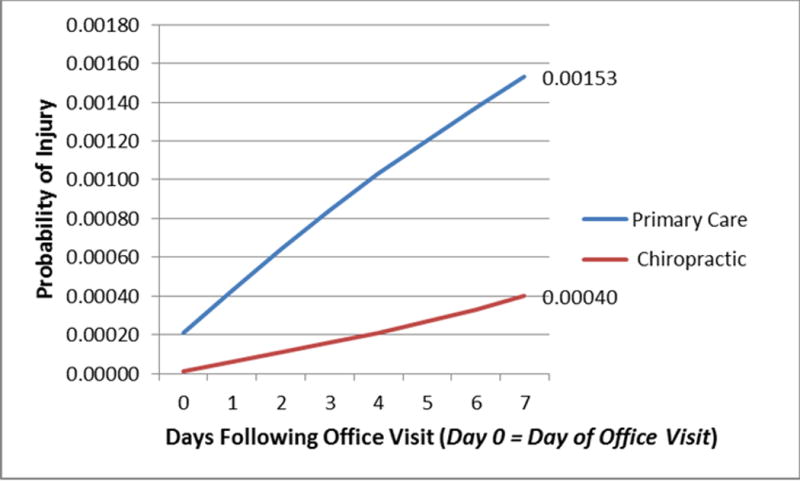
Seven-day Cumulative Probability of Injury Following Office Visit for Neuromusculoskeletal Problem
Table 2.
Risk of Injury within 7 Days of Office Visit
| Hazard Ratio | 95% CI | |
|---|---|---|
| Chiropractic (vs. Primary Care) | 0.24 † | 0.23–0.25 |
|
| ||
| Age Category (vs. 66–69) | ||
| 70–74 | 1.19 † | 1.13–1.26 |
| 75–79 | 1.63 † | 1.55–1.71 |
| 80–84 | 2.15 † | 2.05–2.26 |
| 85–99 | 2.99 † | 2.85–3.13 |
|
| ||
| Male Gender (vs. Female) | 0.9 † | 0.87–0.93 |
|
| ||
| Race (vs. White) | ||
| Black | 0.46 † | 0.43–0.49 |
| Other Race | 0.68 † | 0.64–0.73 |
|
| ||
| Charlson Co-morbidity Score | 1.09 † | 1.09–1.10 |
|
| ||
| Chronic Conditions | ||
| Bone Neoplasm – head, spine, pelvis or ribcage | 2.42 † | 1.58–3.72 |
| Coagulation defect | 1.28 † | 1.13–1.46 |
| Occlusion and stenosis of precerebral artery | 0.98 | 0.90–1.08 |
| Inflammatory spondylopathy | 1.23 † | 1.07–1.41 |
| Osteoporosis | 1.46 † | 1.39–1.54 |
| Myelopathy | 1.39 | 0.98–1.98 |
| Intervertebral disc disorder with myelopathy | 0.82 | 0.64–1.04 |
| Aortic aneurysm and dissection | 1.15 † | 1.01–1.30 |
| Cauda equina syndrome | 1.01 | 0.66–1.53 |
| Long-term use of anticoagulant therapy | 1.31 † | 1.19–1.44 |
= statistically significant association (p<.05)
Among 2,786 injured subjects in the chiropractic cohort, we found 1,059 with dislocation or soft tissue injury, 1,132 with fracture, 562 with brain or spinal cord injury, and 33 with blood vessel injury. We found no nerve injuries in the chiropractic cohort. Table 3 displays odds ratios for diagnosis of any injury and of four categories of injury in patients with specific chronic conditions. Subjects with bony neoplasms of the head, spine, pelvis or rib cage were too few to generate odds ratios. Coagulation defects were associated with elevated likelihood of injury in general (OR 1.87, 95% CI 1.08–3.24). Inflammatory spondylopathy was associated with increased likelihood of dislocation or soft tissue injury (OR 2.59, 95% CI 1.16 – 5.79). Osteoporosis was associated with increased likelihood of injury in general (OR 1.41, 95% CI 1.10–1.80) and for fracture in particular (OR 1.66, 95% CI). Aortic aneurysm & dissection was associated with increased likelihood of injury in general (OR 1.61, 95% CI 1.08–2.41) and specifically for fracture (OR 2.30, 95% CI 1.36–3.91) and injury to blood vessels (OR 23.9, 95% CI 8.23 – 69.45). Long-term use of anticoagulant therapy was associated with increased likelihood of brain or spinal cord injury (OR 2.17, 95% CI 1.15–4.07).
Table 3.
Likelihood of Injury Following Chiropractic Care, by Chronic Condition and Category of Injury
| Any Injury | Dislocation/Soft Tissue Injury | Fracture | Injury to Brain or Spinal Cord | Injury to Blood Vessels | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
| Subjects with Injury | 2,786* | 1,459 | 1,132 | 562 | 33 | |||||
|
| ||||||||||
| Chronic Condition | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI |
| Bone neoplasm of head, spine, Pelvis or rib cage | 0.00 | n/a | 0.00 | n/a | 0.00 | n/a | 0.00 | n/a | 0.00 | n/a |
| Coagulation defect | 1.87 † | 1.08–3.24 | 1.62 | 0.60–4.33 | 1.77 | 0.73–4.28 | 2.63 | 0.98–7.06 | 0.00 | n/a |
| Occlusion and stenosis of precerebral arteries | 0.94 | 0.67–1.34 | 0.91 | 0.50–1.66 | 1.22 | 0.76–1.98 | 0.55 | 0.20–1.46 | 0.00 | n/a |
| Inflammatory spondylopathy | 1.71 | 0.95–3.10 | 2.59 † | 1.16–5.79 | 1.14 | 0.37–3.53 | 1.45 | 0.36–5.83 | 0.00 | n/a |
| Osteoporosis | 1.41 † | 1.10–1.80 | 1.18 | 0.75–1.84 | 1.66 † | 1.16–2.37 | 1.41 | 0.83–2.40 | 0.00 | n/a |
| Myelopathy | 1.58 | 0.22–11.23 | 4.41 | 0.62–31.52 | 0.00 | n/a | 0.00 | n/a | 0.00 | n/a |
| Intervertebral disc disorders with myelopathy | 0.33 | 0.05–2.33 | 0.87 | 0.12–6.22 | 0.00 | n/a | 0.00 | n/a | 0.00 | n/a |
| Aortic aneurysm & dissection | 1.61 † | 1.08–2.41 | 0.37 | 0.09–1.47 | 2.30 † | 1.36–3.91 | 1.26 | 0.47–3.36 | 23.9 † | 8.23–69.45 |
| Cauda Equina Syndrome | 1.41 | 0.20–10.05 | 0.00 | n/a | 3.47 | 0.49–24.73 | 0.00 | n/a | 0.00 | n/a |
| Long-term use of anticoagulant therapy | 1.69 | 0.20–2.36 | 1.57 | 0.89–2.78 | 1.49 | 0.86–2.58 | 2.17 † | 1.15–4.07 | 3.41 | 0.46–25.23 |
Includes subjects with more than one type of injury
= statistically significant elevation in likelihood of injury (p<.05)
Discussion
Our finding of 40 injury incidents per 100,000 subjects at day seven suggests a considerably higher rate of injury than Gouveia and colleagues’ estimate of .05 to 1.46 serious adverse events per 10,000,000 manipulations.9 This is not unexpected because older adults are more vulnerable to injury in general, and indeed we found that within our study population, increased age and comorbidity were associated with higher risk of injury.
It is unlikely that chiropractic care is a significant cause of injury in older adults. The lower risk in the chiropractic cohort may suggest to some that chiropractic care is protective against injury in older adults. However, there is no evidence for such an effect. Given the limitations of observational design, our risk estimates may simply represent background coincidence of injury, without any causal relationship to chiropractic or primary care services. Furthermore, the maximum absolute difference between cohorts in probability of injury (approximately 1 per thousand) is small and of doubtful clinical significance.
Interestingly, although the risk of vertebral artery injury and stroke following SM is controversial and the subject of much investigation, subjects with injury to blood vessels comprised only 1% of subjects with injuries. This finding is consistent with the results of recent research that found a very low incidence of vertebrobasilar stroke among older Medicare beneficiaries.29 Although in the chiropractic cohort the risk of physical injury in patients with occlusion and stenosis of precerebral arteries was reduced, we caution that these conditions – and associated vertebrobasilar insufficiency – are known to be risk factors for vertebrobasilar stroke and therefore contraindicate manipulation of the cervical spine.
In our analysis of selected chronic conditions as potential risk factors for injury following chiropractic care, the prevalence of bone cancer, myelopathy and cauda equina syndrome was too low to generate robust estimates of risk. Myelopathy and cauda equina syndrome have been identified as contraindications to SM under Medicare, but the stronger rationale for contraindication may be the need for medical referral rather than risk of injury due to manipulation. The risk of injury in patients with intervertebral disc disorder with myelopathy was actually reduced, suggesting that this condition is not a risk factor for injury due to chiropractic SM. It is notable that in subjects with a history of aortic aneurysm & dissection, chiropractic SM was associated with increased likelihood of injury in general and strongly associated with increased likelihood of injury to blood vessels. However, we did not specifically evaluate for likelihood of injury in the form of aortic dissection, and the results should not be interpreted as showing an increased risk of aortic dissection. Chiropractic physicians should exercise caution with regard to the provision of SM in older patients with coagulation defects, inflammatory spondylopathy, osteoporosis, aortic aneurysm & dissection, or long term use of anticoagulant therapy.
This study was subject to certain limitations which should be acknowledged. The causal connection between injury and office visit is uncertain due to the inherent limitations of the study design and methods. We did not restrict claims data by E code. E codes are used in claims to identify the circumstance, event, mechanism or agent which caused an injury or adverse effect. Theoretically, the identification of iatrogenic injury could have been facilitated by analysis of E codes. However, E coding is likely inconsistent and was incomplete in our Medicare claims dataset. If complete and accurate E coding had been available, our analysis may have resulted in lower estimates of risk. The actual risk of iatrogenic injury however is unlikely to be higher than the rates reported here. The strong difference in risk between cohorts may have been due at least in part to inadequate control for an older and sicker population in the primary care cohort, and the much larger size of the primary care cohort.
In conclusion, among Medicare beneficiaries aged 66–99 with an office visit risk for a neuromusculoskeletal problem, risk of injury to the head, neck or trunk within seven days was 76% lower among subjects with a chiropractic office visit as compared to those who saw a primary care physician. Among subjects who saw a chiropractor, the likelihood of injury was increased in those with chronic coagulation defect, inflammatory spondylopathy, osteoporosis, aortic aneurysm and dissection, or long term use of anticoagulant therapy.
Supplementary Material
Acknowledgments
NIH and the National Center for Complementary and Alternative Medicine, under Award Number K01AT005092 grant funds were received in support of this work.
Footnotes
The manuscript submitted does not contain information about medical device(s)/drug(s).
Relevant financial activities outside the submitted work: consultancy, stocks.
Contributor Information
James M Whedon, The Dartmouth Institute for Health Policy and Clinical Practice, Lebanon, NH.
Todd A Mackenzie, The Dartmouth Institute for Health Policy and Clinical Practice, Lebanon, NH.
Reed B Phillips, Southern California University of Health Sciences, Whittier, CA.
Jon D Lurie, The Dartmouth Institute for Health Policy and Clinical Practice, Lebanon, NH.
References
- 1.Bronfort G, Nilsson N, Haas M, et al. Non-invasive physical treatments for chronic/recurrent headache. Cochrane Database Syst Rev. 2004;3(3):CD001878. doi: 10.1002/14651858.CD001878.pub2. [DOI] [PubMed] [Google Scholar]
- 2.Gross A, Miller J, D’Sylva J, et al. Manipulation or mobilisation for neck pain. Cochrane Database Syst Rev. 2010;20(1):CD004249. doi: 10.1002/14651858.CD004249.pub3. [DOI] [PubMed] [Google Scholar]
- 3.Rubinstein SM, Terwee CB, Assendelft WJ, de Boer MR, van Tulder MW. Spinal manipulative therapy for acute low back pain: an update of the cochrane review. Spine (Phila Pa 1976) 2013 Feb 1;38(3):E158–177. doi: 10.1097/BRS.0b013e31827dd89d. [DOI] [PubMed] [Google Scholar]
- 4.Rubinstein SM, van Middelkoop M, Assendelft WJ, de Boer MR, van Tulder MW. Spinal manipulative therapy for chronic low-back pain. Cochrane Database Syst Rev. 2011;(2):CD008112. doi: 10.1002/14651858.CD008112.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rubinstein SM, Terwee CB, Assendelft WJ, de Boer MR, van Tulder MW. Spinal manipulative therapy for acute low-back pain. Cochrane Database Syst Rev. 2012;(9):CD008880. doi: 10.1002/14651858.CD008880.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Walker BF, Hebert JJ, Stomski NJ, et al. Outcomes of usual chiropractic. The OUCH randomized controlled trial of adverse events. Spine (Phila Pa 1976) 2013 Sep 15;38(20):1723–1729. doi: 10.1097/BRS.0b013e31829fefe4. [DOI] [PubMed] [Google Scholar]
- 7.Cagnie B, Vinck E, Beernaert A, Cambier D. How common are side effects of SMand can these side effects be predicted? Man Ther Aug. 2004;9(3):151–156. doi: 10.1016/j.math.2004.03.001. [DOI] [PubMed] [Google Scholar]
- 8.Ernst E. Adverse effects of spinal manipulation: a systematic review. J R Soc Med Jul. 2007;100(7):330–338. doi: 10.1258/jrsm.100.7.330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gouveia LO, Castanho P, Ferreira JJ. Safety of chiropractic interventions: a systematic review. Spine (Phila Pa 1976) 2009 May 15;34(11):E405–413. doi: 10.1097/BRS.0b013e3181a16d63. [DOI] [PubMed] [Google Scholar]
- 10.Leboeuf-Yde C, Hennius B, Rudberg E, Leufvenmark P, Thunman M. Side effects of chiropractic treatment: a prospective study. J Manipulative Physiol Ther. 1997 Oct;20(8):511–515. [PubMed] [Google Scholar]
- 11.Senstad O, Leboeuf-Yde C, Borchgrevink C. Predictors of side effects to spinal manipulative therapy. J Manipulative Physiol Ther. 1996 Sep;19(7):441–445. [PubMed] [Google Scholar]
- 12.Senstad O, Leboeuf-Yde C, Borchgrevink C. Frequency and characteristics of side effects of spinal manipulative therapy. Spine (Phila Pa 1976) 1997 Feb 15;22(4):435–440. doi: 10.1097/00007632-199702150-00017. discussion 440–431. [DOI] [PubMed] [Google Scholar]
- 13.Rubinstein SM, Leboeuf-Yde C, Knol DL, de Koekkoek TE, Pfeifle CE, van Tulder MW. The benefits outweigh the risks for patients undergoing chiropractic care for neck pain: a prospective, multicenter, cohort study. J Manipulative Physiol Ther. 2007;30(6):408–418. doi: 10.1016/j.jmpt.2007.04.013. [DOI] [PubMed] [Google Scholar]
- 14.Thiel HW, Bolton JE, Docherty S, Portlock JC. Safety of chiropractic manipulation of the cervical spine: a prospective national survey. Spine. 2007 Oct 1;32(21):2375–2378. doi: 10.1097/BRS.0b013e3181557bb1. discussion 2379. [DOI] [PubMed] [Google Scholar]
- 15.Lee KP, Carlini WG, McCormick GF, Albers GW. Neurologic complications following chiropractic manipulation: a survey of California neurologists. Neurology. 1995 Jun;45(6):1213–1215. doi: 10.1212/wnl.45.6.1213. [DOI] [PubMed] [Google Scholar]
- 16.Haldeman S, Carey P, Townsend M, Papadopoulos C. Clinical perceptions of the risk of vertebral artery dissection after cervical manipulation: the effect of referral bias. Spine J. 2002 Sep-Oct;2(5):334–342. doi: 10.1016/s1529-9430(02)00411-4. [DOI] [PubMed] [Google Scholar]
- 17.Stevinson C, Ernst E. Risks associated with spinal manipulation. Am J Med. 2002 May;112(7):566–571. doi: 10.1016/s0002-9343(02)01068-9. [DOI] [PubMed] [Google Scholar]
- 18.Tuchin P. A replication of the study ‘Adverse effects of spinal manipulation: a systematic review’. Chiropr Man Therap. 2012;20(1):30. doi: 10.1186/2045-709X-20-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Carlesso LC, Gross AR, Santaguida PL, Burnie S, Voth S, Sadi J. Adverse events associated with the use of cervical manipulation and mobilization for the treatment of neck pain in adults: a systematic review. Man Ther. 2010 Oct;15(5):434–444. doi: 10.1016/j.math.2010.02.006. [DOI] [PubMed] [Google Scholar]
- 20.Sran MM, Khan KM, Zhu Q, McKay HA, Oxland TR. Failure characteristics of the thoracic spine with a posteroanterior load: investigating the safety of spinal mobilization. Spine (Phila Pa 1976) 2004 Nov 1;29(21):2382–2388. doi: 10.1097/01.brs.0000143110.59837.f2. [DOI] [PubMed] [Google Scholar]
- 21.Symons BP, Leonard T, Herzog W. Internal forces sustained by the vertebral artery during spinal manipulative therapy. J Manipulative Physiol Ther. 2002 Oct;25(8):504–510. doi: 10.1067/mmt.2002.127076. [DOI] [PubMed] [Google Scholar]
- 22.Herzog W. The biomechanics of spinal manipulation. J Bodyw Mov Ther. 2010 Jul;14(3):280–286. doi: 10.1016/j.jbmt.2010.03.004. [DOI] [PubMed] [Google Scholar]
- 23.Powell FC, Hanigan WC, Olivero WC. A risk/benefit analysis of SMtherapy for relief of lumbar or cervical pain. Neurosurgery. 1993 Jul;33(1):73–78. doi: 10.1227/00006123-199307000-00011. discussion 78–79. [DOI] [PubMed] [Google Scholar]
- 24.Centers for Medicare and Medicaid Services. Chiropractic Billing Guide. NHIC Corp; Hingham, MA: Apr, 2013. [Google Scholar]
- 25.Hebert JJ, Stomski NJ, French SD, Rubinstein SM. Serious Adverse Events and Spinal Manipulative Therapy of the Low Back Region: A Systematic Review of Cases. J Manipulative Physiol Ther. 2013 Jun 17;pii doi: 10.1016/j.jmpt.2013.05.009. S0161-4754(13)00068-7. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 26.Wang HH, Zhan HS, Zhang MC, Chen B, Guo K. [Retrospective analysis and prevention strategies for accidents associated with cervical manipulation in China] Zhongguo Gu Shang. 2012 Sep;25(9):730–736. [PubMed] [Google Scholar]
- 27.Rubinstein SM. Adverse events following chiropractic care for subjects with neck or low-back pain: do the benefits outweigh the risks? J Manipulative Physiol Ther. 2008 Jul-Aug;31(6):461–464. doi: 10.1016/j.jmpt.2008.06.001. [DOI] [PubMed] [Google Scholar]
- 28.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83. doi: 10.1016/0021-9681(87)90171-8. [DOI] [PubMed] [Google Scholar]
- 29.Whedon JM, Song Y, Lurie J. 141st Annual Meeting of the American Public Health Association. Boston, MA: 2013. Likelihood of vertebrobasilar stroke following chiropractic SMin US adults aged 65–99 with neck pain. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.